


INTRODUCTION
An acute red eye is a common presentation to primary care. The majority of these can be safely managed with expectant waiting or topical antibiotics. Children with red eyes are more challenging to assess, as the history may be unclear and examination is often difficult. This article presents an example of a serious ocular condition in a child with a red eye and considers the learning points from this case.
CASE HISTORY
A 4-year-old boy presented to primary care with a sticky red left eye, new-onset squint, and possible abnormal red reflex. He was difficult to examine and so was managed initially with chloramphenicol drops and referred routinely to ophthalmology. While awaiting his eye appointment he continued to be reviewed in primary care, although the presenting condition remained largely unchanged.
He was seen in ophthalmology outpatients 3 months after the onset of symptoms. On examination he was found to have a vision of 6/60 in the affected eye, blepharospasm (difficulty opening the eyelids), photophobia, pain, ptosis, and lid swelling. Further observation revealed a poor red reflex with scarring of the cornea. The superior cornea had localised green fluorescein staining, indicating an epithelial defect in a location frequently associated with a subtarsal foreign body (Figure 1). An examination under anaesthetic was performed and a subtarsal foreign body was found and removed. Postoperatively, the vision gradually improved to 6/18 with glasses wear to correct astigmatism, and patching of the right eye to treat amblyopia.
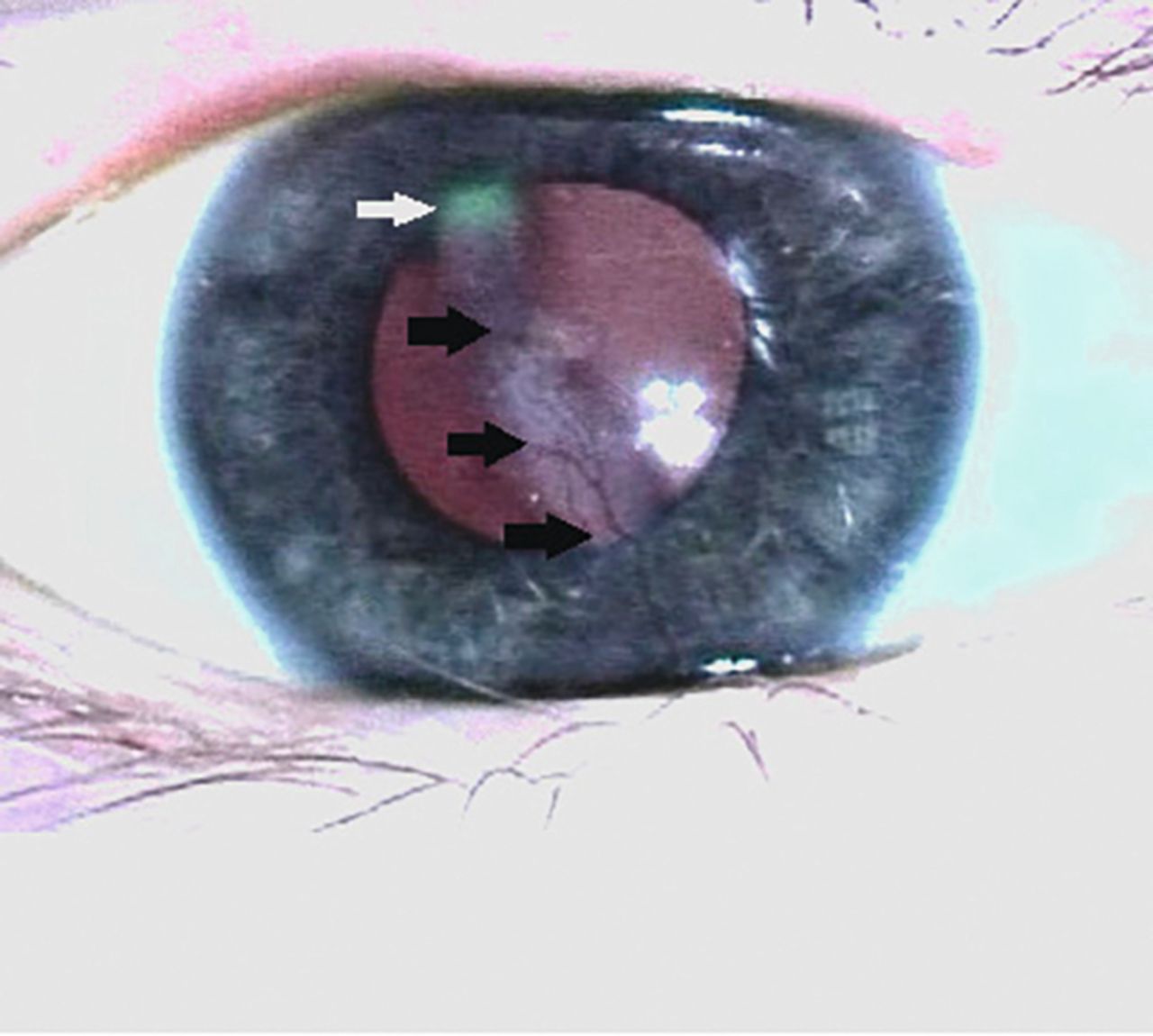
Examination findings of right eye.
Black arrows show white linear corneal scarring. White arrow shows green fluorescein staining.
OCULAR REDNESS IN CHILDREN
A red eye in a child can be due to a number of different underlying causes (Box 1). It is often possible to distinguish between benign and serious causes of red eye in the primary care setting by careful history taking and examination with a direct ophthalmoscope. A red eye is most commonly due to conjunctivitis, which can be safely managed in primary care with observation if the discharge is watery (allergic and viral conjunctivitis are common and frequently self-limiting), or topical antibiotics if discharge is purulent. Occasionally, a more worrying ocular condition may present, and a number of red flags can guide clinicians as to whether further urgent referral to secondary care is indicated (Box 2).
Common causes of paediatric red eye1
Viral conjunctivitis.
Bacterial conjunctivitis.
Corneal abrasion/trauma.
Subconjunctival haemorrhage.
Blepharitis.
Periorbital cellulitis.
Allergic eye disease.
Corneal ulcer.
Uveitis.
Episcleritis.
Red flags for the paediatric red eye
Staining of the cornea.
Corneal haze/opacity.
Abnormal red reflex.
Photophobia/significant pain.
Lid swelling/blepharospasm.
Associated new-onset squint.
Reduced visual acuity.
Failure to improve by 2 weeks.
Contact lens use (older children).
Abnormal pupillary reaction.
Difficulty in examination.
History of high-velocity injury.
Paediatric history taking can be challenging, and in some circumstances the examination findings may yield more useful information than the history. A recent history of viral illness, discharge, and discomfort point towards a diagnosis of conjunctivitis, although significant pain and photophobia are unusual in this setting. A history of trauma may be helpful, but it may be difficult to establish the mechanism of injury, thus increasing the chances of a delay in diagnosis.2 The absence of a history of trauma does not exclude injury, as children may be unwilling to disclose an event that may get them into trouble.1 Reduced vision in a child can lead to rapid decompensation of a squint.
Visual assessment is helpful, although this may not be possible in the primary care setting in pre-school children. If there is concern that the vision is reduced in the context of a red eye then urgent referral to ophthalmology should occur. Fluorescein 2% drops are a useful examination tool, and are stocked in some GP practices. They do not require refrigeration. Staining is carried out by instilling 1 drop of 2% fluorescein into the inferior fornix of the affected eye. This is done approximately 1 minute before examination to allow time for any ocular surface damage to take up the dye. If too much fluorescein is put in the eye, a tissue can be used to remove any excess. It is important to give the drop time to work, as areas of staining can be missed if the patient is examined too hastily. If staining of the cornea is present, an explanation for this should be sought. The pattern of staining may be helpful in establishing the cause for the red eye: traumatic abrasions are usually irregular in shape; dendritic ulcers are often branching in appearance; and linear vertical staining or scarring on the superior cornea suggests a foreign body under the superior eyelid. If whitish discoloration of the cornea is seen, then a diagnosis of infectious keratitis, or scarring, should be considered, and onward urgent referral is recommended. If fluorescein is not available, then further referral should occur if there is concern, particularly if any red flags are present.
It is useful to assess the red reflex in children with red eyes. Causes of an abnormal red reflex include: scarring or infection of the cornea; cataract or opacities within the vitreous; or retinal pathology (including tumours). It is also important to assess the pupillary reaction, ensuring that both pupils are equal, round, and react normally to light. Pupil abnormalities may be seen in trauma, where the affected eye can have a dilated pupil due to traumatic mydriasis or third-nerve palsy, or may be irregular due to a penetrating injury. Uveitis may also result in irregular or asymmetric pupils due to synechiae (stuck-down pupils due to inflammation).
Although the majority of children presenting with a red eye are not victims of abuse or neglect, up to 3% of traumatic eye injuries in presenting children can be non-accidental in nature.3 If any uncertainty exists then referral to an ophthalmologist and a paediatrician should occur for further assessment.
In the case described, a subtarsal foreign body caused redness and irritation, which was initially diagnosed as conjunctivitis. Subtarsal foreign bodies account for over 8% of cases of eye trauma presenting to eye casualties,4 and in the authors’ walk-in eye casualty service the incidence is approximately 1 in 3000 per year. In primary care it may be possible to evert the lid in compliant older children after instillation of local anaesthetic drops and remove any foreign body5 with a cotton bud. If the foreign body can be successfully removed in primary care the patient does not require ophthalmic input. This is provided there is no history of exposure to an environment where power tools were used, or hammering was occurring, which may result in a high-velocity foreign body capable of penetrating the eye.
A number of red flags were present in this case that warranted urgent referral (pain, photophobia, blepharospasm, and a new-onset squint). The learning points of this article are considered in Figure 2.

{kind=link}
{kind=link}
Learning points.
Notes
Patient consent
The patient’s parent consented to the publication of this article and the images.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received April 29, 2016.
- Revision requested May 31, 2016.
- Accepted July 4, 2016.
- © British Journal of General Practice 2016
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

