


Abstract
Background Many guidelines have been developed in the area of depression but there has been no systematic assessment of their relevance to general practice.
Aim To assess national guidelines on general practice management of depression using two complementary approaches to identify specific ways in which guidance could be made more relevant and applicable to the nature of general practice and the patients who seek help in this context.
Design of study Review of national guidelines.
Setting Seven English speaking countries: UK, US, Australia, New Zealand, Ireland, Canada, and Singapore.
Method Seven guidelines were independently reviewed quantitatively using the Appraisal of Guidelines for Research and Evaluation (AGREE) scores and qualitatively using thematic coding.
Results The quantitative assessment highlights that most of the guidelines fail to meet the criteria on rigour of development, applicability, and editorial independence. The qualitative assessment shows that the majority of guidelines do not address associated risk factors sufficiently and the dilemma of diagnostic uncertainty flows over into management recommendations. Management strategies for depression (antidepressants and psychological strategies) are supported by all of the guidelines, with several listing drugs before psychological therapies; there is limited attention paid to the different types of psychological therapies. Moreover, the guidelines in the main fail to acknowledge individual patient circumstances, in particular the influence on response to treatment of social issues such as adverse life events or social support.
Conclusion Assessments of current national guidelines on depression management in general practice suggest significant limitations in their relevance to general practice.
INTRODUCTION
Depression is usually managed in general practice,1 and over the past decade, management guidelines have been produced by a number of nations to assist clinicians.2–8 However, there has been limited evaluation of such guidelines,9 apart from two studies that reviewed guidelines from the UK.10,11 They concluded that the regional guidelines were not of high quality and that they were based mostly on the 1992 Royal College of General Practitioners' consensus-based position statement.
General critiques discuss how depression guidelines ignore the particular issues around the conceptual basis of depression in general practice;12,13 how they fail to acknowledge patients' reluctance to take antidepressant medications14 and the varying evidence about their efficacy for primary care patients;15,16 and do not take account of the varied social issues associated with depression as it presents in general practice.9 Furthermore, GPs have stated that many guidelines are insufficiently flexible to be helpful with the variety of patients they see.17 There is evidence that many patients are frustrated by practitioners' use of guidelines for many conditions, as they want treatment and advice to be individually tailored.18
Current guidelines are mainly based on research evidence that has not been gathered in primary care populations, with the result that the strength of evidence underlying the main recommendations is often weak.9,14 Most of the treatments proposed by the guidelines have mainly been evaluated in patients meeting criteria for major depressive disorders, predominantly in secondary or tertiary care settings.15,19 There is insufficient evidence to support decisions about the use of antidepressants in general practice for patients who do not meet the criteria for major depressive disorders — a common situation in general practice.16 Additionally, trials usually exclude people with significant psychiatric and physical comorbidity, pregnancy, older people, and the young.
The purpose of this study is to assess national guidelines on general practice management of depression using two complementary approaches in order to identify specific ways in which guidance could be made more relevant and applicable to the nature of general practice and the patients who seek help in this context. This review forms part of a programme of research aimed at developing exemplary models of depression care for general practice. Selected current guidelines for the treatment of depression in general practice are reviewed using a standard well-validated generic guideline-assessment tool,20 which provides quantitative ratings as well as qualitative thematic analysis to enrich the numerical assessment and enable comparison of the content of the guidelines.21
METHOD
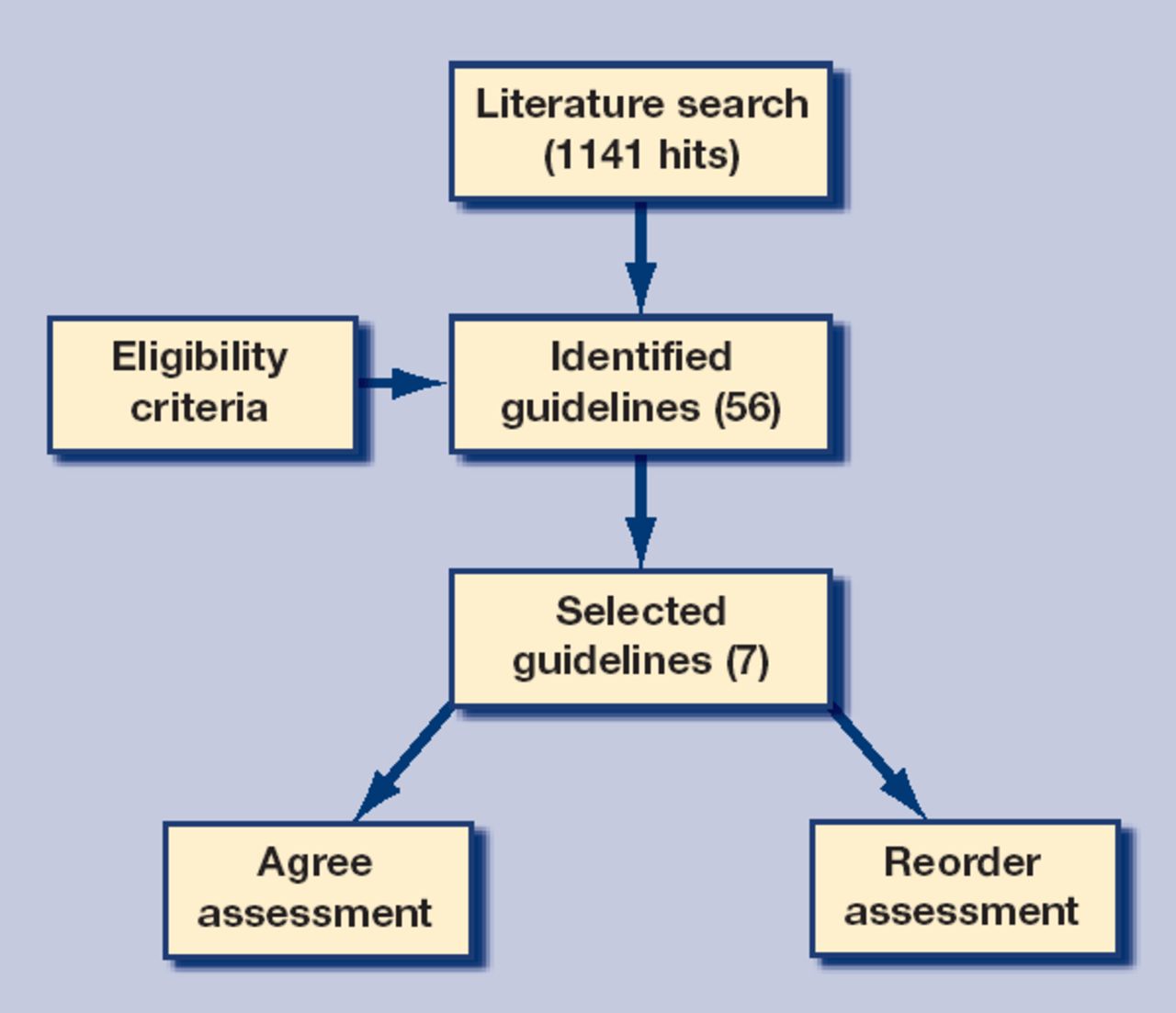
MEDLINE, Web of Science (ISI), EMBASE, CINAHL, PsychINFO, DARE, and Cochrane were searched for recent (1996–2006) national primary care guidelines using the terms ‘depression’ and ‘guidelines’ and ‘primary care/family practice’. Inclusion criteria were then applied to select the guidelines to be used in this review. Guidelines had to be national, in the English language, readily available to GPs, for adult patients, and the most recent for that particular developed country (Figure 1). This search was supplemented with a web search of guideline clearinghouses and relevant international primary healthcare/health provider organisations' guidelines and position statements. Each selected guideline was assessed independently using the two following approaches, to give a numerical quality rating18 and a thematic review.21,22

{kind=link}
Selection and appraisal of relevant guideline literature.
How this fits in
Current depression guidelines are mainly based on research evidence gathered in secondary care populations, which may not be applicable in primary care. The guidelines often do not take into account the social factors associated with depression in primary care, and fail to acknowledge patient reluctance to take antidepressants. GPs often find depression guidelines insufficiently flexible to help with the variety of patients they see. This study found that national guidelines for depression, despite being based on the same body of research evidence, vary considerably from each other in their recommendations on screening patients for depression, the use of self-help, and the length of antidepressant treatment. Some guidelines contain useful elements that others could benefit from adopting, or cross-referring to, including the assessment of suicide risk and guidance on switching antidepressants. Guidelines for depression in primary care should, in future, address the effectiveness of antidepressant treatment in helping patients with physical illness as well as social difficulties, including partner abuse.
Quantitative assessment
The selected guidelines were independently assessed using a well-validated generic clinical guideline tool: Appraisal of Guidelines for Research and Evaluation (AGREE).20 AGREE consists of 23 key items organised in six domains. These include:
scope and purpose: concerned with overall aim, specific clinical questions, and the target patient population (items 1–3);
stakeholder involvement: focuses on the extent of representation of the views of its intended users (items 4–7);
rigour of development: relates to process of synthesising evidence and methods (items 8–14);
clarity of presentation: deals with language and formatting (items 15–18);
applicability: pertains to the organisational, behavioural, and cost implications (items 19–21);
editorial independence: concerned with independence of the recommendations and conflict of interest (items 22–23).
For each domain, questions are scored on a 4-point scale from 4 (strongly agree) to 1 (strongly disagree) and then an overall percentage score is derived for each domain by summing all the scores of individual items and standardising the total as a percentage of the maximum possible score for that domain. This approach is similar to quality-assessment scoring systems used for assessing the quality of research papers in systematic reviews.
Qualitative thematic analysis
This approach to the guideline assessment was developed as part of a project, ‘Re-organising care for depression and related disorders in the Australian primary health care setting’ (Reorder project), and was undertaken without reference to the assessment using the AGREE guidelines. The Reorder research team consisting of GPs, mental health specialists, and non-clinical experts drawn from the behavioural and social sciences, set out to undertake a general practice-centred qualitative appraisal of the depression guidelines. The conceptual perspective of the team embraces a psychosocial rather than purely biomedical view of depression.
A data-extraction template/framework was devised and developed using an approach similar to that used for thematic analysis of qualitative research data.23 This involved an initial list of themes being identified during a 2-day workshop of the Reorder research team by the expert group. The framework and the meaning of each theme were reviewed and refined through further discussion after the workshop, and then applied to the guidelines independently. The framework was then further refined in light of the experience of this initial analysis, in an iterative process. The guidelines were then reviewed independently using this coding and assessment process. Subsequently, at a further meeting the coding and assessments by the two reviewers were compared, any differences were discussed with reference to the guidelines, and the coding and assessment finalised.
The coding process involved identifying where in the guideline a particular theme was discussed, then summarising the content into the data-extraction template. Assessment involved judging whether a theme was covered and, for some, such as ‘social risk factors outlined’, making a judgement about the completeness or detail to be included in the template.
Themes
The five domains of the Reorder thematic coding are guideline development, diagnosis of depression, management of an individual with depression, patient centredness, and system of health care (Box 1). The Reorder guideline review does not examine the strength and quality of the evidence drawn on by the different groups because this was assessed in detail using the AGREE criteria. Although guideline development is included in the AGREE criteria, the Reorder group also included it in the qualitative analysis, as one of the key concerns for the Reorder project is the inclusion of all relevant stakeholders in the design of depression care. In contrast to the AGREE generic guidelines, the other Reorder domains are specific to depression and reflect what is known about the nature of depression and the culture, context, and goals of general practice.
Box 1. Reordera consensus criteria.
▸ Guideline development — who was involved (in particular conflicts of interest), and whether consumers were involved.
▸ Diagnostic issues — screening, concept of depression used, tools recommended to assist in diagnosis, phase and severity of illness, associated social and demographic risk factors, physical and psychiatric comorbidity.
▸ Management — options for treatment and influence of severity, specific drugs, side-effects, length of treatment, suicide issues, and social support.
▸ Patient centredness — how the doctor–patient relationship, patient choice/engagement, and self-management are incorporated.
▸ System of health care — whether there are structured plans, enhanced communication, referral/linkages, follow-up; the cost and training of doctors.
Reorder = ‘Re-organising care for depression and related disorders in the Australian primary health care setting’.
Diagnosis criteria include considering the role of screening in general practice and how this should be done,24 and factors known to increase the risk of depression, including social risk, demographic risk, and comorbidity.19 It also includes phase of illness, as general practice sees patients presenting at very different stages of illness and accompanies them through depression and after recovery.25
Management of depression includes all aspects of the bio-psychosocial model of assessment and management of mental healthcare issues in general practice.26 This includes the varied treatments (drugs, psychological, social), the ordering of treatment,27 and matching treatment to the severity of depression.1 The domain of ‘patient centredness’ draws on evidence of the importance of the doctor–patient relationship in general practice care,28 the engagement of patients in management decisions, and the role of self-management.29 The importance of the context of care provision is recognised in the domain of ‘system of care’.15,30 This domain includes the resources needed to provide care, follow-up, and monitoring, such as training and funding. The study also looked for mention of aspects of the system of care that have been shown to improve outcomes specifically related to depression, for example, enhanced communication and structured plans.
RESULTS
Forty-nine guidelines identified by the search process were excluded because they were for specific population groups (for example adolescents, older people, students, or persons in the military), specific diseases (for example, bipolar illness or diabetes), or were regional rather than national. Seven guidelines met the inclusion criteria and are listed in Table 1.
Guidelines included in review.
Most guidelines had been published within the past 5 years, apart from the New Zealand guideline (which is due to be updated in 2009). Guideline length varied from seven pages (Australia) to 85 pages (US), resulting in considerable disparity in the amount of information presented. Assessment was made on the published guideline, as this is what most GPs would read, even though for some there was additional material (for example, more detail about the UK guideline was available on linked web pages). There was little cross-referencing between the guidelines selected.
Rankings using the AGREE assessment tool are shown in Table 2. The AGREE assessment shows that no guideline scored over 50% for all six domains. Overall, the UK guideline scored highest, followed by the US and Canadian guidelines. Most of the guidelines scored low on applicability. This domain contains items about organisational barriers, cost/resource implications for recommendations, and key review criteria for monitoring and/or audit purposes. Similarly, scores for editorial independence were low, indicating a lack of information on independence from the funding body and on conflicts of interest. Overall assessment by the two academic GP reviewers was that a mixture of sections from different guidelines (for example, the switching table for changing antidepressants from the Canadian guideline, combined with most of the sections of the UK guideline) would be most useful for GPs. To avoid lengthening all the guidelines, it would be helpful if they cross-referenced each other to indicate where readers could find more detail on particular issues.
The relative rankinga of the selected guidelines according to the six AGREE domains.
Assessment using the Reorder thematic analysis is shown in Table 3. Guideline development always includes experts, with most including GPs and few including patient input. Conflicts of interest are not well reported. Screening for depression is recommended mainly for those at high risk of depression (case finding), and only the US guideline recommends universal screening. The guidelines mostly utilise a psychiatric diagnostic classification system (Diagnostic and Statistical Manual for Mental Disorders [DSM-IV] or International Classification of Diseases [ICD-10]) whereas GPs often have a different concept of depression and frequently use severity (mild, moderate, severe) as their criteria for assessment.12 Use of depression instruments for initial assessment is recommended by all the guidelines except those from the UK. Associated risk factors and comorbid conditions are not covered in detail by the majority of guidelines. The New Zealand guidelines emphasise risk factors and cultural issues well.
Qualitative appraisal of the selected guidelines according to the five consensus Reorder domains.
With regard to management, three of the seven guidelines list drugs before psychological treatment,2,7,8 with three guidelines suggesting selective serotonin reuptake inhibitors as the first-line drug.3,5,8 There are varying lengths of treatment across the guidelines, from 6 to 12 months for a first episode of depression, and from 2 years to as long as necessary for recurrent depression. In most of the guidelines there is limited detail about use of specific psychological therapies, or suicide risk assessment, although three guidelines do provide a checklist,3,4,7 and the New Zealand guideline has a detailed risk-assessment guide. Social support in most of the guidelines is only briefly mentioned as a treatment. Self-management, for example books, self-help groups, is not mentioned at all by three guidelines.2,4,7 Only two guidelines emphasise the therapeutic relationship and patient centredness.2,6
Concerning system of care, the majority of guidelines mention multiprofessional care and a structured plan with enhanced communication about referrals. Follow-up is emphasised by all guidelines; however, ongoing monitoring is only mentioned by the Singapore guidance. As with the AGREE assessment, cost implications are not included in the majority of the guidelines.
DISCUSSION
Summary of main findings
These quantitative and qualitative assessments of current English-language national guidelines for depression management in general practice suggest scope for significant improvement to ensure that guidelines are relevant to everyday general practice. Significant limitations have been identified in the relevance and applicability of current guidelines to general practice. The quantitative assessment using the AGREE instrument found that most of the guidelines reviewed failed to meet the criteria on rigour of development, editorial independence, and applicability to organisational issues. The last may be partly because the generic AGREE instrument examines quality management at a practice level rather than at the level of the individual doctor's management of a patient with depression, at which most of the guidelines are aimed.
The qualitative assessment shows that the majority of guidelines do not address associated risk factors sufficiently for individual patients. The diagnostic uncertainty that GPs face with many patients presenting with symptoms of depression, including uncertainty about the use of psychiatric diagnoses or symptom severity, is evident in the management recommendations of the guidelines. Management strategies (antidepressants and psychological strategies) are supported by all of the guidelines, with several listing drugs before psychological therapies, and there is limited attention paid to the different types of psychological therapies available. Moreover, in the main, the guidelines fail to acknowledge individual patient circumstances, in particular the influence on response to treatment of social issues such as adverse life events or social support, or patient views about preferred treatments. For example, very few guidelines acknowledge that a common underlying issue for women is intimate partner abuse.31 Those guidelines (UK, Australia, Canada, US, and New Zealand) that do highlight social issues and self-help strategies (for example, education, bibliotherapy) in the initial treatment do so despite the fact that there are limited data from primary care settings on which to base recommendations.29
Strengths and limitations of the study
Limitations of this review include the inclusion of only English-language national guidelines and the wide variation in length of the guidelines materials that were assessed. The review did not include other related policy developments; for example, policy in the UK now includes the use of a depression instrument for initial assessment of depression.32 Despite these limitations, the study clearly shows that none of the guidelines addresses in detail questions that face GPs in their day-to-day work, such as how to optimise depression treatment in light of background social issues, which type of psychological treatment is beneficial for mild to moderate depression, and how to identify those patients most at risk of suicide.
Implications for clinical practice and future research
The wide variation in the severity and features of conditions like depression in general practice means that short guidelines will always remain limited in their relevance and applicability, while longer ones will often not be read by busy clinicians. A balance needs to be struck to optimise the usefulness of current guidelines. In future, guideline development needs to pay attention to the following:
how individuals of different ages, sexes, and cultural backgrounds experience social issues and comorbidities that affect depression and its treatment;
ensuring that identification of depression discusses the influence of phase and severity; and
that monitoring and self-help (including new technologies) are addressed.
The ideal depression guideline for GPs would also consider:
the culture of general practices and their ability to change and adapt;33
the recognition of depression that is not presented to general practice; and
the effects of changes in society (for example, increasing numbers of asylum seekers/refugees) that require greater cultural awareness in practitioners.
This study has clearly shown the limited relevance and applicability of these guidelines for practising doctors in primary care and the need for more evidence from the primary care setting if we are to inform future guidelines or decision support systems.
Acknowledgments
We would like to acknowledge the input of other Reorder members to the workshop — Helen Hermann, Chris Dowrick, Gail Gilchrist, Caroline Johnson, Maria Potiriadis, and Renata Kokanovich.
Notes
Funding body
The Reorder project is funded by the Australian Primary Health Care Institute and this work is independent of the funders
Ethical approval
Ethical approval was not needed
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received July 2, 2008.
- Revision received September 16, 2008.
- Accepted October 30, 2008.
- © British Journal of General Practice, 2009.
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

