


Introduction
The Harveian Oration, an annual event at the Royal College of Physicians (RCP), was established by William Harvey in 1656. In October 2011, Iona Heath, President of the Royal College of General Practitioners, was invited to speak — the second GP ever to do so in over 350 years. We reflect here upon some of the important issues discussed within this oration, but also urge the reader to seek out and enjoy the original and inspiring text. At its centre is her invitation to expand our repertoire of care and kindness towards patients. Harvey determined the oration should be delivered on the Feast Day of St Luke’s (patron saint of the physician). Iona pays tribute to the relevance of St Luke’s gospel as a source of miracles and parables concerning healing, kindness, and concern for the poor: an approach this piece itself replicates.
In her Oration ‘Divided we fail’ Iona draws upon experience, literature, and research, including her 35 years of clinical practice.1 She uses a multifaceted lens to examine the professional work of doctors through a series of dyads. These include the central dyad of medical practice: doctor–patient; the key dyad of the NHS: generalist–specialist; and the Cartesian split of mind–body. These dyads also extend within her text to illness–disease; subject–object; life–death; technis–praxis; and collaboration–competition.
Why dyads? Viewing the world as ‘divided’ facilitates our understanding of relationships. This may invoke ideas of synergy, balance or harmony between component parts:
‘But let there be spaces in your togetherness,
And let the winds of the heavens dance between you.
… And stand together yet not too near together:
For the pillars of the temple stand apart,
And the oak tree and the cypress grow not in each other’s shadow.’
Kahil Gibran On Marriage (1923).
However, Iona also uses dyads to highlight the gaps in practice and the rigid thinking that they can generate. Understanding the relation between dyads has dominated philosophical enquiry from 17th century humanism2 to 21st century feminism.3,4
In focusing on dualism, Iona implicitly draws our attention to power gradients: how one pole of a dyad tends, almost invariably to dominate the other. Iona encourages us to consider the interconnections between poles, to look anew at the key relationships in medicine and appreciate their complementarity to gain a flourishing of the greater whole. Through a combination of poetry and prose she builds a careful argument for holism and coherence, that respects rather than obliterates difference.
Biography or Biology?
Throughout this presentation, Iona highlights the importance of both the patient’s biography and biology within medical practice. Drawing upon evidence rooted in medical science, literature, and poetry, she emphasises the importance of understanding the patient’s past, present, and future narratives. Rather than presenting biology and biography as competing ideologies within the consultation, Iona explores in-depth the relationship and influence between the two.
This connection between life experience and physiology, which has long been articulated within fictional texts, is explained here using Nobel Prize winning research on the physiological effects which violence, trauma, or chronic stress have upon causation of disease and rates of aging.5 Telomere length can serve as a biological marker of a cell’s age.6 Damaged telomeres have been demonstrated in caregivers of people with Alzheimer’s disease,7 mothers of chronically sick children, and sufferers of domestic violence.8 Telomere length is also significantly shorter in those with mood disorders, representing as much as 10 years of premature aging.9 Similarly, lower levels of telomerase (which increases telomere length) have been associated with smoking; and a range of changes from greater abdominal adiposity; raised glucose; and lipids.10 This, Iona argues, is compelling evidence to nurture not only biotechnical advances, but also a complementary biographical understanding of patients, helping to heal the entrenched Cartesian mind–body split.11
Symptoms as Disease or Illness?
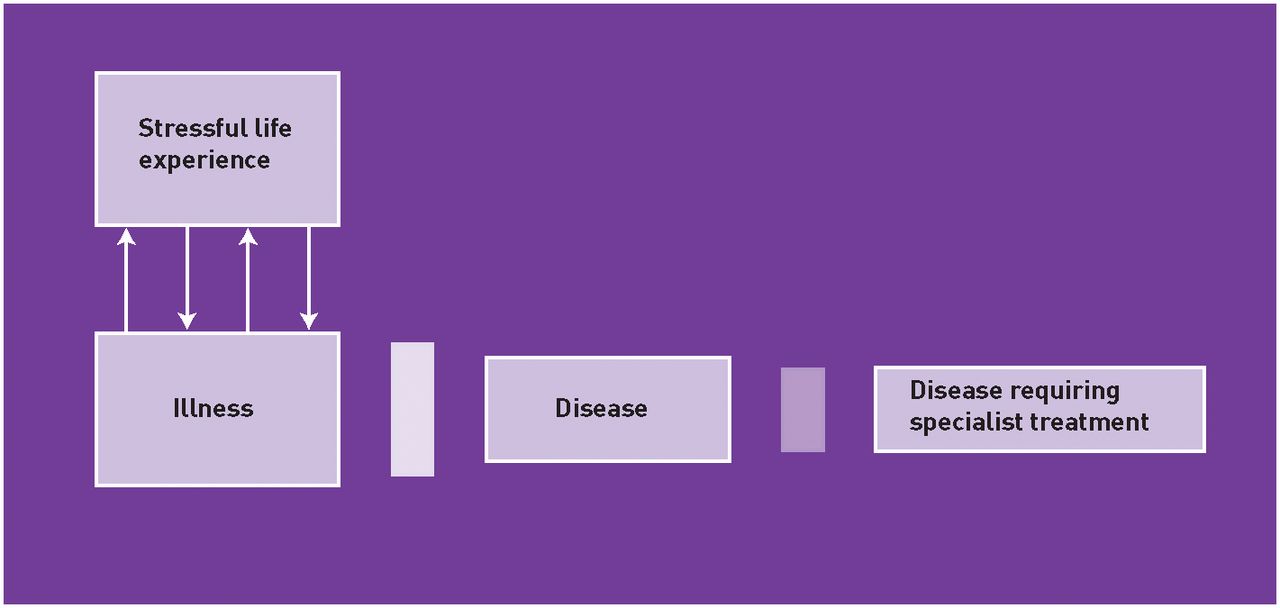
Iona urges us as a medical profession to remain humble about the limitations of our disease-based knowledge and its application. Human suffering (which may or may not be brought to a doctor) might be expressed as ‘illness’: some of which may then represent disease (Figure 1). The work of a GP, she argues, is to negotiate and recognise the boundaries between these symptoms of ‘illness’ and an objective, ‘rational’ disease label, for which subsequent investigation, prognosis, and possible treatment may be available. This involves reconciling of theoretical ‘rules’ with the individual perspectives of patients and doctors.12,13 While many rationing initiatives attempt to limit costs or interventions through focusing upon referral rates at the boundary between ‘disease’ and ‘disease requiring specialist treatment’, Iona argues this junction is too late.
{kind=link}
The borders between illness and disease. Reproduced from: Heath I. Divided we fail: The Harveian Oration 2011. RCP: London, 2011.
Copyright © 2011 Royal College of Physicians. Reproduced with permission.
The crucial step, instead, is to hold effectively the boundary between ‘illness’ and ‘disease’. This limits the exposure of patients to potentially harmful investigations and treatments utilising a clinician’s judgement: confidence or suspicion about the likelihood or presence of disease. Uncertainty always exists surrounding both the limitations of the physician’s own knowledge and the temporal shifts in scientific knowledge between a set of symptoms representing illness, rather than a recognised disease label.14 As demonstrated by the current medicalisation of obesity, these latter shifts from ‘normal’ to ‘abnormal’ or ‘disease’ are not a morally neutral process, but transfer significant societal responsibility onto the medical profession. Most GPs, however, perform daily as best they can a balancing act between their patient’s story or reported experiences and the possibility of currently recognised disease.
This interpretation of the illness–disease model raises several important issues. First, medical knowledge has limitations about its understanding of disease aetiologies, treatments, and prognoses. Diseases may also be experienced in varied ways by different individuals. Similarly, there are myriad conditions for which medicine cannot provide a cure and the doctor instead can helpfully focus no longer upon the biological, but the biographical and its ultimate conclusion, death. The disease–illness dyad is used here then to emphasise the importance of identifying the boundary between illness and disease in order to prevent harm through labelling (or ‘medicalisation’) and the overzealous pursuit of diagnosis and cure.
Objectivity or subjectivity?
The disease–illness dyad is also used in a different way alluding to the shifts in patient-centred communication, through which the subjectivity of the patient is welcomed alongside the doctor’s objective gaze. Iona shares concerns about how the consultation process has been instrumentalised or standardised: turning a way of being into atomised behaviours in checklists for surveys, research, teaching, and assessment.
‘Our meddling intellect
Mis-shapes the beauteous forms of things:
We murder to dissect.’
William Wordsworth The Tables Turned (1798).
Although not explicit, Iona also draws our attention to the neglected subjectivity of the doctor through the work of poet–GP William Carlos Williams and others. As Iona has written elsewhere: doctor–patient dyads often join together and oscillate between the ‘objective’ and ‘subjective’.15 Until we can help future doctors not to perceive themselves as uniquely ‘objective’ in the face of patients’ ‘subjectivity’, we perpetuate a rigid dualism of asymmetric power. We also fail to acknowledge the value of our intuition and our own vulnerability.
Prevention or Cure?
Iona reminds us to be cautious of the appealing ‘preventative’ role now assigned to GPs. Although a few patients are ‘saved’ by screening programmes, many experience subsequent psychological or physical harm. Related, a critical appreciation of statistics is required of studies in order to balance the claims of improved morbidity and mortality with possible effects of lowering diagnostic thresholds (and therefore increasing patient populations defined as ‘having a disease’, usually in milder form). Iona advocates a therapeutic focus upon ‘salutogenesis’ (or coherence of meaning–making), rather than pathogenesis: identifying and supporting patient’s own resources and capacity to create health, rather than concentrating on risks, ill health, and disease.16
Generalism or Specialism?
The relationship between primary and secondary care in this model (Figure 1) is symbiotic not competitive. A GP’s ability to recognise the boundaries between illness and disease and the specialists’ ability to investigate and treat a population of highly selected patients, function only through mutual trust. If a GP cannot willingly admit their limitations to a colleague, while exploiting their expertise elsewhere, this finely tuned arrangement (dependent on human and subjective elements of practice) is unlikely to succeed. While ‘objective’ processes have an important role, the limits of evidence-based medicine, patient-pathways, and protocols in addressing patient’s needs are well documented.17 The ‘protective’ role of GPs in minimising unnecessary exposure of patients to intervention is demonstrated most beautifully by Starfield’s findings that a health system based on strong primary care produces better outcomes at lower cost and with less inequity,18 as well as suggestions that an increase in the number of specialists (relative to generalists) results in increased mortality.19
Past and future
The Oration itself is interwoven with Iona’s kindness and concern for individuals and health care as a whole. To have done this in the halls of the RCP is noteworthy. Iona may even be accused of an act of ‘gentleness’ (or well-judged diplomacy) for describing the accident of history that resulted in the clear separation of generalist from specialist practice in the UK as a ‘gift’; a rather unseemly border skirmish more like! It was, in part, the RCP’s desire to block the establishment of a College of GPs that led to the Medical Act of 1858 and the formation of the General Medical Council (GMC). The resultant structures established the separation described by Stevens:
‘The physician and surgeon retained the hospital [and the student] but the general practitioner retained the patient.’20
This sustained the unhelpful, hierarchical aspects of dyads Iona illuminates for us. What may have happened to the profession as a whole if as well as ‘keeping the patient’ the GPs had also kept a part share in the medical student too, rather than having to wait another 100 years to teach them in our practices (something Iona did in inspiring fashion)?
Iona begins by referring to the influence of her own history and experience upon her reflective insights. Quoting from Mrs Dalloway on the compensation of growing old as being ‘the power of taking hold of experience, of turning it round, slowly in the light’.21 The importance of this past experience on shaping our future role as GPs and relationships with both patients and colleagues is paramount. It may be that one day we will see Iona’s clinical career as spanning a ‘golden era’ of general practice — starting at the time the New GP Charter had bedded in (early 1970s) and closing just before the ‘liberation’ of the NHS (2010).
At one of the most challenging times in the history of the service, the Health and Social Care Bill establishes a revised, formalised divide between colleagues and patients embracing explicit commercial and competitive interaction. Iona asks us to take a ‘united’ view of our patients and our profession — and invokes the need to consider a final dyad together — health care as human right versus health care as commodity. This Oration reminds us that we are the custodians of a system based on equity and social justice. While the qualities and features of general practice Iona highlights may be used by many in their daily practice, this piece makes these qualities explicit in a way that should inform commissioning agendas, medical education, future research, and clinical practice.
Postscript
It is hard not to end with the image of a ladder which Iona has taken down and placed firmly in the RCP bicycle shed before she cycles off home:
Chairman: ‘It has been put to us … that the two branches of the profession, GPs and consultants, are not senior or junior to one another, but they are level. Do you agree with that?’
Lord Moran (former President of the RCP): ‘I say emphatically “No!” Could anything be more absurd? I was Dean at St Mary’s Hospital medical school for 25 years, and all the people of outstanding merit … aimed to get on the staff. There was no other aim and it was a ladder off which some of them fell. How can you say that the people who get to the top of the ladder are the same as those who fall off it? It seems to me so ludicrous.’22
Acknowledgments
With thanks to Iona Heath for permission to share this material and draft review. Thanks also to Andy Haines for reviewing an earlier draft.
Notes
Provenance
Freely submitted; not externally peer reviewed.
Footnotes
‘Divided we fail: The Harveian Oration 2011’ presented by Dr Iona Heath, CBE, FRCP, PRCGP, was presented to the Royal College of Physicians on Tuesday 18 October 2011. Accessible at: www.rcplondon.ac.uk
- © British Journal of General Practice 2012
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

