


Article Figures & Data
Figures
- Figure 1
PRISMA flow diagram showing selection of studies.
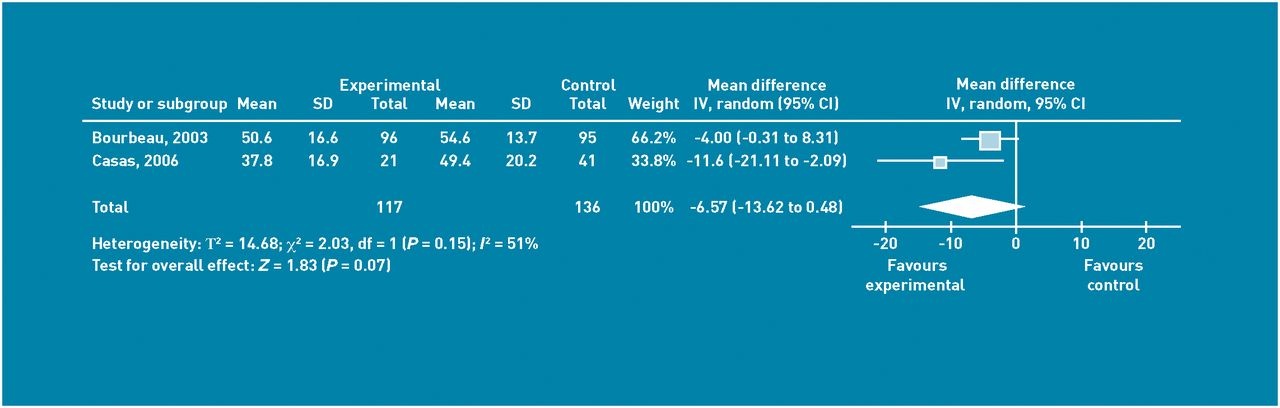
- Figure 2
Mean difference between groups at end of 12 months according to St George’s Respiratory Questionnaire for COPD-related quality of life. Random effects analysis.
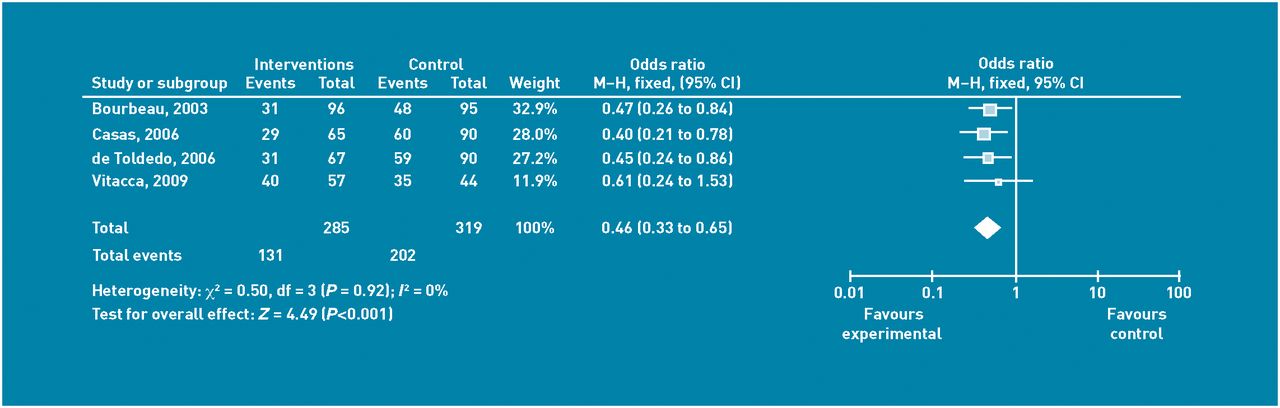
- Figure 3
Numbers of patients with one or more visits each to the emergency dept over 12 month period of study. Random effects analysis. M-H = Mantel Haenszel odds ratio.
- Figure 4
Number of patients with one or more hospitalisations over 12 months. Fixed effects analysis. M-H = Mantel Haenszel odds ratio.
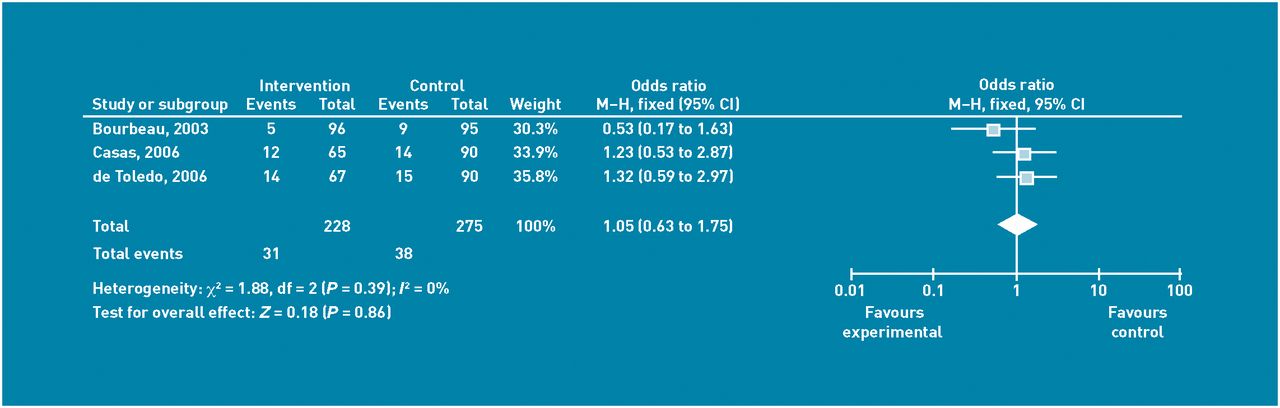
- Figure 5
Deaths over 12 months in the control group and telehealthcare group of the studies. Fixed effects analysis. M-H = Mantel Haenszel odds ratio.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
Study, year Number of participants, country, setting Intervention studied Main outcomes of interest Bourbeau 200312 191 participants, Quebec, Canada, participants were recruited by hospital clinic and were recruited if the had been hospitalised at least once in the preceding year for an acute exacerbation of COPD COPD self-management programme consisting of 1 hour/week teaching delivered to the patient at home for 7 weeks. Supervised by respiratory nurses. Followed by weekly telephone calls for 8 weeks. Then monthly telephone calls Medication profile, spirometry, 6-minute walk test, dyspnoea measurements after exercise, quality of life as measured by the SGRQ, healthcare use (emergency department visits, hospitalisations unscheduled and scheduled general practice, and specialist visits), costs and cost effectiveness Casas 200613 (Garcia-Aymerich 200722 155 participants, Barcelona, Spain, Leuven, Belgium, patients were recruited from two tertiary hospitals immediately following discharge. All patients had been admitted for COPD exacerbation for more than 48 hours Physical and social assessment and education were delivered with coordination by a case manager working between hospital and primary care. A web-based call centre facilitated coordination and weekly educational phone calls were made for the first month following discharge Hospital re-admission, quality of life as measured by SGRQ, clinical features of current exacerbation, comorbid conditions, treatment, including concordance and observed skills for inhaling drugs and oxygen, healthcare use, and mortality Chandler 199015 13 adult patients in Kentucky, US with COPD, asthma, or both who were receiving theophylline from pulmonary medicine outpatients The intervention group measured their theophylline level at home using a blood spot test, then phoned the clinic for advice on drug dosage Lung function at each clinic visit, degree of dyspnoea at each clinic visit, night and day coughing, wheezing and breathlessness were measured on visual analogue scales, drug-related adverse events. Patients' health attitudes and beliefs were assessed using the Krantz Health Opinion Survey and the Multidimensional Health Locus of Control de Toledo 200614 157 participants, in Spain all recruited during their tertiary hospital admission for an exacerbation of COPD Videoconferencing with patients in their own homes supported by a web-based patient record which also supplied education to patients and professionals. Patients had 24-hour access to the multidisciplinary team via a call centre Number of readmissions, number of visits to emergency department, mortality, acceptability to professionals, patterns of use, equipment, and communication costs Finkelstein 2004,23 200616 68 participants, in Minnesota, US an unspecified number of whom had COPD, congestive heart failure, or chronic wounds. The study took place between the central site and the home environment, where either the patient, or a carer, had to be physically and cognitively able to use the homecare equipment Two intervention groups: 1) standard care plus videoconferencing. 2) standard care plus videoconferencing plus physiological monitoring; for example, spirometry for COPD Termination from home care or loss of eligibility for home care, time to discharge to a higher level of care such as a nursing home or hospital, mortality, morbidity patient perception of telehealthcare (Telemedicine Perception Questionnaire), Patient satisfaction Home Care Client Satisfaction Instrument, quality and clinical usefulness of virtual visits, patient use of services, cost for both subjects and service providers Johnston 200017 Patients who had been referred for home health care because they suffered from a chronic condition in Sacramento, California, US via a health insurance organisation. 102 intervention patients, 110 control patients. 29 intervention patients had COPD, 19 control patients had COPD, the other patients had congestive heart failure, stroke, cancer, diabetes or needed wound care. All patients were projected to need two or more visits a week Both groups received routine home health care with face-to-face visits and access to telephone contact. However, the intervention group also had a remote videoconferencing system with equipment for testing cardiopulmonary status. This could provide a virtual visit at any time of day or night Use of services, costs for inpatient and outpatient services, visits to emergency departments, costs for pharmacy services, clinicians, emergency department visits, inpatient treatment, home healthcare costs and videoconferencing costs, patient compliance with medication regimen, patient knowledge about their illness, patient ability to move towards self care, patient satisfaction survey. Results for patients with COPD were not presented as separate from the other illnesses Nguyen 200818 50 patients with moderate to severe COPD (all of whom could use the internet) in San Francisco and Seattle US were assigned to either internet-based dyspnoea management (intervention) or face-to-face dyspnoea management control). Patients were recruited from web and non-web sources, including chest clinic referrals Internet based dyspnoea management focused on education, skills training and ongoing support and was delivered via a hand-held computer. The control intervention delivered the sam econtent using face-to-face methods Dyspnoea with activities of daily living and quality of life as measured with the Chronic Respiratory Questionnaire, exercise behaviour, and exercise performance, COPD exacerbations, self-efficacy and social support, and patient satisfaction Vitacca 200919 240 chronically ill respiratory patients, Lumezzane, Italy all of whom require home oxygen, some were on home mechanical ventilation, 101 had COPD, other reasons for respiratory failure included amyotrophic lateral sclerosis, restrictive chest disease, or other neuromuscular disease. Inclusion criteria: patient had had one hospitalisation for respiratory illness in the previous year. This study was conducted in the home setting The intervention was a teleassistance programme based on continuous 24-hour on-call service. Patients had pulse oximetry, and modem to transmit through the home telephone line. The teleassistance nurse was available by phone during working hours and out of hours the pulmonologist on duty was contacted Reduction in hospitalisations, reduction in urgent GP calls, acute emergency department admissions, also costs after paying for set-up of equipment Whitten 200720 Patients with a diagnosis of COPD and/or congestive heart failure who were prescribed home-healthcare services by their insurer were recruited Michigan, US. Intervention group = 83 patients and control group = 78 patients, The study was conducted in the home setting Intervention was a combination of traditional face-to-face home health care and virtual telemedicine visits The Short Form 36, Outcome and Assessment Information Set and patient charts were used to collect outcome data. Qualitative work, in the form of telephone interviews, collected patient perceptions of home telecare services Wong 200521 60 patients with COPD were recruited from an acute care hospital setting, in Hong Kong. The intervention was post-discharge telephone follow-up Intervention was post-discharge telephone follow-up provided by an experienced respiratory nurse. Two phone calls were made in the first 4 weeks after discharge from hospital Self-efficacy (a person with high self efficacy feels mor confident about engaging in activities and makes more effort to overcome challenges), as measured by the Chinese Self-Efficacy Scale, number of visits to emergency department, number of hospitalisations, and unscheduled visits by clinicians COPD = chronic obstructive pulmonary disease. SGRQ = St Georges Respiratory Questionnaire.
Study, year Adequate sequence generation Allocation concealment Blinding Incomplete outcome data addressed? All outcomes Free of selective reporting Free of other bias Bourbeau 200312 + + + + + – Casas 200613,29 (Garcia-Aymerich 200722 O O – + O – Chandler 199015 + O + – – – de Toledo 200614 O O – O + – Finkelstein 2004,23 200616 O O – – – – Johnston 200017 O O – O – – Nguyen 200818 + + – – + + Vitacca 200919 + – – – + – Whitten 200720 O O O – + – Wong 200521 + O + O + + + = criterion fulfilled. – = criterion not fulfilled. O = insufficient information.
Study, year Quality of life Emergency department visits Hospitalisations Deaths Drop outs Patient satisfaction Costs Other outcomes Bourbeau 200312 On the SGRQ, QoL life improved with mean difference, –4.00 (95% CI = –8.31 to 0.31) where negative change is improving There were fewer emergency department visits for the intervention group with an OR of 0.40 in comparison with the control group There were fewer hospitalisations for the intervention group with an OR of 0.47 in comparison with the control group There were 5 deaths out of % patients among the intervention group and 9 deaths out of 95 patients in the control group. OR 0.53 (95% CI = 0.17 to 1.63) 26 patients dropped out after randomisation, 1 was lost to follow up, and 11 found the burden of evaluation to be too great Total per–patient cost of self management was US$3778: mostly accounted for by the case manager's salary. Each case manager supervised 14 patients and there was no significant difference between costs for the two arms The differences from baseline lung function across the groups were not significantly different for either of the measures of FEV1 or FVC Casas 200613,29 On SRGQ, QoL improved with mean difference –11.60 (95% CI = –21.11 to –2.09) There were fewer hospitalisations for the intervention group with an OR of 0.40 in comparison with the control group There were 12 deaths out of 65 patients in the intervention group and 14 deaths out of 90 patients in the control group. OR 1.23 (0.46 to 1.75) After randomisation 35 patients were excluded from the trial = 35%: 26 deaths, 2 cases of cancer, 3 changed address, and 4 patients moved to palliative care Differences from baseline lung function increased more in the usual care group but not significantly (P = 0.6) Chandler 199015 No hospitalisations 2 patients due to moving and financial reasons No comparisons were statistically significant between the groups Home theophylline measuring kit (Acculevel) cost US$15, (1990) in comparison with routine measurement (>US$30) or physician visit (>US$25), other costs to be calculated include: clinician time, follow-up visits and long- distance telephone calls Symptomology was measured by visual analogue scale, there was no significant difference between groups. FEV1 decreased by a greater amount over the study in the control group (P>0.05) de Toledo 200614 Significant reduction in emergency department attendance OR 0.47 (95% CI = 0.24 to 0.89 Significant reduction in hospitalisations OR 0.50 (0.29 to 0.85) No significant difference in deaths. 14 patients died in the intervention group of 67 and 15 patients died in the control group of 90 Cost of the equipment: €36,469, cost of communications: €1656, 1 day hospitalisation for COPD costs €220. The reduction in hospitalisations will pay for the system by 1 year. 157 patients Finkelstein 2004,23 200616 No statistically significant difference in mortality across the groups Home care client satisfaction instrument scores were significantly higher for patients who had experienced virtual visits Breakdown of costs according to type of interaction. Virtual visits cost an average US$22.11, monitoring visits, US$33.11; and face-to-face visits, US$48.27 due to nurse and travel time Discharge to a higher level of care (nursing home or hospital): 42% of control participants, 21.4% of video care participants and 15% of telemonitoring participants Johnston 200017 Reported that mean number of visits per patient was 1.79 for intervention patients and control patients 1.53 Results are not given separately for different conditions Over 95% of both groups said that they agreed or strongly agreed with statements made pertaining to patient satisfaction. There was no difference between the groups Total mean cost of patients in the control group was US$2674 (standard deviation [SD] 6313) and in the intervention group US$1948 (SD 3681) note large SDs Nguyen 200818 Groups were compared using the Chronic Respiratory Questionnaire Only one patient attended the emergency department 50 patients were randomised, 39 remained after 6 months, 5 control patients dropped out, 7 intervention patients 4 of whom were unable to access the website Satisfaction scores for both arms were similar: 2.7 and 2.6. Vitacca 200919 Marked reduction in emergency department visit in intervention arm OR 0.07 (95% CI = 0.02 to 0.21) Reduction in hospitalisations, however CIs cross the line of no-effect OR 0.61 (95% CI = 0.24 to 1.53) No significant difference for deaths (COPD deaths are not reported separately) 111 patients were excluded because of reduced cognitive status, insufficient family cultural requisites or refusal ICU admission accounted for almost 50% of the total costs of hospitalisation in both groups. Mean overall cost per COPD intervention patient was more than 50% cheaper than for the control group COPD patients and tracheostomised patients requested the most assistance for ventilation. Fewer exacerbations were experienced by patients using teleassistance Whitten 200720 Interviews were conducted with 49 patients who were overall very satisfied with the telehealthcare programme. Data of patients with COPD and CHF were analysed together Wong 200521 There was a greater mean number of visits per patient in the control group: OR 0.17 There was no significant difference between the telephone and the control group in hospitalisation rates at 3 months P= 0.182 4 patients refused to answer the second wave of questions and had their answers replaced by the group mean CHF = chronic heart failure. COPD = chronic obstructive pulmonary disease. CRQ = Chronic Respiratory Questionnaire. FEV1 = forced expiratory volume in 1 second. FVC = forced vital capacity. ICU = intensive care unit. OR = odds ratio. QoL = quality of life. RR = relative risk. SGRQ = St George’s Respiratory Questionnaire. US$ = United States dollars. Є = Euros.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

