


Abstract
Background Prevalence of diagnostic inertia (DI), defined as a failure to diagnose disease, has not been analysed in patients with obesity.
Aim To quantify DI for cardiovascular risk factors (CVRF) in patients with obesity, and determine its association with the cardiovascular risk score.
Design and setting Cross-sectional study of people ≥40 years attending a preventive programme in primary healthcare centres in Spain in 2003–2004.
Method All patients with obesity attending during the first 6 months of the preventive programme were analysed. Participants had to be free of CVD (myocardial ischaemia or stroke) and aged 40–65 years; the criteria used to measure SCORE (Systematic COronary Risk Evaluation). Three subgroups of patients with obesity with no personal history of CVRF but with poor control of risk factors were established. Outcome variable was DI, defined as poor control of risk factors and no action taken by the physician. Secondary variables were diabetes, fasting blood glucose (FBG), body mass index (BMI), and SCORE. Adjusted odds ratios (OR) was determined using multivariate logistic regression models.
Results Of 8687 patients with obesity in the programme, 6230 fulfilled SCORE criteria. Prevalence of DI in the three subgroups was: hypertension, 1275/1816 (70.2%) patients affected (95% CI = 68.1 to 72.3%); diabetes, 335/359 (93.3%) patients affected (95% CI = 90.7 to 95.9%); dyslipidaemia subgroup, 1796/3341 (53.8%) patients affected (95% CI = 52.1 to 55.4%. Factors associated with DI for each subgroup were: for hypertension, absence of diabetes, higher BMI, and greater cardiovascular risk; for dyslipidaemia, diabetes, higher BMI, and greater cardiovascular risk (SCORE); and for diabetes, lower FBG levels, lower BMI, and greater cardiovascular risk.
Conclusion This study quantified DI in patients with obesity and determined that it was associated with a greater cardiovascular risk.
- diabetes mellitus
- dyslipidaemias
- hypertension
- inertia
- obesity
- physician’s practice patterns
- primary health care
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of mortality, according to the World Health Organization.1 The main modifiable risk factors are obesity, hypertension, diabetes, dyslipidaemia, and smoking.2 In addition, high blood pressure (HBP), high blood cholesterol (HBC), and high blood glucose levels are more prevalent in patients with obesity.3 For this reason, the detection and control of cardiovascular risk factors (CVRF) in patients with obesity is highly recommended.4
Clinical inertia, also known as therapeutic inertia, has been defined as a failure to start or intensify therapy when indicated by clinical guidelines.5 The factors associated with therapeutic inertia have been studied in an integrative review. These were by defined by Anjoulat et al as:
‘... providers’ knowledge of and attitudes toward evidence-based guidelines; providers’ own clinical judgment; providers’ awareness of patients’ attitudes, behaviours, and preferences; and providers’ ability to make decisions in specific clinical contexts.’6
In a recent review, Lebeau et al7 determined that Gil-Guillén et al distinguished diagnostic inertia from therapeutic inertia, as follows:
‘Diagnostic inertia was identified when a patient without known hypertension had high blood pressure but was labelled “normal” by the medical staff ...” 8
Furthermore, they found an inverse association between body mass index (BMI) and inertia in hypertensive patients.8 The concept of diagnostic inertia has also been studied in dyslipidaemia.9
In the Valencian Community in Spain, a free-of-charge health screening preventive programme was carried out between September 2003 and December 2004 from at primary healthcare centres. The Government invited all individuals aged ≥40 years to attend their health centre for a check-up that included cardiovascular and gynaecological screenings, and a vaccination campaign.10
Data from this preventive programme were used in the present study to determine the rates of diagnostic inertia for hypertension, diabetes, and dyslipidaemia in obese individuals, and the association between this inertia and the cardiovascular risk score was analysed.11 Other studies have analysed diagnostic inertia and its association with a personal history of CVRF.8,9 However, none have examined cardiovascular risk using a scoring system such as SCORE (Systematic COronary Risk Evaluation).11 SCORE is a system that calculates the probability of cardiovascular mortality in individuals aged 40–65 years that are free of CVD.
How this fits in
Diagnostic inertia is defined as non-adherence to clinical guidelines for diagnosing diseases. To the authors’ knowledge no previous studies have analysed diagnostic inertia solely in obese patients. In this study the issue of diagnostic inertia in obesity was assessed. The prevalence of inertia was very high for all cardiovascular risk factors. This association between inertia and cardiovascular risk was surprising because a higher cardiovascular risk was associated with this inertia. This issue should be avoided in clinical practice.
Although, Sepehri et al examined this association in patients with obesity, inertia was defined as a lack of advice to lose weight.10
This is an important distinction because cardiovascular risk scores consider the current status of patients rather than the personal history of CVRF.10
Therefore, by considering cardiovascular risk in the obese population, this study could determine whether there are gaps in detecting CVRF and, as a consequence, reduce the incidence of CVD.
METHOD
Study population
People living in the Valencian Community, aged ≥40 years, who attended their health centre for the preventive health screening programme were included in the study. These patients have a high prevalence of CVRF. The majority are female, of an older age, and attend their health centre frequently.12
Study design and participants
A cross-sectional study was performed in which all patients with obesity (BMI ≥30 kg/m2) who attended their health centre voluntarily during the first 6 months of the preventive programme were analysed. To qualify for the study patients had to be free of CVD (myocardial ischaemia or stroke) and aged 40–65 years. These are the criteria used to measure SCORE.11 Three subgroups of obese patients were established:
Those with no personal history of hypertension but with high blood pressure (HBP) (≥140/90 mmHg, or ≥130/80 mmHg for patients with diabetes).13
Those with no personal history of diabetes but with high fasting blood glucose (HFBG) values (≥7.0 mmol/L).14
Those with no personal history of dyslipidaemia but with HBC values (total cholesterol ≥5.17 mmol/L).15
The cut-off points for the diagnosis of these CVRF are equivalent to those defined in UK and European guidelines.16–19 The three groups were not independent; a patient could belong to one, two, or all three of the groups, or to none of them.
Use of the database was approved in 2007 and this study (determining the research question, literature and statistical analysis, and drafting of the article) was started in March 2014.
The physicians in the study were blinded to its aim of determining the prevalence of diagnostic inertia. They were only aware of the requirement to perform the preventive programme correctly.
Variables and measurements
In each subgroup the outcome variable was diagnostic inertia, defined as having high values of control parameters (HBP, HFBG, and HBC) but with no action taken by the physician. It would be expected that any action to be taken would occur once the patient had received blood test results, blood pressure measurement, a personal clinical interview, and had their BMI calculated. All tests and the physician’s action were recorded on the same morning.
The secondary variables were sex, personal history of CVRF (hypertension, diabetes, dyslipidaemia, and smoking), age (years), blood pressure (systolic/diastolic, mmHg), total cholesterol (mmol/L), fasting blood glucose (FBG) (mmol/L), BMI (kg/m2) and SCORE (%). SCORE was calculated using the variables sex, age, systolic blood pressure, total cholesterol, and smoking.11 Outcomes and secondary variables were measured using guidelines in force when the study was undertaken.13–15
Blood pressure was recorded as the mean of two measurements taken using a validated and calibrated device. BMI was calculated by measuring weight and height with calibrated devices, without shoes, and removing all objects that could affect weight. Blood was drawn at the start of the morning after an 8-hour fast and measured using calibrated devices to obtain readings for total cholesterol and fasting blood glucose.
Sample size
The sample group consisted of 1816 patients with unknown hypertension who had HBP, 3341 with unknown dyslipidaemia who had HBC, and 359 with unknown diabetes who had HFBG. The sample size calculation was therefore performed later.20 With a 95% confidence, an expected proportion of 50% (maximum), and with the aim of estimating the prevalence of inertia (the main study objective), errors of 2.3%, 1.7%, and 5.2%, respectively, were obtained.
Statistical analysis
Absolute and relative frequencies were used to describe the qualitative variables, and the mean and standard deviation for quantitative variables. In each subgroup, a logistic regression model was constructed to determine which variables were associated with diagnostic inertia. Using this model the adjusted odds ratios (ORs) were determined. These ORs were adjusted for SCORE, BMI, and a personal history of diabetes. In patients who had diabetes, FBG was used instead of a personal history of diabetes. The remaining variables were not introduced into the models due to collinearity issues. The predicted probability of inertia was calculated in the models and represented in graph form to aid understanding. The goodness of fit of the models was assessed by the likelihood ratio test. All the analyses were done with an α = 5% and the associated confidence interval (CI) was calculated for each relevant parameter. All the analyses were done with IBM SPSS Statistics 19.
RESULTS
An outline of the process is given in Figure 1. A total of 33 440 people attended their health centres to participate in the preventive programme. Of these, 8687 were obese and 6230 fulfilled the criteria to calculate the SCORE (aged 40–65 years and free of CVD). Of these, 2044 patients belonged to none of the groups, 2942 to just one group (hypertension 693, dyslipidaemia 2151, and diabetes 98), 1158 to two groups (hypertension and dyslipidaemia 983, hypertension and diabetes 54, dyslipidaemia and diabetes 121) and 86 to all three groups.

Flow chart of the study process. 2003–2004 data, Spain. CVD = cardiovascular disease.
The first subgroup (unknown hypertension with HBP) consisted of 1816 patients, of whom 1275 (70.2%) experienced inertia (95% CI = 68.1 to 72.3%). The subgroup of patients with unknown diabetes and HFBG consisted of 359 people, 335 (93.3%) of whom experienced inertia (95% CI = 90.7 to 95.9%). The subgroup with unknown dyslipidaemia and high HBC consisted of 3341 patients, of whom 1796 (53.8%) experienced inertia (95% CI = 52.1 to 55.4%).
The descriptive and analytical characteristics of the sample are shown in Table 1. The high prevalence of CVRF was reflected in the overall range values of hypertension (22.4–32.3%), diabetes (4.4–7.4%), dyslipidaemia (9.3–14.8%), and smoking (20.7–23.7%). Sex also varied (male 39.5–51.3%), the average age ranged from 53.1–53.7 years, the average BMI was 33.3–34.5 kg/m2, and the average SCORE was 1.6–2.1%. In the hypertension subgroup a greater probability of diagnostic inertia was associated with no personal history of diabetes (OR 0.18, 95% CI = 0.12 to 0.26, P<0.001), a higher BMI (per 1 kg/m2) (OR = 1.05, 95% CI = 1.02 to 1.09, P = 0.005) and a greater SCORE (per 1%) (OR 1.11, 95% CI = 1.05 to 1.18, P<0.001). In the dyslipidaemia subgroup the associated factors were a personal history of diabetes (OR 1.29, 95% CI = 0.91 to 1.82, P = 0.156), a higher BMI (per 1 kg/m2) (OR 1.01, 95% CI = 0.98 to 1.03, P = 0.628), and a greater SCORE (per 1%) (OR 1.25, 95% CI = 1.19 to 1.31, P<0.001). In the diabetes subgroup a greater probability of diagnostic inertia was associated with lower FBG figures levels (per 1 mmol/L) (OR 0.99, 95% CI = 0.99 to 1.00, P = 0.008), a higher BMI (per 1 kg/m2) (OR 0.99, 95% CI = 0.89 to 1.11, P = 0.901) and a greater SCORE (per 1%) (OR 1.16, 95% CI = 0.89 to 1.50, P = 0.266).
Analysis of inertia for recognising cardiovascular risk factors in obese patients at primary healthcare centres
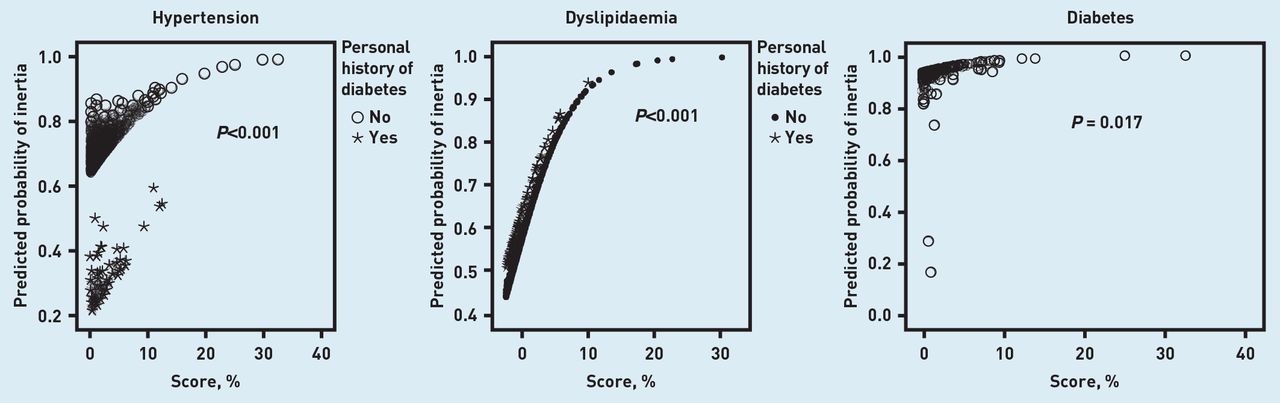
The relationship between SCORE risk and diagnostic inertia in each subgroup is shown in Figure 2. In these Cartesian graphs the predicted probability is plotted on the Y axis and the SCORE risk on the X axis. Symbols were used to distinguish whether a patient had a personal history of diabetes. The graphs demonstrate the increase in the probability of inertia in relation to the greater cardiovascular risk (SCORE). The variables in the graphs were a personal history of diabetes and SCORE. SCORE was included as a variable because it relates to the main CVRF (hypertension, diabetes, older age, male sex, smoking, and dyslipidaemia) and diabetes was included because it is not a predictive variable in SCORE.11

{kind=link}
{kind=link}
Predicted probabilities of diagnostic inertia and their relationship with the SCORE cardiovascular risk in hypertension, diabetes and dyslipidaemia. 2003–2004 data, Spain. P-values correspond to the goodness-of-fit of the multivariate models.
DISCUSSION
Summary
This study found that diagnostic inertia was prevalent; seven out of every 10 obese patients who fulfilled the criteria for HBP were not followed-up by their physicians in order to confirm or discard a diagnosis of hypertension, nine out of 10 patients with HFBG were not followed up for diabetes, and one-half of the patients who had HBC were not investigated for dyslipidaemia. It also shown that a greater cardiovascular risk was associated with a higher probability of inertia. This probability increased by between 11–25% (OR 1.11 to 1.25) for every 1% increase in cardiovascular risk (SCORE).
Strengths and limitations
The main strength of this study is that it is the first to deal with failure to detect CVRF in patients with obesity. The results show that physicians who should be diagnosing CVRF are failing to adhere to clinical guidelines; in other words, diagnostic inertia. The results also indicate that diagnostic inertia is associated with a greater cardiovascular risk. This is an issue that needs to be investigated further. The study design defined the limitations. There was selection bias, as only the patients who attended a preventive health screening programme were included. It would be interesting to replicate this study in general clinical practice. Information bias was minimised by the use of calibrated devices. The failure to include physician variables, such as age, sex, or training is a further limitation of the study.
Finally, although data were used from 2003–2004, diagnostic inertia remains a problem decades after it was detected in the 1980s.21 However, it was not defined as inertia at that time, and still remains a relevant subject of study.9 Clinical guidelines are constantly being updated and cut-off control parameters modified, but diagnostic inertia still exists.
Comparison with existing literature
Other studies have assessed the relationship between diagnostic inertia and CVRF in dyslipidaemia and hypertension. In relation to hypertension, a higher level of inertia was found in persons who smoked, had diabetes, coronary heart disease, or lower blood pressure, and had lower BMI. Studies that analysed inertia in dyslipidaemia have found that patients with a high cardiovascular risk were more likely to have abnormal high-density lipoprotein cholesterol levels but no diagnosis of dyslipidaemia.8,9 These results are generally in accordance with the current study, as a greater cardiovascular risk was associated with inertia. This could be due to the fact that most patients had multiple disorders and were polymedicated, so that the healthcare professional decided not to increase the therapeutic complexity of the patient. However, as these studies included patients both with and without obesity, it is difficult to compare findings.
Only one study analysed inertia in patients with obesity.10 Inertia was defined as a lack of advice to lose weight. This study and the current analysis determine the relationship between inertia and a cardiovascular risk score. The current study shows the same association as the previous one; that is, a greater risk score in patients with inertia.10
The findings were unexpected as these patients have a higher probability of cardiovascular death if no preventive measures are taken. Like Sepehri et al, the authors believe that physicians are focusing on the personal history of CVRF, rather than on the actual status of the patient. In other words, physicians do not consider blood pressure, FBG, or cholesterol levels, as they are concentrating more on the personal history of disease. Consequently, they do not calculate the cardiovascular risk score.10
Implications for research and practice
This study highlights a problem in situations where a patient has high control parameters but is not followed-up by the physician to confirm or discard a diagnosis of other CVRF, in addition to their cardiovascular risk due to obesity. The authors expected the prevalence of diagnostic inertia to be low, but in fact found that in all CVRF it was high (53.8–93.3%). Furthermore, patients with obesity, who already have a higher probability of cardiovascular mortality, had high rates of diagnostic inertia as the cardiovascular risk increased (OR 1.11 to 1.25).
Finally, this study was performed during a cardiovascular health screening preventive programme. Overall, considering that diagnostic inertia during this preventive programme was found to be frequent, it would be interesting to know what the situation is in daily clinical practice. In primary care settings physicians use their own judgement to decide whether to request tests or take action, as opposed to this preventive programme in which all patients were screened. A possible solution to prevent diagnostic inertia may be to integrate alarm systems into health records. For example, whenever a physician accesses the records of a patient with abnormal control parameters, this could be flagged up by a recognisable sound or a flashing light. Another approach would be to perform a qualitative (focus group) study to determine why family physicians do not follow clinical guidelines when diagnosing CVRF. This would also have relevance in the UK, because inertia is a prevalent problem that can affect patient outcomes.22
Acknowledgments
We thank the Conselleria de Sanitat (Valencian Community) for permission and finance for this study. The authors also thank Ian Johnstone for help with the English language version of the text.
Notes
Funding
This study received a grant from the Conselleria de Sanitat (Valencian Community). The grant was used to contract a person (Antonio Fernández) to collect and computerise the data. This public organism subsidised and authorised this study exclusively to determine the situation of patients attending their health centre. It played no part in the study design, data collection, analysis or interpretation, writing the manuscript or the decision to send it for publication.
Ethical approval
The data analysis was approved by an agreement between Miguel Hernández University and the Health Institution of the Valencian Community. These institutions guaranteed that all data analysis was in accordance with the current legislation on medical ethics. The institutions had no role in data collection, analysis, or interpretation. Nor did they have the right of approval over the finished manuscript.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received October 9, 2014.
- Revision requested December 15, 2015.
- Accepted February 13, 2015.
- © British Journal of General Practice 2015
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

