


In this personal commentary, we will describe the ‘what’, ‘why’, and ‘how’ of a visionary system we believe could improve the diagnosis and management of infectious disease in primary care.
THE CLINICAL PROBLEM (PAST, PRESENT, AND FUTURE)
Consider Ahmed: a 4-year-old brought to see you on Friday evening with a 5-day history of runny nose, chesty cough, fever (described by his mother as severe and not improving), 1/2 normal fluid intake, loose stools, and not eating. The family are exhausted from the sleepless nights, but mostly his mother is worried about the chesty cough and fever, and asks if Ahmed needs antibiotics.
You complete the history — no vomiting, no rash, up-to-date with immunisations, no chronic diseases — and you examine Ahmed. He is listless and looks at you warily with red (conjunctivitis?) eyes while clinging to his mother. His breathing rate is normal (30 breaths per minute) and he does not have any cyanosis, respiratory recession, or rash. He has a temperature of 38.2°C, a pulse of 135 beats per minute, and oxygen saturation of 98%. His peripheries are well perfused with a capillary refill rate of <2 seconds. On auscultation, you hear some moist crackles with expiratory wheezing (bilaterally and not confined to a single zone); and, finally risking his wrath, you check Ahmed’s ears and throat: normal tympanic membranes and some redness of his pharynx, but no pus or enlarged tonsils.
Summing up, you know he has an infectious disease affecting mainly his respiratory tract (coryza, chesty cough, pharyngitis, bronchitis) but also affecting his gastrointestinal tract (diarrhoea); and you know he is moderately unwell. You think a ‘viral illness’ is most likely, but you are concerned not to under-treat a bacterial infection.
MANAGEMENT OPTIONS AND CURRENT GUIDELINES
Your management options are clear: 1) provide symptomatic advice regarding fluids and antipyretics, with the option of asking the out-of-hours service to review in 12 to 24 hours; 2) prescribe antibiotics; and/or 3) arrange secondary care assessment.
National Institute for Health and Care Excellence (NICE) sepsis guidelines1 put Ahmed at moderate risk of sepsis (tachycardia), but you discount sepsis because he has no other features, and you think his tachycardia is due to fever.2 NICE respiratory tract infection guidelines from 2008 recommend immediate antibiotics (or further investigations) for patients ‘systemically very unwell’ or with ‘symptoms and signs suggestive of serious illness and/or complications’.3 NICE pneumonia guidelines4 recommend using C-reactive protein testing in suspected community-acquired pneumonia, but you do not suspect pneumonia (at this stage) and, in any case, you do not have the necessary point-of-care testing equipment.
You feel an antibiotic could be justified by NICE criteria (‘at risk of pneumonia’),3 but you are aware that a high proportion of antibiotic prescribing is unnecessary5 and contributes to antimicrobial resistance;6,7 and you feel uncomfortable ‘treating blind’ (what is the microbiological cause of his illness?). Moreover, you suspect your motives: using an antibiotic would be as much to cover your diagnostic uncertainty8 — a ‘just-in-case’ prescription that prevents subsequent accusation of undertreatment9 — and that its side effects could add vomiting and a rash to Ahmed’s already miserable condition.
WHAT ELSE COULD HELP (IN 2018)?
You would really like to know the underlying cause of Ahmed’s illness and if his condition is likely to deteriorate. Laboratory microbiological testing will not help — the laboratory turnaround will take too long.
You consider using a recently developed clinical rule to stratify his prognosis (risk of hospital admission for serious respiratory infection in the next 30 days),10 but Ahmed has two of the seven ‘STARWAVe’ characteristics (short [≤3 days] illness, temperature [parent-reported severe fever in the previous 24 hours or ≥37.8°C], age [<2 years], recession, wheeze on auscultation, asthma, and vomiting). This places him in the ‘normal’ (1.5%, 1:66) risk group, which does not reassure you or his parents.
Finally, you seek advice from your local children’s emergency department (CED). After listening to Ahmed’s history and examination findings, you hear the CED consultant audibly smile: she offers to see Ahmed, but she also says her waiting room has 20 children meeting Ahmed’s illness description, and, based on the hospital laboratory testing of other children with the same illness, she suspects Ahmed has an adenovirus infection, which is likely to self-resolve.
COULD LOCALLY RELEVANT, REAL-TIME SYNDROMIC/MICROBIOLOGICAL SURVEILLANCE HELP (IN THE FUTURE)?
Sitting at the top of the illness iceberg, the CED consultant has a ‘bird’s eye’ view of the epidemiology of currently prevalent illnesses in her area. But could this information be systematised and made available to primary care clinicians; and, if so, how would it work and is there any evidence it could be effective?
Our recent systematic review has identified several surveillance systems based in the US, Canada, New Zealand, Spain, and Norway.11 Using weekly or daily emails or faxes, they disseminate locally relevant information regarding circulating illnesses to primary care centres within geographically distinct areas. One such system is embedded within the electronic health record.
And we found promising evidence that this information could be effective in reducing antibiotic prescribing. The evidence is largely based on observational research, and therefore requires further experimental (RCT) evaluation (including an investigation of its cost-effectiveness), but let us consider how it works and how it could be operationalised in the UK.
BAYES’ THEOREM ‘PLUS’
Even if we do not know it as Bayes’ theorem, experienced primary care clinicians will be familiar with its application when making diagnoses. In response to open questions used early in the consultation, we consider a list of provisional diagnostic possibilities (in Ahmed’s case these might be: self-limiting viral infection, impending bacterial pneumonia, and Kawasaki disease). To each we assign a probability based on our past experience of the prevalence of that condition (self-limiting viral infection — probable; bacterial pneumonia — possible [and important not to miss]; Kawasaki disease — improbable (but also important not to miss). These provisional diagnoses are sometimes referred to as ‘prediagnostic probabilities’. We then seek evidence (using closed questions, examination findings, and investigation results) to increase or decrease the ‘post-diagnostic probability’ until we consider one sufficiently probable (or improbable) to rule in (or out) of the diagnosis.
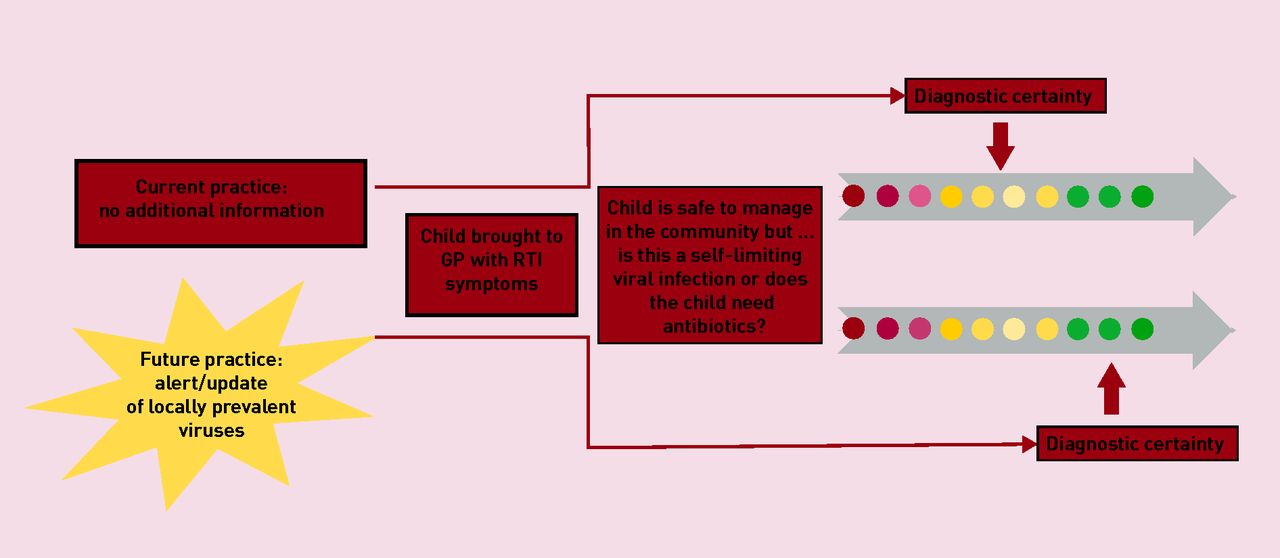
With locally relevant, real-time surveillance data, instead of basing the prediagnostic probability exclusively on our past experience of the prevalence of that condition, it can also be influenced by knowledge of its current prevalence — which is why we use the term Bayes’ theorem ‘plus’ (Figure 1).
{kind=link}
Role of infection surveillance data and effect on diagnostic certainty.
RTI = respiratory tract infection.
REAL-TIME INFECTION SURVEILLANCE IN UK PRACTICE
A substantial proportion of the necessary elements for a locally relevant infection surveillance system are already in place. For example, EMIS, Qsurveillance, Public Health England, and the RCGP Research and Surveillance Centre already capture and analyse regional syndromic (and some microbiological) data. The other two elements necessary are: 1) locally based microbial testing for a range of relevant microbes; and 2) the capacity to link and analyse the syndromic and microbiological data in real time. Once in place, primary care clinicians could receive alerts regarding the most prevalent infectious diseases (with microbial cause) in their locality.
CONCLUSIONS
We have described a system that could use existing syndromic data supplemented by locally relevant microbial data, to help improve the diagnosis and treatment of infectious diseases in primary care. Such a system should first be subject to rigorous evaluation to establish its intended (clinical and cost-effectiveness) and unintended (harmful) effects.
Notes
Provenance
Freely submitted; not externally peer reviewed.
Competing interests
The authors have declared no competing interests.
- © British Journal of General Practice 2018
In this issue









Jump to section
- Top
- Article
- THE CLINICAL PROBLEM (PAST, PRESENT, AND FUTURE)
- MANAGEMENT OPTIONS AND CURRENT GUIDELINES
- WHAT ELSE COULD HELP (IN 2018)?
- COULD LOCALLY RELEVANT, REAL-TIME SYNDROMIC/MICROBIOLOGICAL SURVEILLANCE HELP (IN THE FUTURE)?
- BAYES’ THEOREM ‘PLUS’
- REAL-TIME INFECTION SURVEILLANCE IN UK PRACTICE
- CONCLUSIONS
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

