


Abstract
Background For older patients with polypharmacy, medication management is a process of careful deliberation that needs periodic adjustment based on treatment effects and changing conditions. Because of the heterogeneity of the patient group, and limited applicability of current guidelines, it is difficult for GPs to build up a routine.
Aim To gain insight into GPs’ medication management strategies for patients with polypharmacy, and to explore the GPs’ perspectives and needs on decision-making support to facilitate this medication management.
Design and setting Two focus group meetings with Dutch GPs, discussing four clinical vignettes of patients with multimorbidity and polypharmacy.
Method Questions about medication management of the vignettes were answered individually; the strategy chosen in each case was discussed in plenary. Analysis followed a Framework approach.
Results In total, 12 GPs described a similar strategy regarding the patients’ medication management: defining treatment goals; determining primary goals; and adjusting medications based on the treatment effect, GPs’ and patients’ preferences, and patient characteristics. There was variation in the execution of this strategy between the GPs. The GPs would like to discuss their choices with other professionals and they valued structured medication reviews with the patient, as well as quick and practical support tools that work on demand.
Conclusion To facilitate decision making, a more extensive and structured collaboration between healthcare professionals is desired, as well as support to execute structured medication reviews with eligible patients, and some on-demand tools for individual consultations.
INTRODUCTION
An ageing population means GPs increasingly manage older patients with multiple chronic conditions (that is, multimorbidity).1–3 These patients are often recommended to use multiple different medications at several times of the day. The chronic use of at least five medications is also called ‘polypharmacy’.4,5 In a recent study, it was found that the proportion of older patients with polypharmacy varied, by a factor of 2.4, between general practices after accounting for differences in the patient and practice population.6 This suggests that medication management, the process of monitoring and evaluating the patient’s prescribed medications, differs between GPs. Both multimorbidity and polypharmacy are associated with a range of adverse health outcomes, for instance, a lower quality of life, more adverse drug reactions, and higher rates of unplanned hospitalisation.5,7,8 Therefore, in older patients with polypharmacy, attention to appropriate medication prescribing is of major importance.
GPs in the Netherlands are searching for appropriate polypharmacy for older patients to help optimise prescriptions,9 while taking into account the best evidence along with patient perspectives; but this is often complex. It concerns a heterogeneous patient group and the combination in types and severity of diseases.10 Each patient also has their own characteristics (age, prognosis, cognitive ability, and preferences) to be taken into account.11,12 Due to changes in conditions of life and treatment effects, which are likely in this patient group, periodic adjustment of the prescribed medications is necessary. Unfortunately, due to the single-disease focus of most clinical practice guidelines (CPGs), it is not always possible to adopt the recommendations on medication prescribing in patients with multimorbidity.13–16 GPs have to find a balance between the risks and benefits of adhering to the CPGs and providing patient-centred care.12,15 In daily practice, GPs and patients often decide together which prescribing option to start with, and GPs often rely on their own experience when changing or stopping a medication prescription.17,18
Considering the limited applicability of CPGs and the heterogeneous patient group, little is known of how GPs assess the benefits and harms of the available treatment options. Furthermore, it remains unclear how GPs make decisions in medication management, and by what kind of factors this management is influenced. Therefore, this study aims to gain insight into the GPs’ medication management strategy for older patients with polypharmacy, and to explore the GPs’ perspectives, needs, and ideas on decision-making support to facilitate medication management for these patients.
How this fits in
Appropriate medication prescribing for older patients with polypharmacy is often challenging for GPs. By discussing clinical case vignettes of patients with multimorbidity and polypharmacy in two focus group sessions, 12 experienced GPs described their management strategy. Because patient characteristics and medication-related factors were appraised differently, as well as the GPs’ approach, variation occurred concerning the adjustments in the patients’ prescribed medications. Because the GPs also expressed the need for decision-making support, more extensive collaboration is desired between GPs and pharmacists to discuss patients with complex polypharmacy, as well as support to facilitate the execution of a medication review, or some on-demand tools for individual consultation.
METHOD
Design
Two focus groups with experienced GPs were organised. Local trainers were motivated to create more awareness among the trainees on polypharmacy and two meetings were organised within their training programme. All GPs participated voluntarily, being informed that anonymity and confidentiality were ensured; the discussion was audio-recorded. The meeting started with an individual written medication review of clinical case vignettes. A senior GP who lectured the GP-trainers moderated the meetings assisted by two researchers. The topic guide covered items on the medication management strategy, the accomplishment of the strategy, impact factors (sex, age, lifestyle, social context), and support tools.
Clinical case vignettes
Each focus group meeting started with an individual assignment for the GPs: reviewing medication management of four clinical case vignettes covered in a survey. The vignettes are described in Appendices 1–4, accompanied with possible treatment considerations, based on Dutch CPGs. The vignettes described patients (aged 68–84 years) diagnosed with multiple, highly prevalent chronic diseases, often part of a cluster of diseases.10 The patients used multiple medications, some of which can influence clinical functions, such as impaired renal function due to NSAIDs, or furosemide and hyponatraemia,19,20 or can induce symptoms (for example, dipyridamole and headache). The vignettes varied as regards to the safety of the combination of the medications, patient’s sex, age, lifestyle, and social context. The questions accompanying the vignettes covered treatment goals, an appraisal of the patient’s prescribed medications, and the possibility of consulting another health professional. The vignettes were developed by two of the authors and were validated by two additional practising GP-researchers.
Analysis
A Framework approach21 was used by defining themes a priori, in order to facilitate the plenary session and to focus on the research aims. The themes were integrated into the clinical vignette survey, and concerned ‘patient complexity’ and ‘treatment goals/strategy’, as these concepts were both considered as influencing GPs’ management.12,18,22 Concerning decision support, no a priori themes were defined. After the first meeting, the audio-tape was transcribed verbatim. The transcript was case and thematically coded by one researcher and quotes were classified into the two themes, if possible, or new themes were reported. If new themes emerged, they were discussed during the second meeting. The second meeting added no new themes and the course was comparable with the first meeting. The data indexed into the themes were checked by a second researcher and, in any case of disagreement, the two researchers were in discussion until consensus was reached.
RESULTS
Participants and group dynamics
A total of 12 GPs participated in two focus groups, each lasting around 75 minutes. All the GPs worked in the eastern or southern part of the Netherlands, and had, on average, 24.8 years of work experience (Table 1). The plenary sessions were dynamic. The GPs were enthusiastic, eager to hear about the considerations made by their peers, and the meeting was considered useful:
‘It turns out (again) that we should discuss these patients not on our own, but in a team, as it yields more [information] than you anticipate.’
(GP5)
Characteristics of the GPs participating in the focus groups (total N = 12)
GPs’ medication management strategy
All GPs described a quite similar medication management strategy. First, treatment goals were defined and prioritised, usually together with the patient. Second, the goals that were considered the primary concern in treatment were determined, and the focus of the current consultation was agreed. Mostly, primary goals were the reason for the encounter, or were regarded as important to prevent damage:
‘I think you should treat that first, this man’s complaints [case 4]. He is currently in a lot of pain.’
(GP2)
‘In my opinion [treating] the blood pressure is always the most important because the lower the blood pressure, the lower the chance for a CVA, TIA, or renal failure. That is my consideration.’
(GP5)
Third, adjustments were made in the patient’s prescribed medications, while considering formulated primary goal(s). Often, one or two adjustments were suggested immediately:
‘I don’t see, I don’t think the blood sugar level is too low [case 3], thus you could change a lot but I would start with [treating] the heart failure … If the HbA1c still decreases, then we could consider it [adjusting metformin].’
(GP11)
Accomplishment of the strategy
Although a similar strategy for polypharmacy was described, there was variation between GPs in the actual performance. There was variation in the (number of) treatment goals formulated for the patient, and the number of proposed primary goals; there was a focus on addressing several goals simultaneously versus a ‘step-by-step’ approach. Further, there was variation as regards focusing on optimising clinical values by referring to targets described in CPGs, or focusing on the reason for an encounter. As a result, the proposed adjustments in the cases’ prescribed medications varied (Figures 1–4). In Box 1 noteworthy findings per vignette are given, accompanied by statements made from GPs. The GPs expressed that work experience facilitates the decision-making process. Nevertheless, they seemed indecisive about the best approach; they repeatedly declared that they needed to search for information (for example, reference values, medication dosages, potential side effects), and were interested in the approach of other GPs. Besides, several prescribing options seemed possible according to the GPs. Yet, consulting a pharmacist or medical specialist was rarely considered, as they wanted to optimise the patient’s condition themselves first. Only if the patient’s condition did not improve, would they be likely to deliberate with a medical specialist.
Findings per case vignette, accompanied by statements given from the participating GPs
For case 1 (Appendix 1), it can be seen that all GPs focused on lowering blood pressure in this patient, which resulted in adding an ACE inhibitor. The variation in changes could be due to the fact that some GPs had more primary goals, whereas others had a more ‘step-by-step’ approach: ‘I have changed a series of prescribed medications. I am not sure if I will change everything at once, but this would be my purpose’ (GP8) and ‘[about the fact that this GP reported far less adjustments in the medication list] Yes, I did not want to adjust everything at the same time. I have recorded the medications which I would like to change at first place … After that you will see the patient again, and then you could focus on remaining goals … It is not very inspiring for the relationship of trust if you would say “Now we will do everything differently” after 8 years of treatment.’ (GP9)
With respect to case 2 (Appendix 2), nearly all GPs stated that naproxen should be stopped immediately, but not all GPs suggested alternatives to treating the patient’s pain. Moreover, only some GPs mentioned pain management as a treatment goal. Furthermore, all GPs suggested focusing on lowering blood pressure, but some GPs preferred to await the effect of stopping naproxen before increasing the dosage of enalapril.
GPs considered case 3 (Appendix 3) a typical ‘general practice patient’ because their approach would be to make one or two changes, wait a few days, and then determine the effect of the changes. For this patient, there was no apparent primary treatment goal: 10 different treatment goals were reported, and most GPs focused on three or four goals. This could be due to ambiguity about some symptoms or complaints. A GP stated, ‘That dizziness, we don’t know the type of dizziness. I am curious about the woman’s type of dizziness, I really want to know that. It hinders me.’ (GP1)
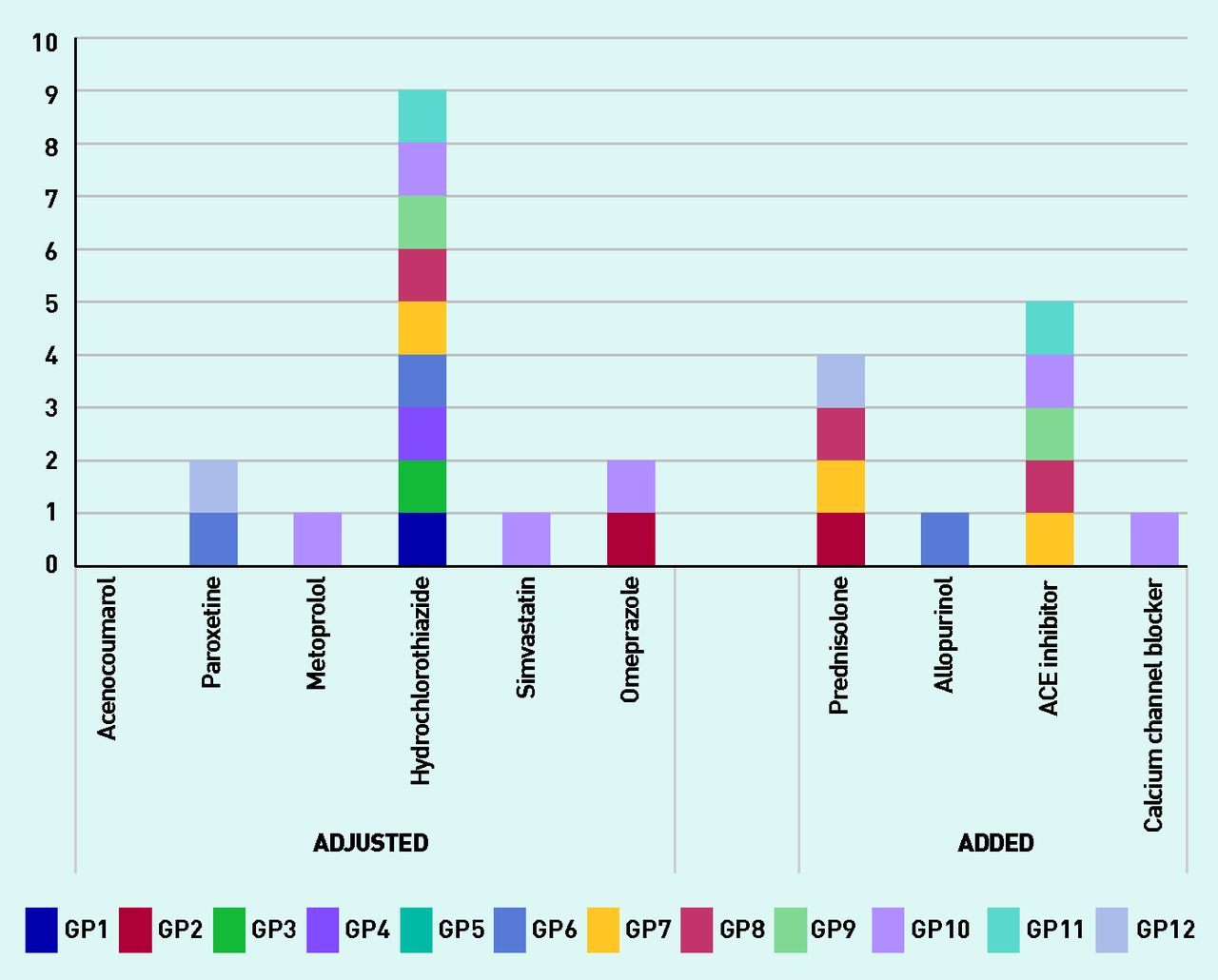
As regards case 4 (Appendix 4), nearly all GPs said that they would wish to stop hydrochlorothiazide because of the patient’s gout attack, despite the fact that this is no longer recommended in the Dutch guidelines. Treatment goals mainly focused on pain management and lowering the blood pressure.
Factors influencing the medication management process
The patient’s age, vitality, prognosis/ life expectancy, and quality of life were mentioned as factors influencing medication management. For instance, the patient’s age influenced the GP’s adherence to CPG recommendations. GPs accepted less optimal clinical values if the patient’s quality of life was at stake:
‘[If the patient was 85 years old] I would be more flexible about the blood pressure. That it will not result in, that he [case 2] falls or gets dizzy, or falls from a chair. I rather want him to be active with a higher blood pressure, than inactive with a lower pressure.’
(GP9)

Case 1 (Appendix 1): number of GPs that reported adjusting the particular prescribed medication in the case vignettes. ‘Adjust’ can indicate changing the dosage or stopping the prescribed medication.
Furthermore, the patient’s social context was considered important for the focus of the treatment, as well as their perspectives, wishes, and preferences on the proposed treatment.
‘ [About the information that the GP wishes to have] At least information about her lifestyle, for how long she uses the prescribed medications, what the motives are [to prescribe it], what her daily routine is. I just want to know more about her.’
(GP10)
‘I think that you could have an interesting talk with her [case 3] about what she aims for, and how frail she is.’
(GP7)
Regarding medication-related factors, the number of prescribed medications and their dosage, together with the combination of diseases, contributed to the complexity in management. When deliberating with the patient on potential medication adjustments, GPs sometimes hesitated to change or stop a prescribed medication. For instance, when medications were prescribed in their current dosage for a long period, or when it concerned medications prescribed by a medical specialist:
‘It is always a dilemma, a tense situation [adjusting medications]. We know that many hospital admissions are caused by medication … “errors” is a strong word, but surely due to failures in adequate medication. But we do know that stopping everything at once will also become counterproductive. Thus, that is really something to consider.’
(GP1)
Decision-making support tools
The GPs expressed that it was hard to think about appropriate support tools because of the heterogeneity of the patients. Tools regarded valuable by some GPs were characterised as practical and quick to use, such as the CHA2DS2-VASc score for stroke risk assessment,23 or the CVD risk assessment tool.24 Tools providing insight into the practices’ frail older population were also mentioned. Some existing tools incorporated in the GPs’ electronic medical record (EMR) system to check applicable CPGs lacked the GPs’ preferred ability to use it only when they needed it — to use it on demand. According to some GPs:
‘It would be nice if you can do that on demand. That there would be a button in your system which would automatically compare the medications and lab results, and then would report “the advice would be to …” But only when you press the button, and not that it goes “plop, plop” every time.’
(GP6)
Overall, two main options for support were valued. The first concerned meetings with GPs or pharmacists to discuss patients with complex problems, as a check of their expertise, and to exchange ideas and information around medication management decision making. About half of the GPs reported having meetings with a pharmacist at least bi-monthly, but only a few already discussed the older patients in multidisciplinary teams:
‘It is not such a bad idea to do [talking about complex patients], and to discuss them together, like we are doing right now. When doing so, you come up with new ideas sooner, like, I should pay more attention to those factors.’
(GP10)

Case 2 (Appendix 2): number of GPs that reported adjusting the particular prescribed medication in the case vignettes. ‘Adjust’ can indicate changing the dosage or stopping the prescribed medication.

Case 3 (Appendix 3): number of GPs that reported adjusting the particular prescribed medication in the case vignettes. ‘Adjust’ can indicate changing the dosage or stopping the prescribed medication.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 4 (Appendix 4): number of GPs that reported adjusting the particular prescribed medication in the case vignettes. Adjust’ can indicate changing the dosage or stopping the prescribed medication.
The second concerned medication reviews with the patient,25 executed during an annually extensive consultation. Some GPs stated that agreements with a pharmacist were made to perform a medication review, and a few participated in a programme focusing on managing the frail older patient, that included a medication review. Nevertheless, it seemed that the two options for support were not yet structurally performed. Perceived issues related to the execution of medication reviews were: lack of time, minimal beneficial results, and uncertainty about the patients who may be eligible for a review. Subsequently, GPs stated that the means to select these eligible patients systematically and easily were not sufficiently applicable.
DISCUSSION
Summary
Although the GPs had a similar medication management strategy, there was variation as regards the accomplishment of this strategy, due to differences in the GPs’ approaches (for example, focus on clinical values versus reason for encounter, or step-by-step versus simultaneous approach). Patient- and medication-related factors influenced the medication management process. As a result, variation existed in the proposed adjustments of the patients’ prescribed medications. Collaboration between GPs and pharmacists was valued as a medium to discuss patients with complex medication regimens, as well as structured medication reviews with the patient, and quick tools that work on demand.
Strengths and limitations
Clinical vignette surveys are shown to be effective for the evaluation of treatment decisions made by GPs.26–28 The applied study design can be seen as a major strength, because all GPs assessed identical hypothetical patients and thus provided insight into some level of variance regarding medication decision making. Further, using focus group meetings enabled GPs to contemplate the same patient, and to enquire about possible reasons for variation in their prescribing management. A limitation of this study is the inclusion of only experienced GPs, thus introducing possible bias. More specifically, GPs in other studies mentioned lacking certain skills, or felt incompetent managing patients with multimorbidity.11,29,30 Although this was not found in the present study, it was also not explicitly asked about. Also, only two meetings were organised. However, because the second meeting did not reveal any new themes, and the content of the discussion resembled the first meeting, the data-collecting process was considered saturated.
Comparison with existing literature
Contrary to the methods chosen in previous studies,11,12,17,18,22,29,30 this study incorporated the assessment of case vignettes based on fictitious patients into focus group sessions, which yielded information about variation in medication adjustments between GPs, as well as considerations for the choices made. This study therefore clearly showed that, for similar patients, GPs executed their medication management strategy quite differently. As far as the authors are aware, this has not been found in other studies. As to factors influencing decision making, these findings show similarities with existing literature. For instance, the findings that less stringent levels of disease control were accepted, that compromises were made between what a GP thought was best for a patient and the patient’s requests, and that setting priorities in management was of importance.17,18 In a study by Schuling and colleagues,11 it was stated that some GPs hesitated to discuss the subject of life expectancy. This is contrary to the findings in this study, as all GPs intended to enquire about a patient’s prognosis and quality of life. Luijks and colleagues12 showed that the patient’s quality of life was a main focus of GPs’ professional performance, and management was adapted to personal preferences and vitality. Adhering to available CPGs has been described as not very realistic or as even unwanted in polypharmacy.11,18,31 Although guideline adherence was not a main topic in these sessions, the GPs indicated that they did not always adhere to the CPGs, but they referred to CPGs as a fundamental basis for judgement.
Implications for practice
Even GPs with a lot of experience and skills perceive the need for additional support to facilitate decision making in polypharmacy. Considering the potential consequences of failure in medication management, it seems evident that decision-making support tools, such as BADRI,32 although not available in the Netherlands, are important. As evidence is available that a programmatic approach can be effective, and the availability of these support tools increases, it should be stressed that implementation strategies are needed to facilitate their usage in practice. In a systematic review on decision-making tools for multimorbidity,33 none of the available tools included a patient-centred approach, or worked on demand — components that were regarded as important by the GPs in the present study. Focusing on extensive collaboration between healthcare professionals seems therefore more promising as a means to facilitate medication management and to reduce possible inappropriate variation in medication prescribing. Although a few GPs indicated they participate in multidisciplinary team meetings, there seems to be room for improvement as regards embedding these meetings structurally. Because structured meetings with GPs and pharmacists around pharmacotherapy already exist (as in pharmacotherapy audit meetings),34,35 these seem suitable to embed discussions around patients with complex polypharmacy. Medication reviews with patients can also facilitate medication management, but currently seem not to be structurally performed. More knowledge is needed on the role patients can play in these reviews, especially regarding their health literacy.36 Interventions exist that include executing a medication review, but these are not embedded nationwide. Also, acceptable software that could extract eligible patients seemed insufficiently applicable to GPs. Recently, Sinnott and colleagues37 described a future intervention to improve medication management by combining the concept of discussing complex patients with multiple GPs, and discussing the determined results during a medication review with the patient. It seems a promising intervention; however, it does not account for the uncertainty around the potential patient group eligible for such a review pointed out by the GPs in the current study. Therefore, it is worthwhile enquiring about the group eligible for such a review, perhaps supported by a tool incorporated into the GP’s EMR system that could select these eligible patients.
In conclusion, a more extensive and structured collaboration between healthcare professionals is desired to facilitate decision making in this heterogeneous patient group, as well as support to simplify the process of selecting patients eligible for a structured medication review, and some on-demand tools for individual consultation.
Acknowledgments
The authors thank all participating GPs for their effort and input during the focus group sessions. Furthermore, we would like to thank Dr Alfons OldeLoohuis for his contribution to the organisation and execution of the focus group sessions, and also thank the GP-researchers for their help in validating the clinical case vignettes.
Appendix 1. Adams: description of fictionalised case vignette with possible treatment considerations
Vignette 1: Mrs Adams (71 years old)
Mrs Adams visits her GP after completing her high-dosage prednisolone treatment. For 10 years, Mrs Adams has been diagnosed with moderate COPD. The GP is her main clinician, because she is considered a patient with stable COPD. In the last 14 months, Mrs Adams experienced three acute exacerbations of COPD, for which short courses of systemic corticosteroids were prescribed (prednisolone 30 mg o.d. for 7 days). During the consultation, Mrs Adams tells the GP that she does not experience severe shortness of breath any more, but she does feel somewhat airless, and, until recently, she has had headaches quite often, she feels tired, and she has a frequent need to urinate. In 2007, Mrs Adams was diagnosed with diabetes mellitus type 2, and at the end of 2012 she suffered a TIA. Moreover, she has high blood pressure and impaired renal function. Mrs Adams and her husband still live together independently at home. For over 40 years, Mrs Adams had been a heavy smoker, but she gave up smoking in 2004, when diagnosed with COPD. Mrs Adams works in a library one afternoon in the week, and walks with her daughter twice a week.
| Prescribed medications | (Laboratory) test results | Visit (20 May 2014) | Visit (30 Jul 2014) | Current visit (1 Oct 2014) |
|---|---|---|---|---|
| Metformin 1000 mg t.i.d. | Blood pressure (mmHg) | 150/91 | 150/92 | 149/91 |
| Gliclazide 80 mg b.i.d. | eGFR (ml/min/1.73 m2) | 42 | 42 | 41 |
| Acetylsalicylic acid 80 mg o.d. | Albumin/creatinine ratio (mg/mmol) | 3.6 | 3.6 | 3.6 |
| Dipyridamole 200 mg b.i.d. | LDL cholesterol (mmol/l) | 3.0 | 3.0 | 2.8 |
| Simvastatin 40 mg o.d. | HbA1c (mmol/mol) | 52 | 57 | 61 |
| Hydrochlorothiazide 25 mg o.d. | Fasting blood glucose level (mmol/l) | 7.0 | 7.1 | 8.1 |
| Salbutamol 200 mcg q.i.d., p.r.n. | BMI (kg/m2) | 30 | 30 | 30 |
| Tiotropium 18 mcg o.d. | ||||
| Omeprazole 20 mg o.d. | ||||
| Alendronic acid 10 mg o.d. |
Points of concern: diabetes control, impaired renal function, blood pressure, dyspnoea
Possible treatment considerations based on separate Dutch CPGs:
Lower the metformin dosage. In patients with a renal function at 30–50 ml/min, the maximum metformin dose is 500 mg b.i.d.38
Consider starting with insulin. Insulin is considered since the HbA1c target (<58 mmol/mol) was not met, despite the maximum metformin dosage.39
Change the dosage of hydrochlorothiazide into 12.5 mg o.d. For hypertension treatment, an ACE inhibitor is preferred in patients with diabetes mellitus type 2 and microalbuminuria (loss of 3.5–35 mg albumin/mmol creatinine in women).24
Start with an ACE inhibitor. Despite the current hydrochlorothiazide dose, the recommended systolic blood pressure level of ≤140 mmHg was not achieved, therefore additional medication is recommended. An ACE inhibitor is preferred in patients with type 2 diabetes mellitus and microalbuminuria (loss of 3.5– 35 mg albumin/mmol creatinine in women).24 The recommendation is to stop the hydrochlorothiazide for 2–3 days, and then start with the ACE inhibitor and hydrochlorothiazide.
Change simvastatin into atorvastatin 20 mg o.d. If the LDL cholesterol target of <2.5 mmol/l is not met with simvastatin, the recommendation is to change to the preferred second step in cholesterol therapy.24
A common side effect of dipyridamole is headache. In patients with complaints related to dipyridamole, one can consider giving acetylsalicylic acid alone.24 Clopidogrel is an alternative to prevent myocardial infarction (MI) and stroke; if complaints occur related to the use of acetylsalicylic acid, change acetylsalicylic acid into clopidogrel.
Consider starting with inhaled corticosteroids. Inhaled corticosteroids are considered for patients with frequent exacerbations.40 If it is decided not to start with inhaled corticosteroids, stop with omeprazole; the patient finished the 7-day high-dose oral corticosteroids course, and consequently the use of a proton pump inhibitor is no longer indicated for this patient.41
Consider consulting a nephrologist. Recommended in patients >65 years with an eGFR between 30 and 45 ml/min/1.73 m2.38
Appendix 2. Brown: description of fictionalised case vignette with possible treatment considerations
Vignette 2: Mr Brown (68 years old)
Mr Brown was asked to visit his GP, as laboratory tests showed a decline in renal function. At the end of 2012, he suffered an MI and since then he uses several medicines as measures for secondary prevention after MI. In 2009, Mr Brown was diagnosed with osteoarthritis. An NSAID was prescribed for pain management because treatment with paracetamol had insufficient effect, and during treatment with tramadol he experienced nausea. Mr Brown lives alone, and quit smoking at the age of 60. He intended to cycle every day, but is not always able to do this because of pain, especially in the knees. Last August, a diuretic was prescribed because of his high blood pressure, and the GP evaluated Mr Brown’s sodium intake and lifestyle. In November, his blood pressure was hardly lowered, and therefore an ACE inhibitor was prescribed.
| Prescribed medications | (Laboratory) test results | Visit (21 Aug 2014) | Visit (12 Nov 2014) | Current visit (15 Dec 2014) |
|---|---|---|---|---|
| Naproxen 250 mg b.i.d. | Blood pressure (mmHg) | 165/100 | 160/100 | 158/96 |
| Acetylsalicylic acid 80 mg o.d. | eGFR (ml/min/1.73 m2) | 52 | 50 | 42 |
| Metoprolol 100 mg o.d. | Albumin/creatinine ratio (mg/mmol) | 2.3 | 2.4 | 2.8 |
| Simvastatin 40 mg o.d. | LDL cholesterol (mmol/l) | 3.0 | 3.1 | 3.1 |
| Hydrochlorothiazide 12.5 mg o.d. | Fasting blood glucose level (mmol/l) | 4.8 | 4.7 | 4.8 |
| Enalapril 5 mg o.d. | ||||
| Omeprazole 20 mg o.d. |
Points of concern: blood pressure, cholesterol, use of naproxen, pain
Possible management considerations based on separate Dutch CPGs:
Stop naproxen. Use of an NSAID, in combination with acetylsalicylic acid, is discouraged due to gastric complications, and because NSAIDs stimulate sodium and water retention, which increases the risk for (or worsens) impaired renal function, high blood pressure, and heart failure. It is further discouraged in patients with an MI.19,42
Start with paracetamol/acetaminophen (with codeine) as an alternative for naproxen, or consider morphine therapy, or corticosteroid injections in the knee. All as possible alternatives for pain treatment.18,40
Increase ACE inhibitor dosage. The recommended systolic blood pressure level of ≤140 mmHg is not achieved with the current dosage of hydrochlorothiazide and enalapril.24
Consider changing simvastatin into atorvastatin 20 mg o.d. If the LDL cholesterol target of <2.5 mmol/l is not met with simvastatin, the recommendation is to change to the preferred second step in cholesterol therapy.24
Assess possibilities for a knee brace, or knee arthroplasty. In view of the patient’s age and physical condition, surgery could be considered as an option.43
Appendix 3. Smith: description of fictionalised case vignette with possible treatment considerations
Vignette 3: Mrs Smith (84 years old)
Mrs Smith visits her GP with complaints about dizziness. During the consultation, she further indicates that she has sleeping problems due to shortness of breath and a frequent need to urinate. Mrs Smith was weighed and had gained 4 kg since her last visit. She has had hypertension since 1999, and osteoporosis since 2000. Concerning her osteoporosis treatment, she used alendronic acid for 5 years. In 2002, Mrs Smith was diagnosed with type 2 diabetes mellitus, and in 2008 she was diagnosed with cardiac dysrhythmia, for which she receives anticoagulation medication from an anticoagulation clinic. Since 2014, she has had heart failure with symptoms of fluid retention, and therefore furosemide is prescribed. She lives alone, and generally stays indoors. Mrs Smith’s daughter visits her twice a week with groceries, and to give practical household help.
| Prescribed medications | (Laboratory) test results | Visit (03 Oct 2014) | Current visit (6 Nov 2014) |
|---|---|---|---|
| Calcium/vitamin D 600/400 o.d. | Blood pressure (mmHg) | 148/92 | 149//92 |
| Paracetamol 500 mg t.i.d. | Ventricular rate (b.p.m.) | 89 | 92 |
| Metoprolol 100 mg o.d. | eGFR (ml/min/1.73 m2) | 46 | 42 |
| Lisinopril 5 mg o.d. | Albumin/creatinine ratio (mg/mmol) | 2.4 | 2.6 |
| Furosemide 40 mg o.d. | LDL cholesterol (mmol/l) | 2.5 | 2.5 |
| Simvastatin 40 mg o.d. | HbA1c (mmol/mol) | 58 | 58 |
| Metformin 500 mg b.i.d. | Fasting blood glucose level (mmol/l) | 4.8 | |
| Phenprocoumon from an anticoagulation clinic | Random blood glucose level (mmol/l) | 6.3 | |
| Sodium (mmol/l) | 138 | 132 | |
| Potassium (mmol/l) | 4.0 | 3.9 | |
| INR | 2.8 | 2.5 |
Points of concern: dizziness, dyspnoea, oedema/increase in weight, blood pressure
Possible treatment considerations based on separate Dutch CPGs:
Increase furosemide dosage. Patient’s rapid increase in weight, and dyspnoea at night, can indicate fluid retention, possibly insufficiently treated by the current dosage of furosemide; furosemide promotes the loss of excess fluid in patients with heart failure.20 Monitor serum electrolytes frequently, in view of the increased furosemide dosage and her decreased sodium values.
Enquire as to type of dizziness. There are several reasons for dizziness, for instance, dizziness due to orthostatic hypotension, or due to a side effect of the medications. Insight into the type (or cause) of dizziness can influence treatment.
Increase lisinopril dosage to control the blood pressure, and to improve the blood flow.20
Consider increasing the metoprolol dosage, but only after treatment for the heart failure exacerbation.20
Consider starting with spironolactone if adjusting the furosemide, lisinopril, and metoprolol dosages does not result in reduced fluid retention and dyspnoea.20
Appendix 4. Turner: description of fictionalised case vignette with possible treatment considerations
Vignette 4: Mr Turner (71 years old)
Mr Turner visits the GP with a severe pain attack in his big toe. It is too painful to even touch his toe. During the consultation, Mr Turner points out that he had experienced several attacks of severe pain in his foot; however, up until now, using paracetamol was often an adequate analgesic and, therefore, he had not mentioned it to his GP. This week, paracetamol could not alleviate the pain. A blood test demonstrated an elevated uric acid level, and considering his previous pain attacks Mr Turner was diagnosed with gout. Since 2008, Mr Turner has cardiac dysrhythmia and in 2012 he suffered a TIA. He also has high blood pressure. In 2014, his wife passed away, which resulted in depression. Paroxetine was prescribed, and he has been using paroxetine for 6 months.
| Prescribed medications | (Laboratory) test results | Visit (7 Oct 2014) | Current visit (3 Nov 2014) |
|---|---|---|---|
| Acenocoumarol from an anticoagulation clinic | Blood pressure (mmHg) | 150/92 | 148/91 |
| Paroxetine 20 mg o.d. | Ventricular rate (b.p.m.) | 92 | 92 |
| Metoprolol 50 mg o.d. | eGFR (ml/min/1.73 m2) | 49 | 49 |
| Hydrochlorothiazide 12.5 mg o.d. | Albumin/creatinine ratio (mg/mmol) | 2.6 | 2.6 |
| Simvastatin 40 mg o.d. | LDL cholesterol (mmol/l) | 2.4 | 2.4 |
| Omeprazole 20 mg o.d. | Fasting blood glucose level (mmol/l) | 4.8 | |
| Uric acid (mmol/l) | 0.46 | ||
| INR | 3.1 | 3.6 | |
| BMI (kg/m2) | 27 | 27 |
Points of concern: (pain due to) gout attack, blood pressure, depression treatment
Possible treatment considerations based on separate Dutch CPGs:
Stop omeprazole. It is unknown if the patient has gastric complaints, and the patient does not use an NSAID or a low-dose acetylsalicylic acid (LDASA), and therefore a proton pump inhibitor is not indicated.41
Start prednisolone 30 mg o.d. for 5 days. Short-term use of systemic corticosteroids can be effective in treating gout attacks, when NSAIDs are contraindicated.44
Add an ACE inhibitor. The recommended systolic blood pressure level of ≤140 mmHg is not achieved with the current dosage of metoprolol. It is recommended to stop the hydrochlorothiazide for 2–3 days, and then start again with the ACE inhibitor and hydrochlorothiazide.24
Monitor use of paroxetine. Enquire about effects of treatment and consider stopping or changing the medication if the patient does not perceive any effect. Long-term use of paroxetine is discouraged.45
Notes
Funding
The authors have declared no funding sources.
Ethical approval
According to Dutch legislation, interviewing healthcare professionals regarding their professional beliefs does not need the approval of an external ethics committee.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received December 18, 2015.
- Revision requested January 23, 2016.
- Accepted March 15, 2016.
- © British Journal of General Practice 2016
REFERENCES
In this issue









Jump to section
- Top
- Article
- Abstract
- INTRODUCTION
- METHOD
- RESULTS
- DISCUSSION
- Acknowledgments
- Appendix 1. Adams: description of fictionalised case vignette with possible treatment considerations
- Appendix 2. Brown: description of fictionalised case vignette with possible treatment considerations
- Appendix 3. Smith: description of fictionalised case vignette with possible treatment considerations
- Appendix 4. Turner: description of fictionalised case vignette with possible treatment considerations
- Notes
- REFERENCES
- Figures & Data
- Info
- eLetters
More in this TOC Section
Related Articles
Cited By...

