


Abstract
Background Cardiovascular disease (CVD) is the leading cause of global mortality. Risk factor management in clinical practice often relies on relative risk modification rather than the more appropriate absolute risk assessment.
Aim To determine whether patients receiving more-frequently designated GP visits had increased benefit in terms of their absolute CVD risk assessment, as compared with patients in receipt of their usual GP care.
Design and setting Prospective, open, pragmatic block randomised study in a 1:1 group allocation ratio in three Western Australian general practices.
Method A convenience sample (n = 1200) of patients aged 40–80 years were randomised to 3-monthly GP visits (five in total for the intensive) or usual GP care (two in total for the opportunistic), with 12 months’ follow-up. The main outcome was absolute CVD risk scores based on the New Zealand Cardiovascular Risk Calculator. Others outcome measures were weight, height, waist circumference, blood pressure, and fasting blood lipids and glucose.
Results There were 600 patients per group at baseline. At 12 months’ analysis there were 543 in the intensive group and 569 in the opportunistic group. Mean (standard deviation [SD]) absolute CVD risk reduced significantly between baseline and 12 months in the intensive group (6.28% [5.11] to 6.10% [4.94]) but not in the opportunistic group (6.27% [5.10] to 6.24% [5.38]). There was a significant reduction between baseline and 12 months in mean (SD) total cholesterol (5.28 mmol/l [0.94] to 5.08 mmol/l [0.96]); low-density lipoprotein cholesterol (3.08 mmol/l [0.87] to 2.95 mmol/l [0.89]); triglyceride (1.45 mmol/l [0.86] to 1.36 mmol/l [0.84]); and in mean (SD) waist circumference in men (98.74 cm [10.70] to 97.13 cm [10.20]) and females (90.64 cm [14.62] to 88.96 cm [14.00]) in the intensive group.
Conclusion A targeted approach using absolute risk calculators can be used in primary care to modify global CVD risk assessment.
- cardiovascular diseases
- general practice
- general practitioners
- primary care
- primary prevention
- risk factors
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of global mortality affecting almost all countries and all income groups.1 Hypercholesterolaemia, lack of exercise, hypertension,2 obesity,3 and smoking4 are key risk factors in the treatment or prevention of CVD, and modification can be of potential benefit to healthy ageing.5,6
There are few primary care data on approaches to the primary prevention of CVD. Many CVD risk factors, though modifiable, remain undiagnosed and untreated. The presence of multiple risk factors and comorbidities among the general practice population calls for a more systematic and pragmatic approach from GPs.7 Relying on opportunistic presentations is unlikely to be successful. Even when diagnosed and with a treatment plan is in place, patient understanding of and adherence to treatment guidelines may not be rigorously followed.8 Lifestyle modifications, including reduced dietary intake and increased physical activity, are essential components for a sustained management plan.
Attempts to modify cardiovascular risk have, until recently, concentrated predominantly on reducing the relative risk from individual factors, such as hypertension, hypercholesterolaemia, and smoking, rather than the combined effects from a wider range of risk factors. A 1996 study looking at the ability of clinicians to quantify cardiovascular risk and treatment benefits accurately revealed that general internists and family physicians performed poorly,9 with each group revealing exaggerated perceptions of both disease risk and treatment benefit. Other studies also found clinicians often neglect to assess cardiovascular risk accurately in their patients.10,11
Evidence suggests that more accurate estimation of absolute cardiovascular risk can be achieved through use of sophisticated risk calculators.12 These instruments, based on Framingham Heart Study data, have been developed using intricate equations based on multivariate risk predictions to determine global cardiovascular risk in patients with no prior history of a cardiovascular event. They have been found suitable for use in everyday clinical practice,12 as well as facilitating improved clinical management.13,14
Uptake of risk calculators into routine clinical practice has been slow,15 and they remain under-used in primary care.11,16–20 Further general practice-based evidence is needed to convince patients and doctors that greater benefits can be achieved by shifting to calculations of absolute risk, rather than achieving traditional target guidelines for individual relative risk factors. The New Zealand (NZ) Cardiovascular Risk Calculator estimates probabilities for a CVD-related event over the next 5 years and helps GPs, primary healthcare professionals, and patients establish a reliable benchmark with which to assess a baseline, monitor progress, and encourage cooperation in CVD treatment plans.18
Howthis fits in
Calculations of absolute risk of cardiovascular disease (CVD) are being suboptimally used in clinical practice. Reliance is placed on estimations of single risk factors rather than the more important synergistic and cumulative effects from a number of CVD risk factors. Absolute risk calculators can be used to identify patients at greatest risk and reduce modifiable CVD risk factors and global absolute risk through primary prevention strategies at the primary care level.
The Fremantle Primary Prevention Study aimed to determine if more-frequently designated GP visits had increased benefit for patients in terms of their assessment of absolute cardiovascular risk, as compared with patients in receipt of their usual GP care.
METHOD
Study design
An open, prospective, pragmatic randomised study in three general practices in Western Australia was undertaken between November 2006 and July 2008.
Participants
A total of 1200 participants were consecutively recruited during routine surgery attendances, from patients attending three general practices (400 per practice). Inclusion criteria were patients aged 40–80 years. Exclusion criteria were patients with a prior history of CVD (angina, myocardial infarction, coronary artery bypass graft/stent, or stroke), patients who were physically unable to attend the practice during the study period, transient visitors to the practice, and those incapable of giving informed consent.
Interventions
Participants were randomly allocated to either opportunistic or intensive groups. Opportunistic patients had two study visits: an initial visit and one at 12 months. Intensive patients had five study visits: an initial visit followed by visits at 3, 6, and 9 months, with a final visit at 12 months.
Patient counselling/advice
All participants were advised individually of their risk-factor measurements and their specific targets, at each visit as listed under outcome measures below. Counselling and individualised treatment were offered as appropriate. Referrals to specialist and/or allied health services were initiated with participant agreement. Each participant was encouraged to aim for individual risk-factor targets, as well as improving their absolute risk score. The level of risk advice was at the discretion of the GP.
Outcome measures
Information was obtained on demographic data, medical history, the presence or absence of diabetic/cardiac medications, smoking, physical activity, weight, height, waist circumference, blood pressure recordings, and fasting blood samples for lipids and glucose. Patients with diabetes were blood tested for renal function, glycosylated haemoglobin, and urinary albumin/creatinine ratio. Risk-factor targets for blood lipid levels and blood pressure were based on National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand target guidelines,21,22 and were: zero smoking, blood pressure ≤130/85 mmHg, physical activity of 150 minutes/week, body mass index (BMI) <25 kg/m2, waist circumference <94 cm (males) and <80 cm (females), fasting blood glucose <5.5 mmol/l, and fasting lipid targets: <4.0 mmol/l total cholesterol, <2.5 mmo/l low-density lipoprotein cholesterol (LDL-C), >1.0 mmol/l high density lipoprotein cholesterol (HDL-C), and <2.0 mmol/l triglycerides. Blood pressure (measured electronically [Omron Corporation SEM-2 Automatic Blood Pressure Monitor, Omron Corporation] or by mercury/aneroid sphygmomanometry), weight (measured electronically), and waist circumference (midway between the superior iliac crest and inferior costal margin) measurements were standardised between practices. Blood testing was carried out by a clinical pathology laboratory (Western Diagnostic Pathology, Western Australia).
An overall absolute risk score for combined risk factors based on the NZ Cardiovascular Risk Calculator23 was obtained for each participant at each visit. The General Health Questionnaire (GHQ-28)24 relevant to the previous month was completed by each participant in both groups at the initial and final visits. Scoring was based on a Likert scale (0–3) and provided total scores from 0 to 84 (none to severe psychiatric distress related to illness). Cardiovascular risk and GHQ-28 scores were calculated by a researcher who was independent of the GP clinics.
Patients were included in the study only after consenting to participate, and their demographic data were collected. Three-monthly reminders were given to patients in the intensive group, and final-visit reminders were given to patients in the opportunistic group. No restrictions were placed on routine patient attendances outside of study visits, and the frequency of these was recorded. Detailed follow-up of medications used in patient management and of physical activity were not included in analysis, as these data were not comprehensively collected.
Sample size
Sample size was determined by assuming a risk reduction in global score of clinical significance to be 16% in the intensive group,25 and approximated as 10% in the opportunistic group, based on an α of 5% and power of 85%.
Randomisation
Randomisation was in a 1:1 group allocation ratio in variable blocks of 2, 4, and 6. Predetermined randomised lists (one for each GP site) generated by computer, based on a variable (2, 4, 6) block design in a 1:1 group-allocation ratio. Randomisation was in sequence and not concealed for logistical reasons, and was undertaken by the practice nurse enrolling patients.
Data analysis
Data were collected on data-collection sheets by the GP or practice nurse and forwarded for processing centrally. Paper records were transcribed into a Microsoft Access database, with participants identified only by study ID number, and analysed using SPSS (version 18.0). The denominator population used in analysis at each data-collection point included only those who attended at the respective time point and for whom data had been collected. A χ2 analysis was used to compare sex distributions in participants allocated to the two study groups and to compare the proportions not completing the study in both groups. Paired t-tests were used to compare changes between baseline and 12 months within the two groups, while independent t-tests were used for comparisons of the differences between changes over the 12 months. General linear modelling (univariate analysis of variance; ANOVA) was used to adjust for confounding sex and baseline differences between groups. Information on GP visits outside those for study participation was collected for some participants and compared between groups using the Mann–Whitney U test.
RESULTS
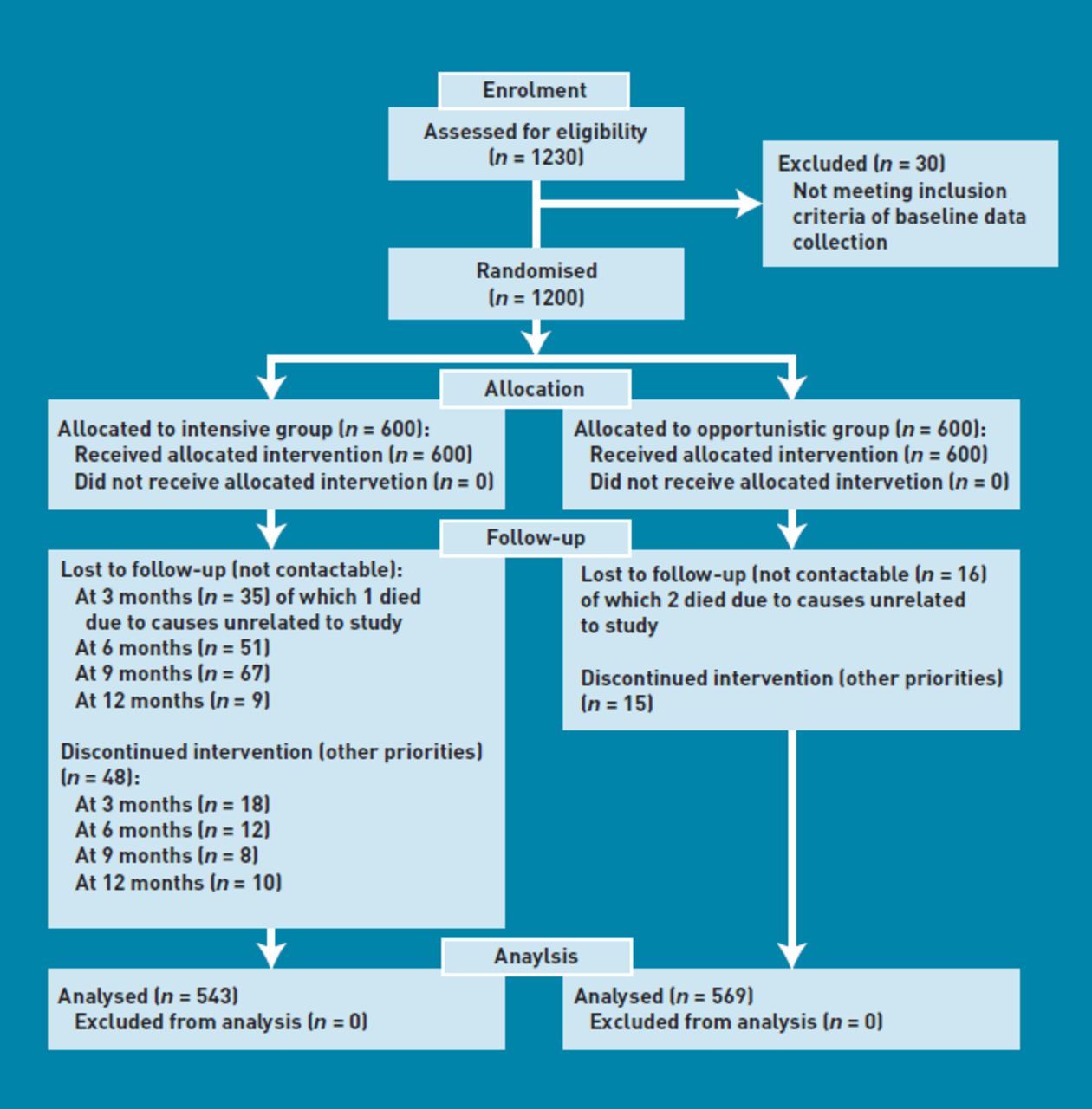
Figure 1 shows the CONSORT patient flow diagram for the study.26,27 Population demographics are shown in Table 1. There were more females in the study, though the sex distribution between the two study groups was not significant. Overall at baseline, 19% of 1200 participants had an absolute CVD risk score of over 10%.

{kind=link}
CONSORT diagram.
Demographics of the study population
At 12 months’ analysis, there were 543 participants in the intensive group and 569 participants in the opportunistic group, with a significantly greater proportion of participants not completing the study in the intensive group (χ2 = 8.29, degrees of freedom = 1, P = 0.004). There was no significant difference in participation rate at 12 months between the three general practice data-collection sites (96.3%, 92.3% and 89.5%).
Information on GP visits outside those for study participation was collected for a small number of participants (n = 89 intensive group and n = 92 opportunistic group). There was no significant difference between groups in the mean number of visits by these participants (5.58; standard deviation [SD] = 5.39) for intensive and 6.83; SD = 6.48 for opportunistic) outside of study visits.
Whether participants were on diabetic and/or cardiac medications was only reliably recorded at baseline. Information showed that 8.7% (52/600) of the intensive group were current smokers, and by 12 months this had decreased to 5.9% (32/543). In the opportunistic group, 10.2% (61/600) were current smokers, and by 12 months this had decreased to 7.9% (45/569). At baseline, 7.3% (44/600) of the intensive group and 8.7% (52/600) of the opportunistic group had diabetes. At 12 months, 9.0% (49/543) of the intensive group and 9.5% (54/569) of the opportunistic group had diabetes.
At baseline, 40.8% (245/600) of the intensive group were on cardiovascular medications, 0.67% (4/600) were on medications for diabetes, and 4.2% (25/600) on both. This was similar in the opportunistic group, where 41.0% (246/600) were on cardiovascular medications, 0.83% (5/600) were on medications for diabetes, and 3.83% (23/600) on both.
Mean values of risk parameters measured at each collection point over the duration of the study are shown in Table 2. Mean changes in the risk parameters between baseline and 12 months within each group and between the two groups are shown in Table 3. Paired results showed a small but significant reduction in absolute risk in the intensive group over the 12 months of the study. No significant risk reduction was observed in the opportunistic group. Total cholesterol, LDL-C, triglyceride levels, and waist circumference were reduced significantly between baseline and study completion in the intensive group only. The intensive group reported a reduction in GHQ-28 scores at 12 months compared to baseline. Both groups showed reductions in blood pressure (systolic and diastolic), BMI, and weight over the study duration.
Data measures for the two study groups
Mean changes in risk parameters between baseline and 12 months in each study group separately and between study groups
When comparing the differences between the two groups over the 12 months, total cholesterol, LDL-C, total:HDL-C ratio, and waist circumference showed significant reductions. Changes in LDL-C (ANOVA F = 6.70, P = 0.01), total:HDL-C ratio (ANOVA F = 4.69, P = 0.03), and waist circumference (ANOVA F = 12.75, P<0.001) between the two groups were significant after controlling for sex and baseline differences.
DISCUSSION
Summary
The study demonstrates that absolute cardiovascular risk can be improved by primary prevention strategies at the primary care level. The significant improvements in blood pressure and lipid levels achieved during the study may reflect the ability of combined medication and lifestyle factors to achieve target levels over the relatively short period of the study, but because data on medications were inconsistently collected at follow-up, it is not possible to draw firm conclusions. Some patients who were newly diagnosed with diabetes emerged during the course of the study, probably as a result of more frequent testing, especially in the intensive group.
Strengths and limitations
A systematic review12 of risk calculators based on Framingham Heart Study data found that the NZ Cardiovascular Risk Calculator performed well in terms of accuracy and feasibility for use in clinical practice.12,14 Despite the potential of these instruments to help clinicians improve the management of CVD, there remains a lack of evidence that such knowledge actually translates into better clinical outcomes.28 Instrument limitations include the fact that Framingham Heart Study data are based on US populations and may not be applicable elsewhere, especially among ethnic-minority groups. Information about adverse effects of risk-lowering interventions is lacking, while more novel risk factors are not included in calculations: lipoprotein(a), C-reactive protein, homocysteine.12
The current study used more-frequent (3-monthly interval, five in total) consultations delivered by GPs as the major intervention and compared these with usual care (two in total) over a 12-month period. For ethical reasons, no restrictions were placed on participant attendances outside designated study visits for either group. Findings showed that increasing the number of individual GP visits had an effect on absolute risk reduction and on a number of individual risk parameters as compared with patients having regular GP contacts. However, the study design and analysis did not take into account the effect of the natural clustering as a result of differences in the delivery of the intervention between GPs or practices.29 Blood pressure, BMI, and weight showed significant improvements in both groups over the 12-month study period.
Although both groups showed significant differences in a number of parameters between baseline and 12 months, only reductions in LDL-C, total:HDL-C ratio, total cholesterol, and waist circumference were significant over the study period between the two groups. It is possible that a longer study duration could have produced greater benefits from targeted lifestyle changes. In addition, randomisation at the patient level could have contributed to contamination between the groups. Had randomisation occurred at the GP or practice level (allowing for the imposed clustering),29 differences in outcomes may have been more significant between study groups.
Comparison with existing literature
It has been suggested that the next generation of clinicians should ‘treat risk not risk factors’.18 Clinical guidelines have shifted from estimating cardiovascular risk based on individual risk factors or simple summation of such factors, focusing instead on global risk using sophisticated instruments such as the NZ Cardiovascular Risk Calculator.10,17,18 For this process to gain more widespread acceptance, clinicians and patients will need to accept that calculation of global risk is not feasible without such accurate and easy-to-use instruments.12 This will involve a significant shift in accepting that estimating the likelihood of a cardiovascular event over a certain period of time (absolute risk) depends more on the interactive effects from a number of risk factors (age, sex, blood pressure, lipids, smoking, diabetes, obesity) rather than treating to target elevated levels in a few factors.
GPs are well positioned to offer positive health messages and treatment options to influence their patients’ health.30–32 Such benefits can be achieved through increasing patient involvement in self-care for risk-factor management, as well as providing greater primary care support through their GP, practice nurse, and primary care team.33 This is supported by the current study findings, as patients were well motivated to work cooperatively with their practice team, and 93% (n = 1112) of the 1200 recruited were still involved at the study conclusion. Those patients who saw their GP/practice nurse more frequently reported increased overall wellbeing, as determined by the GHQ-28.
Implications for research and practice
Absolute CVD risk calculations are being suboptimally used. Many GPs and specialists erroneously rely on estimations of single risk factors rather than the more important synergistic and cumulative effects from a number of CVD risk factors.10,17,18 At baseline, one in five patients in the study without known CVD had a greater than 10% (medium to high)34 chance of developing a cardiovascular event over the subsequent 5 years. Greater use of absolute risk calculators can help the primary care team identify such patients who are at greater risk, and introduce strategies to modify risk factors.17 The findings of this study showed that targeted interventions can produce significant changes in absolute risk reduction.
There is merit in encouraging primary care teams to streamline their assessment of absolute CVD risk, with better use of treatment care plans for identified at-risk patients. Such an approach might help engender an improved culture of risk calculator usage in primary care, thereby fostering a more cooperative, ongoing approach to global risk management in the future. As discussed previously, the limitations of absolute risk calculators in predicting future cardiac events must be acknowledged. Simply waiting for a cardiovascular event to occur, however, will inevitably mean that many patients will proceed to develop significant CVD disease or die before any preventative treatment is instituted. The patient cohort of this study engaged favourably with the team approach adopted. GPs and primary care teams should implement similar strategies with ongoing commitment to primary prevention in their practices.
The study provides additional general practice-based evidence to help convince both patients and doctors that improved benefits can be achieved by shifting to absolute risk calculations to help reduce the burden of CVD in the future. Further general practice-based research examining the effects of risk calculators on clinical practice and outcomes is warranted.
Acknowledgments
The authors acknowledge the assistance of staff at the three practices and medical students involved with data collation. The following also contributed to the study: Ms Michelle Caneppelle (data collation), Dr Frank Sotzik (data collation), Dr Agung Riono (data analysis) and Dr Robert Moorhead (research advice).
Notes
Funding
Investigator Initiated Research (IIR) Grant (AUS-Non Drug CVS-06-001) Pfizer, Australia. Western Diagnostic Pathology, Western Australia. The Australian Commonwealth Government Primary Health Care Research Evaluation and Development (PHCRED) Strategy Phase II.
Ethics committee
Human Research Ethics Committee of the University of Notre Dame Australia. Trial registration: Australian New Zealand Clinical Trials Registry; ACTRN12609000235202.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
Tom Brett, William Walker, Frances Cadden are GPs and Julie Young, Wendy Manea-Walley and Noelene Mora practice nurses at the participating practices and were involved in screening patients, data collection and write-up of the study. Pfizer (Australia) or its representatives had no input into the research design, conduct, analysis and write-up of the study.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received April 12, 2011.
- Revision received July 19, 2011.
- Accepted September 9, 2011.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

