


Abstract
Background Most blood pressure recordings end with a zero end-digit despite guidelines recommending measurement to the nearest 2 mmHg. The impact of rounding on management of cardiovascular disease (CVD) risk is unknown.
Aim To document the use of rounding to zero end-digit and assess its potential impact on eligibility for pharmacologic management of CVD risk.
Design of study Cross-sectional study.
Setting A total of 23 676 patients having opportunistic CVD risk assessment in primary care practices in New Zealand.
Method To simulate rounding in practice, for patients with systolic blood pressures recorded without a zero end-digit, a second blood pressure measure was generated by arithmetically rounding to the nearest zero end-digit. A 10-year Framingham CVD risk score was estimated using actual and rounded blood pressures. Eligibility for pharmacologic treatment was then determined using the Joint British Societies' JBS2 and the British Hypertension Society BHS–IV guidelines based on actual and rounded blood pressure values.
Results Zero end-digits were recorded in 64% of systolic and 62% of diastolic blood pressures. When eligibility for drug treatment was based only on a Framingham 10-year CVD risk threshold of 20% or more, rounding misclassified one in 41 of all those patients subject to this error. Under the two guidelines which use different combinations of CVD risk and blood pressure thresholds, one in 19 would be misclassified under JBS2 and one in 12 under the BHS–IV guidelines mostly towards increased treatment.
Conclusion Zero end-digit preference significantly increases a patient's likelihood of being classified as eligible for drug treatment. Guidelines that base treatment decisions primarily on absolute CVD risk are less susceptible to these errors.
- blood pressure determination
- data quality
- decision support systems
- evidence-based medicine
- practice guidelines
- professional practice
- risk assessment
INTRODUCTION
It has long been recognised that there is significant imprecision in measuring and recording blood pressure.1,2 Although most clinical practice guidelines have protocols for measurement, and recommend reading and recording to the nearest even number,3–5 monitoring for quality assurance is not routine and it is unclear how this imprecision has an impact upon assessment or treatment of cardiovascular disease (CVD) risk.6
Recent CVD risk management guidelines incorporate a combination of absolute CVD risk and individual risk factor-level thresholds. The absolute risk of CVD events is estimated using risk-prediction algorithms utilising multiple risk factors.7–9 Two UK guidelines that include both individual CVD risk factor and absolute CVD risk thresholds are the 2004 British Hypertension Society guidelines (BHS–IV)10 and the 2005 Joint British Societies' guidelines on the prevention of cardiovascular disease (JBS2).11
The prevalence of zero end-digit preference in primary care using data generated within PREDICT™-CVD, a web-based electronic CVD risk assessment and decision-support system used in primary care practices in New Zealand, is described in this study. The potential impact of rounding upon pharmacologic treatment decisions using criteria recommended in the 2004 BHS–IV and 2005 JBS2 guidelines is then assessed.
How this fits in
In this and other studies, over 60% of blood pressures measured in primary care are recorded with a zero end-digit when auscultatory sphygmomanometers are used. The impact of end-digit preference on classification for pharmacologic treatment for cardiovascular risk is not well described. End-digit preference errors significantly increase the likelihood a patient will be classified for pharmacologic treatment in guidelines that base treatment recommendations primarily on blood pressure thresholds. In contrast, this error has less effect on eligibility for treatment when decisions are based on absolute cardiovascular risk.
METHOD
An integrated web-based decision support system for assessing and managing CVD risk (PREDICT™–CVD) was provided free of charge to primary care practices in a large general practice organisation (ProCare Limited) in Auckland, New Zealand.12 PREDICT™–CVD enables GPs and practice nurses to rapidly estimate a patient's overall CVD risk, and also provides patient-specific treatment recommendations during the consultation, based on national guidelines developed using estimated overall CVD risk.3 All risk profiles are automatically and anonymously stored for research purposes using nationally-agreed encryption algorithms and systems approved by the Auckland Ethics Committee.
For this study, the first risk profile was extracted for every person opportunistically risk assessed in routine practice settings between August 2002 and August 2005. Systolic (SBP) and diastolic (DBP) blood pressure measures were classified according to whether the final digit was zero or not.
Each patient's 10-year absolute risk of a CVD event was estimated by applying the ‘any CVD’ equation derived from the Framingham Heart Study.7 The risk score is based on seven risk factors: age (years); sex; SBP; cigarette smoking (yes/no); total cholesterol: high density cholesterol (HDL) ratio; current diabetes (yes/no); and left ventricular hypertrophy (LVH) confirmed by electrocardiography. In PREDICT™–CVD, LVH was not collected and was assumed to be absent. Student's t-tests and χ2-square tests were used to test differences in risk factors between the groups with and without a zero end-digit in SBP. Throughout, risk was assessed and patients were classified regardless of any current treatment.
For the subset of patients whose original blood pressure was measured without a zero end-digit, a second rounded blood pressure measure was generated by arithmetically rounding their actual blood pressures to a nearest zero end-digit (systolic and diastolic): end-digits six to nine were rounded upwards, digits one to four downwards, and fives were randomly assigned with equal probability either upwards or downwards. This was done to simulate rounding in routine practice. The Framingham risk score was then recalculated with the arithmetically rounded SBP. The effect on the mean Framingham risk scores (original versus simulated rounding), was tested with a paired t-test to assess whether use of zero end-digit introduced bias in recorded risk. Patients with a history of CVD were excluded from these analyses as the Framingham scores apply only to those who had no prior history of CVD.
To compare the effect of simulated rounding on management for primary CVD prevention, the first strategy assumed that pharmacologic treatment is appropriate for patients with a 10-year Framingham CVD risk score of 20% or more. The calculated Framingham risk score was used to classify each patient accordingly, using first the original then the simulated rounded blood pressures. Patients were then classified according to their eligibility for pharmacologic treatment under the JBS2 and the BHS–IV criteria,10,11 also using the original and then simulated blood pressures, as follows.
BHS–IV classifies patients with blood pressure over 160/100 mmHg as eligible for blood pressure lowering therapy, and those below 140/90mmHg as ineligible for treatment, regardless of other risk factors or absolute risk. Those with intermediate blood pressure levels have their absolute CVD risk assessed using the Framingham equation, and if the estimated 10-year risk is over 20%, blood pressure lowering therapy is recommended.10
In the JBS2 guideline, patients with blood pressure ≥160/100 mmHg, total cholesterol: HDL cholesterol ratio ≥6.0; or diabetes are all eligible for blood pressure lowering therapy. Other patients are also eligible if their calculated 10-year Framingham CVD risk is 20% or more.11
The resulting changes in treatment classification are described in two ways. The first is based on a comparison of the original and the simulated rounding classification and is generalisable to those patients measured with rounding. In the second, the impact of rounding to zero for the whole cohort is estimated. The cohort was divided into three component groups: those not measured with zero who after rounding would remain in the same treatment group because they were not rounded; those regarded as ‘true zeroes’, (one in five of the whole cohort); and finally the remainder, the ‘non-true zeroes’, who can be regarded as having been already rounded, and were apportioned to a simulated ‘original’ treatment classification based on the proportions observed in the simulated rounding exercise. Before and after tables were completed and the results summed to obtain the final figures.
RESULTS
Blood pressure records for 23 676 people were obtained from 406 GPs and 89 practice nurses. Mean age was 53.8 years for men (n = 13 396), and 57.5 years for women (n = 10 280).
A zero end-digit was recorded in 64.4% (15 254) of the SBP and 61.8% (14 673) of the DBP records (Table 1) both clearly exceeding an expected percentage of around 20% if recorded to the nearest even number as recommended. Almost half (11 144/23 676, 47.1%) of all blood pressures were recorded with a zero end-digit for both SBP and DBP (Table 1). After zero, the next most commonly reported blood pressure end-digit was five. Figure 1 shows that the proportion of blood pressures recorded with zero end-digit was high across the entire blood pressure ranges. The distribution of those recorded without a zero end-digit was symmetrical, but those recorded with zero were right skewed.

Distribution of (a) systolic and (b) diastolic blood pressure in 23 676 patients.
Cross-tabulation of systolic versus diastolic end-digits (n = 23 676).
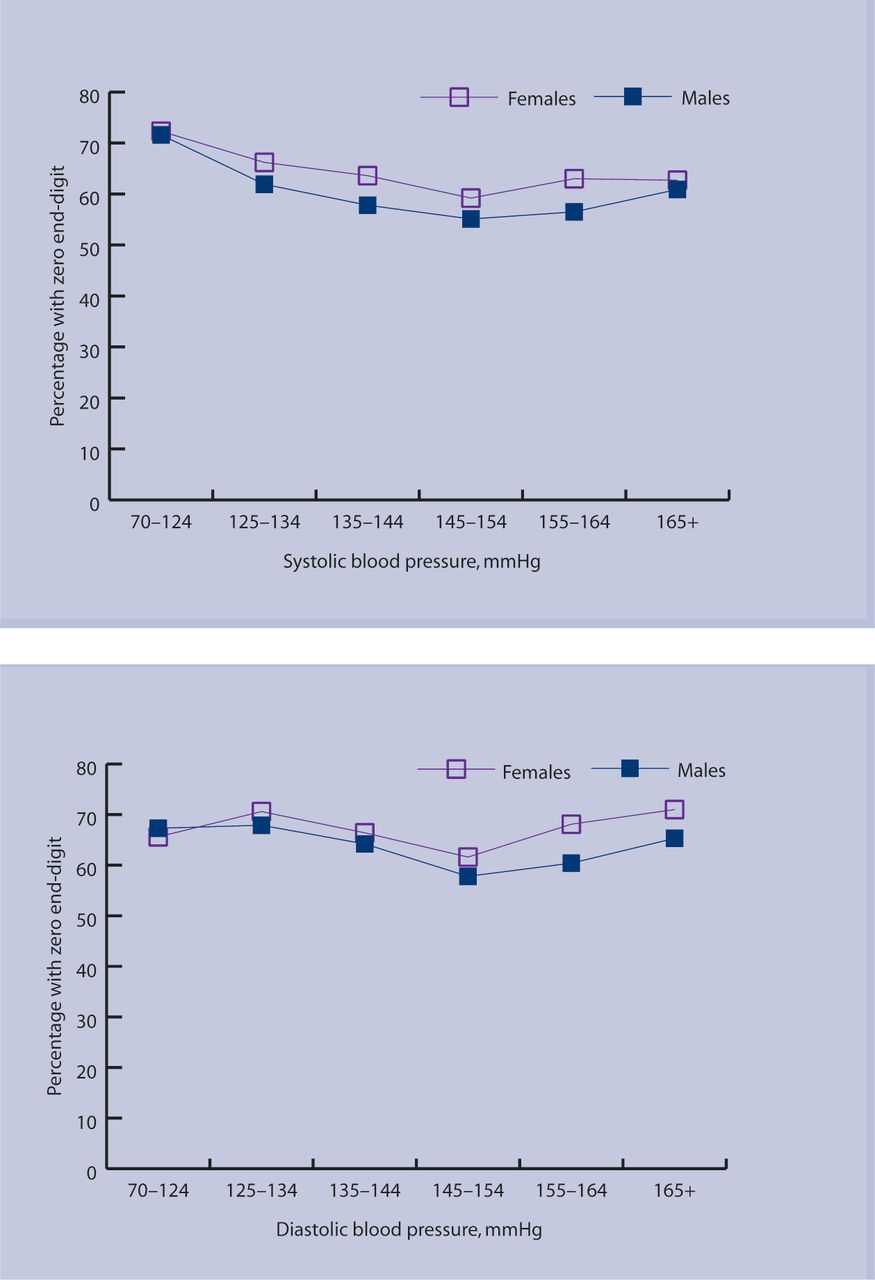
There were no clinically important differences between participants whose blood pressure was recorded with and without a zero end-digit, although many of these differences were statistically significant because of the large sample size (Table 2). For both SBP and DBP, the proportion with zero end-digit varied across the blood pressure range in a slightly U-shaped relationship (Figure 2).

{kind=link}
{kind=link}
Proportion of (a) systolic and (b) diastolic blood pressure measured with zero end-digit.
Demographic and risk factors, by systolic blood pressure end-digit.
Mean (standard deviations) blood pressures were 134 mmHg (18.4) for SBP, and 82 mmHg (10.6) for DBP. Those recorded with a zero end-digit in SBP were lower on average, by 3.0 mmHg SBP, than those recorded without a zero end-digit (P<0.001).
The corresponding difference for DBP was 1.0 mmHg (P<0.001). Mean Framingham 10-year CVD risk scores were 7.0% (6.3) and 7.1% (6.2) in those with and without zero end-digit in SBP (P = 0.33).
After excluding patients with a history of cardiovascular disease, or whose SBP was recorded with a zero end-digit, there were 7542 patients whose original blood pressures were recorded with non-zero end-digit available for simulating a rounded SBP and DBP level. When recalculated with simulated rounding of SBP as described, mean Framingham 10-year CVD risk scores were 0.16% higher than with the original blood pressures (paired t-test P<0.001).
Table 3 illustrates the potential impact of rounding by classifying these 7542 patients as eligible or ineligible for pharmacologic treatment using original blood pressures and simulated rounded blood pressures. Table 3 also shows that of the patients who would be eligible for treatment because their risk was ≥20% based on original blood pressures, as a result of rounding, 94 would be misclassified as <20% and therefore not eligible for pharmacologic treatment. Conversely, 88 with an original risk score of <20% would be misclassified as needing treatment. Therefore, 182 (94 + 88 = 182, or 2.4%) of these patients would be misclassified if an absolute CVD risk threshold alone was used, that is, one patient in 41 would be misclassified.
Classification into risk/treatment group, before and after simulated rounding of blood pressure according to overall Framingham CVD risk, and BHS–IV and JBS2 guidelines.
Also illustrated in Table 3 is the comparable impact on these patients of their simulated rounding under the other two guidelines. Misclassification occurred for 633 (8.4%) and 395 (5.2%) under the BHS–IV and JBS2 guidelines respectively, and consequently one in 12 patients would be misclassified for treatment under the BHS–IV guidelines, and one in 19 under JBS2.
The impact of rounding on the cohort as a whole was most marked if BHS–IV is used; 3.4% were misclassified, mostly because the proportion for treatment changed from 21.5% to 24.4%, a relative increase of 13.6%. Under JBS2, 2.4% would be misclassified, changing the proportion for treatment from 36.9% to 38.5%, a 4.6% relative increase. Differences were much smaller with the Framingham rule under which 1.3% were misclassified, the proportion for treatment changed from 32.6% to 33.0%, a 0.9% relative increase.
DISCUSSION
Summary of main findings
Zero end-digit preference in blood pressure recording is the norm rather than the exception in routine primary care practice, with almost two-thirds of SBP measurements recorded with zero as the end-digit. Statistically, if blood pressures are measured to the nearest even number as recommended by most national guidelines, the expected prevalence of a zero end-digit is around 20%. Further, the high proportion of patients with both a SBP and DBP measured with a zero end-digit (almost 50%) demonstrates that clinicians commonly round both SBP and DBP, although statistically the expected prevalence is 4% (0.2 × 0.2 = 0.04).
Rounding in those without a zero end-digit is potentially associated with treatment reclassification in either direction. When using 20% 10-year Framingham CVD risk as the only classification threshold, the number of patients reclassified for treatment was similar to those reclassified as not for treatment. That is, the effect of the simulated rounding process was symmetric. In contrast, the results under the two British guidelines were markedly asymmetric, particularly BHS–IV. Because the BHS–IV and JBS2 guidelines use treatment thresholds defined with zero end-digits, many more patients who were not eligible for treatment were classified for treatment than the opposite. The impact on the patients rounded to zero showed one in 12 would be misclassified using the BHS–IV criteria, one in 19 using the JBS2 criteria, but one in 41, when the only threshold was a Framingham CVD risk score of 20%.
To generalise to the whole cohort, it was necessary to take account of the approximate 20% of patients in whom the true SBP (if measured to the nearest 2 mmHg) will have a zero end-digit and therefore will be susceptible to rounding errors only if DBP is also rounded. Analyses that allowed for this 20% and estimated the proportion misclassified in the whole cohort showed a relative increase in treatment (and presumably costs), of 14% under BHS–IV, 5% under JBS2, and 1% under the Framingham rule.
Strengths and limitations of the study
This is a large, recent cohort of patients drawn from more than 400 GPs in a population where guidelines for the management of hypertension are well established. Data were used from routine primary care practices measured by practitioners with no additional training in measurement, and no protocols, monitoring, or other constraints upon practice that usually apply in research settings. The study population comprised of patients assessed opportunistically as part of routine primary care and therefore were not a representative sample of any geographically defined population. Nevertheless, the patients were typical of those for whom GPs are assessing CVD risk.
The findings of this study are likely to be generalisable to other primary care settings where blood pressure is routinely measured.
As all risk assessments were undertaken using PREDICT™–CVD, a standardised electronic decision-support system integrated with the practitioners' computer-based medical records, data consistency and completeness was high. Included in the Framingham formula is ECG-classified LVH, It was not recorded in PREDICT™–CVD as it is rare, not commonly measured in primary care practice in New Zealand, and is often associated with a prior history of CVD. It was therefore assumed that none of the patients in this study had ECG-classified LVH. Data for all other variables required were available, so it possible to estimate absolute CVD risk and to assess the potential impact of zero end-digit preference on clinical management in virtually all patients.
It was also assumed that the blood pressure measures were taken from a single measurement during the first assessment. In contrast, the Framingham equation, the guidelines, and clinical management, require ‘usual’ blood pressure. Common sense suggests that the latter is more likely to be rounded, but even so, treatment decisions are affected.
Although the type of measurement device used was not recorded, standard mercury auscultatory sphygmomanometers are almost universal in these practices (personal communication based on Janine Bycroft, unpublished survey data, 2007). Internationally, blood pressure is increasingly being measured with electronic instruments that virtually eliminate rounding errors,13 although it is noted that the 2006 NICE guidelines describe how to measure blood pressure using a traditional sphygmomanometer.5
It is likely that rounding introduces more error than that introduced by the use of electronic machines. To assess the impact of rounding on risk and treatment assessment, simulated rounded values were created from the non-zero end-digit records. When the rounding of blood pressures was simulated it was assumed that clinicians recording zero end-digits did so by rounding values with end-digits of six through nine upwards, one through four downwards, with the end-digit five rounded randomly. While standard practice may differ a little from the arithmetically ‘rounded’ estimates, it is unlikely to change the substance of the conclusions.
It was assumed that individuals with a non-zero end-digit had their blood pressure recorded more accurately, which seems a reasonable assumption as there is little evidence of rounding to any other end-digit (Table 1). It was also assumed that the subset of participants with blood pressure recorded with a non-zero end-digit (7542 of 21 020 with no history of CVD), were similar to those with a zero end-digit recorded. This appears to be reasonable given the similarities between the groups (Table 2), the small differences in mean blood pressures that are likely to arise mainly from the skewed nature of the distribution, and the very similar mean Framingham risk scores.
The two British guidelines were chosen for comparison purposes because they were published within a 2-year period, yet differed in that the key determinant of treatment decisions in the BHS–IV guideline were blood pressure thresholds. However, the treatment decisions in the JBS2 guideline were more driven by absolute CVD risk. The recently published NICE guideline revisions are similar to the BHS–IV guidelines, as is the US seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure (JNC 7 guidelines).14 All these are more susceptible to rounding errors than the JBS2 guidelines and those from New Zealand.3
Comparison with existing literature
The prevalence of 64% with zero end-digit in this study is somewhat lower than the 75–90% found in audits of some general practices.15–18 A much lower proportion of 40% was found in a hypertension clinic where blood pressure is the main focus of care.19 Three previous studies have drawn attention to the problems of treatment thresholds with zero end-digits. In a Canadian prenatal clinic, redefining a treatment threshold by just 1 mmHg, from SBP >140 mmHg to SBP ≥140 mmHg, doubled the proportion of patients who were regarded as requiring treatment from 13% to 26%.20 In a UK study of elderly patients diagnosed as having hypertension, 26% were regarded as controlled if the cut-off was <160/90 mmHg, but this more than doubled to 62% if ≤160/90 mmHg.17 In a UK case-control study based in general practice, the impact of terminal digit preference on disease outcomes was associated with increased mortality.21
Implications for future research or clinical practice
Rounding blood pressure measurements to a zero end-digit appears to be the norm in primary care practice in New Zealand. It is of concern that rounding may substantially increase the likelihood a patient is classified as requiring pharmacologic treatment, usually for life.
Historically, treatment with blood pressure lowering drugs was recommended for patients if ‘hypertensive’, as defined by systolic and diastolic blood pressure thresholds.22,23 Where a threshold is defined by a number ending with zero in either SBP or DBP, those with blood pressure recorded at the threshold may have true values ranging upwards or downwards by approximately 5 mmHg.
This study has shown that blood pressure thresholds defined with zero end-digits lead to misclassification in treatment eligibility, mostly towards treatment. Treatment recommendations based primarily on individual risk factor thresholds, such as the BHS–IV guidelines, are significantly more susceptible than guidelines based primarily on absolute CVD risk. Guidelines that use absolute risk thresholds rather than individual risk factor thresholds are much less susceptible to misclassification and should be encouraged.
Acknowledgments
We acknowledge ProCare Health Ltd, a Primary Health Care Organisation, and the GPs who belong to it, for access to the patient data collected. Joanna Broad drafted this paper during Women Writing Away, an academic writers' retreat. The National Heart Foundation of New Zealand provided salary support for Sue Wells during the study. Chieh-En Thomas Huang undertook preliminary analyses. Tania Riddell, Alistair Stewart, and Joanna Stewart provided helpful comments
Notes
Funding body
Funding for the study was provided under Project Grant 03/183 from the Health Research Council of New Zealand
Ethics committee
Ethics approval was provided by the Auckland Ethics Committee (AKY/03/12/314)
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received January 4, 2007.
- Revision received March 1, 2007.
- Accepted June 14, 2007.
- © British Journal of General Practice, 2007.
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

