


Abstract
This study aimed to assess the incidence of unintentional injuries presented in general practice, and to identify children at risk from experiencing an unintentional injury. We used the data of all 0–17-year-old children from a representative survey in 96 Dutch general practices in 2001. We computed incidence rates and multilevel multivariate regression analysis in different age strata and identified patient and family characteristics associated with an elevated injury risk. Nine thousand four hundred and eighty-four new injury episodes were identified from 105 353 new health problems presented in general practice, giving an overall incidence rate of 115 per 1000 person years (95% confidence interval [CI] = 113 to 118). Sex and residence in rural areas are strong predictors of injury in all age strata. Also, in children aged 0–4 years, a higher number of siblings is associated with elevated injury risk (≥3 siblings odds ratio [OR] = 1.57, 95% CI = 1.19 to 2.08) and in the 12–17-year-olds, ethnic background and socioeconomic class are associated with experiencing an injury (non-western children OR = 0.67, 95% CI = 0.54 to 0.81; low socioeconomic class OR = 1.39, 95% CI = 1.22 to 1.58). Unintentional injury is a significant health problem in children in general practice, accounting for 9% of all new health problems in children. In all age groups, boys in rural areas are especially at risk to experience an injury.
INTRODUCTION
It is estimated that one in four children receives medical attention for an injury each year, in either primary or secondary care.1-3 Studies in emergency departments have provided some insight in to the determinants associated with injuries in children presented. However, surprisingly few studies on childhood injuries have been performed in primary care.3,4
The objective of this study is to estimate the incidence of childhood injuries presenting in primary care and to identify determinants of children at risk for injuries.
METHOD
Second National Survey of General Practice
Data of children aged 0–17 years were extracted from the second Dutch National Survey of General Practice performed in 2001. The participating practices were representative for Dutch GPs and the Dutch population.5 During 12 months, 195 GPs in 104 practices registered all physician–patient contacts and coded all health problems presented within a consultation by using the International Classification of Primary Care (ICPC).6 All visits concerning the same health problem were linked into the same episode. For the present study, morbidity data from of the practices were excluded due to insufficient quality of the data.
Baseline characteristics of the study population such as age, sex and family composition were derived from practice files. Other characteristics (such as, ethnic background and socioeconomic characteristics) were obtained by postal questionnaire.
Extraction of diagnoses related to accidents and unintentional injuries
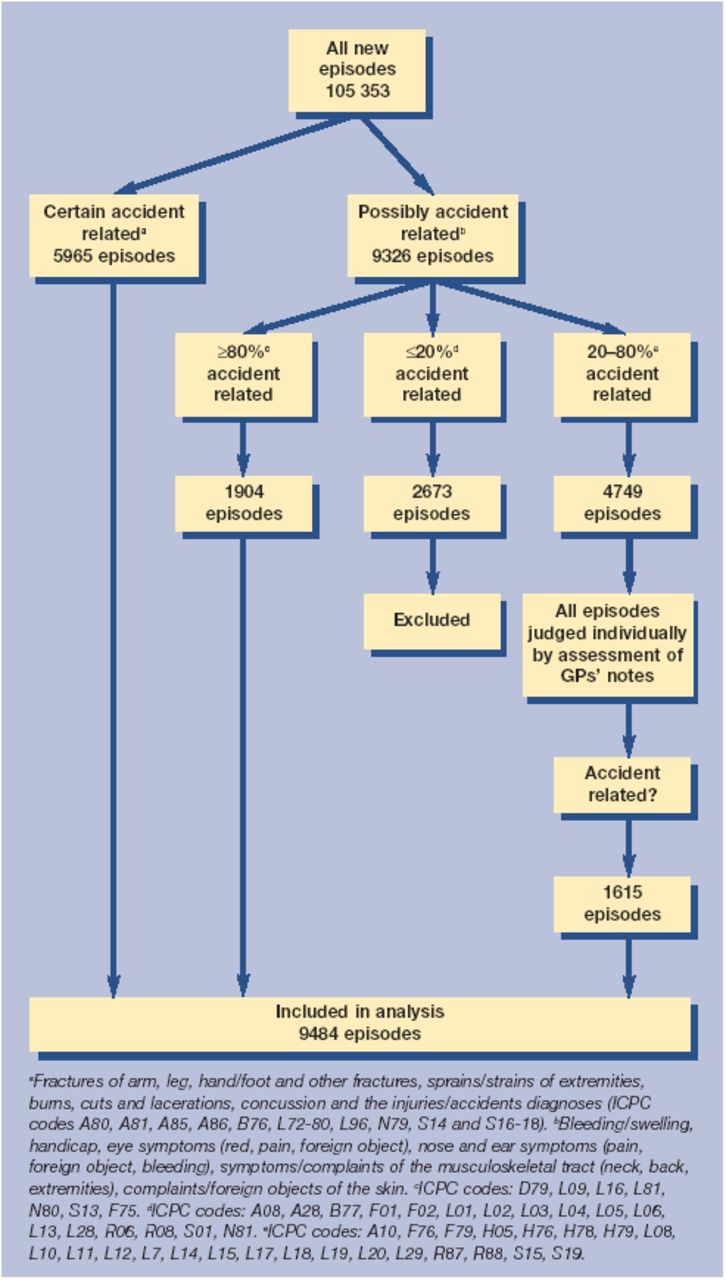
Unintentional injury is defined as all disability which occurs under accidental circumstances.7 We selected all possible injury-related ICPC codes of all children and categorised the diagnoses into those we considered to be probably caused by an accidental injury, and those possibly related to an accidental injury. All probable injury-related diagnoses were included in the analysis. Of the possible accident-related diagnoses, a random sample of 10% of the free-text notes in the electronic patient records was examined to assess whether the health problem was caused by an accident. If less than 20% of the sample for each diagnosis was considered to be an accidental injury, all these diagnoses were excluded from the analysis, Similarly, if more than 80% of these diagnoses were considered to be accidental injuries, all diagnoses were included in the analysis. Notes of all other diagnoses (20–80% accident-related) were examined per patient in the electronic patient files and included in the analysis only if related to an accident. If there were no notes concerning that diagnosis (occurring in approximately 20%) the case was excluded from the analysis (Figure 1).
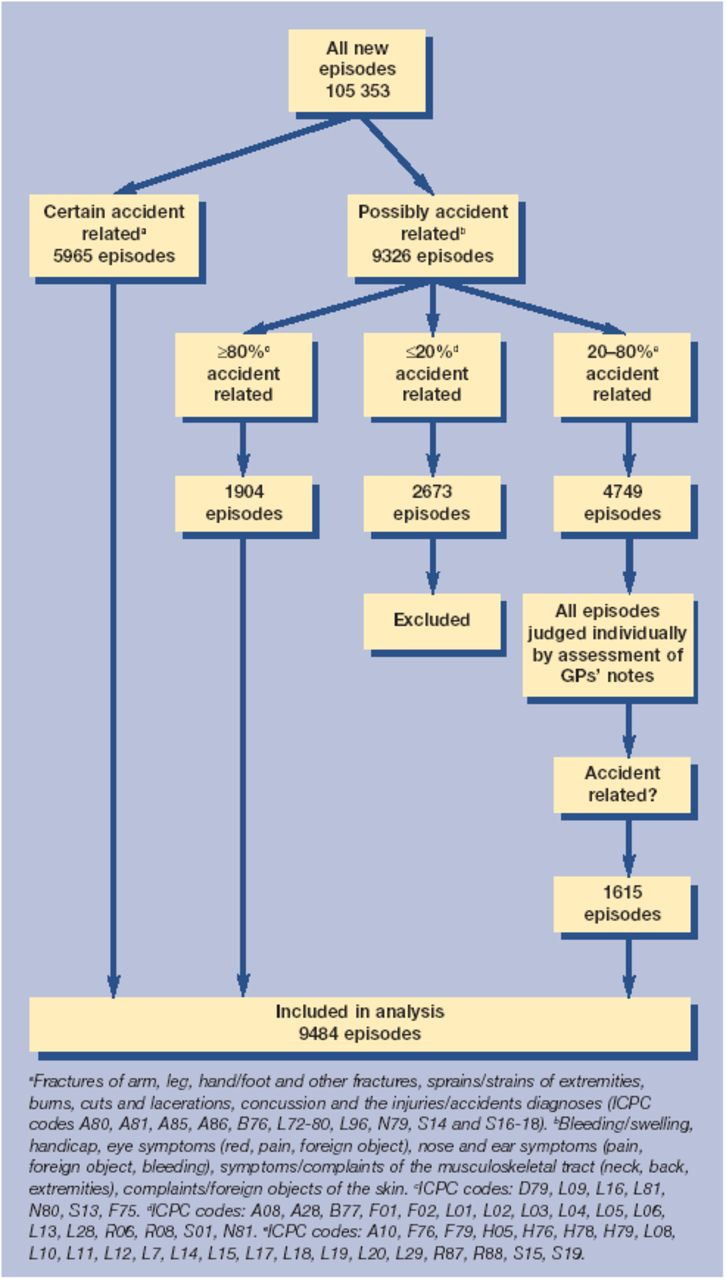
Flowchart of extraction of diagnoses.
How this fits in
At least half of all injuries in children that seek medical attention are handled by GPs, but few studies on childhood injuries have been performed in primary care. Unintentional injury is a significant health problem in children in general practice, accounting for 9% of all new health problems in children. In all age groups, boys in rural areas are especially at risk to experience an injury.
Analysis
All analyses were performed in age strata according to school ages (0–4 years; 5–11 years; 12–17 years). Incidence rates (number of new episodes divided by number of person years) and confidence intervals (considering a Poisson distribution) were calculated. We used a multilevel multivariate logistic regression model to determine which child and family characteristics were associated with experiencing an injury. The characteristics that were associated with experiencing injuries in the univariate analyses (with cut-off point P<0.05) were entered into the multivariate model to adjust for the other characteristics (SPSS version 11.0, SAS 8.2).
RESULTS
The response rate ranged from 70–100% for the different variables, the lowest for ethnic background and socioeconomic variables. Eighty-two thousand and fifty-three children (aged 0–17 years) presented with 105 353 new episodes of disease. In total, 9% were unintentional injuries (9484/105 353). The overall incidence rate (IR) was 115 per 1000 person years. The IR was highest in children aged 12–17 years (Table 1). Figure 2 shows the types of injuries and differences per age group; 29.5% of all injuries involve skin injuries (for example, lacerations and cuts) and incidence rates are highest in the 0–4-year-olds. Sprains and strains, account for 15% of all injuries.

{kind=link}
{kind=link}
Types of injury stratified by age category.
Incidence rates of injuries presented to GPs by age category.
In Table 2 results of the multilevel univariate and multilevel analysis show that male sex and living in a rural residence were associated with an elevated risk of injury in age strata. In children aged 0–4 years, having three or more siblings was also associated with an elevated injury risk. In children aged 12–17 years, low socioeconomic class and Western background were also independently associated with an elevated risk of childhood injury.
Characteristics associated with childhood injury, stratified by age category.
DISCUSSION
This is the first episode-based representative study to provide reliable incidence rates for unintentional injuries in general practice. We found an overall incidence rate of 115 per 1000 people. This is comparable with the results of Hambidge et al, who found an injury-related visit rate of 138 per 1000 people in primary care in the US.4 However, they did not account for multiple visits concerning the same injury episode. Other studies were performed in emergency department settings or based on retrospective questionnaire surveys, the latter susceptible to recall and selection bias.8 Most paediatric injuries in general practice were skin injuries and sprains/strains of extremities, which has also been reported by others.1,4
Residence in a rural area is the most frequently occurring independent risk factor for experiencing childhood injury in all age groups. Although not completely clarified, this finding is consistent with the results of others.4 It is possible that, due to a higher density of emergency departments in urban areas, less severely injured children are treated directly in secondary care compared with rural areas. Another explanation is that rural areas foster a higher level of proneness to accidents.
Compared with others, the socioeconomic gradient is less clear in our study.9 Explanations for this could be that, in the Netherlands, there are smaller socioeconomic class differences regarding access to primary care, or other studies may have suffered from a selective response to the health questionnaires on which their estimates were based. From school age onwards, western children are more at risk of injuries than non-western children. Another Dutch study has hypothesised that non-western children participate less in sports, thus lowering their injury risk.10
In their study in Leicester, UK, Tobin et al found that, compared to other ethnic groups, South Asian children were less likely to utilise hospital services as a result of an accident.11
Inevitably there is some misclassification of injuries. We estimate that this error is approximately 4%, since up to 19% of the diagnoses in the >80% group may be mistakenly classified as an unintentional injury. Also, incidence rates are most likely to be underestimated in general practice, because we excluded diagnoses where, besides the diagnosis, no other information was available in the patient record of the 20–80% injury-related group. If all of these had in fact been accidental injuries (20% of the 3135 excluded episodes from this group) the incidence rate would have risen to approximately 123 per 1000 people.
When measuring injuries in a primary care setting, there is always some overlap with injuries encountered in emergency departments. We found that 434 (4.5% of all injuries) of the injury-related diagnoses were referred to specialists. Theoretically, it is possible that the GP did not treat these children in their surgery, but that children were treated directly in a hospital and that specialists requested a referral in retrospect. Furthermore, we had no information on circumstances and severity of injuries, which is an important drawback in our study.
Unintentional injuries treated in general practice are an important childhood health problem in primary care. Research has shown that unintentional injuries in children may be preventable, for example by GPs' safety advice combined with easy access to safety equipment.12 Western boys living in rural areas could be targeted when considering implementing preventative measures.
Notes
Ethics committee
The Ethics Committee of NIVEL approved the study
Competing interests
None.
- Received April 9, 2004.
- Revision received June 23, 2004.
- Accepted September 13, 2004.
- © British Journal of General Practice, 2005.
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

