


Abstract
Background Accurate assessment of the need for admission is challenging in out-of-hours (OOH) primary care. Understanding more about patient contacts where the decision to continue care in the community may have been incorrect could assist clinicians in assessing clinical risk.
Aim To define the population contacting OOH primary care who are at higher risk of re-presenting to this service and requiring urgent transfer to secondary care within 3 days of their initial contact.
Design and setting Retrospective service evaluation of 4 years of patient contacts with Oxfordshire OOH primary care.
Method Multivariable logistic regression was used to evaluate demographic and service delivery factors associated with increased risk of delayed escalation to secondary care.
Results Almost 1% of 496 931 patients contacting OOH primary care required escalation to secondary care within 3 days. Of these, 68.5% were initially discharged with no follow-up or advice to contact their GP; 14.7% were initially referred to secondary care. The odds of requiring escalation were increased with age (odds ratio [OR] 1.010; 95% confidence interval [CI] = 1.009 to 1.011; P<0.001), more frequent prior use of the OOH service (OR 1.016; 95% CI = 1.010 to 1.021; P<0.001), and presenting during periods of low call volume (OR 0.880; 95% CI = 0.857 to 0.904; P<0.001).
Conclusion Older, prior users of the service, presenting at less busy times, are at greater risk of requiring secondary care referral from the OOH service within 3 days of their initial contact. These higher-risk patient groups might benefit from active follow-up by the OOH service.
INTRODUCTION
The provision of primary care services outside core contracted hours is fundamental to the operation of the NHS.1 In 2013–2014, out-of-hours (OOH) GP services in England handled around 5.8 million cases, of which 3.3 million were face-to-face consultations, including 800 000 home visits.2 A challenge for OOH primary care is accurate assessment of clinical risk to guide a decision over whether to escalate a patient’s care to hospital settings or to continue care in the community with advice on seeking further care (termed ‘safety netting’). This assessment is more difficult in OOH primary care compared with in-hours routine general practice because of a lack of detailed medical records, lack of familiarity with the patient, increased use of telephone rather than face-to-face assessment, lack of support from trusted colleagues, and a higher proportion of vulnerable patients with more complex care needs.3
Furthermore, the decision to escalate care is complex. Decisions to admit patients from US emergency departments have been shown to be influenced by non-medical factors in over half of cases.4 Age, sex, and ethnic group were associated with increased emergency admissions in a recent cross-sectional survey of admissions from in-hours general practice.5 In addition, an individual GP’s tolerance of risk affects the number of admissions made out-of-hours.6 These studies do not, however, offer insight into improving recognition of serious illness in OOH primary care. Mortality rates following OOH primary care assessment point to the higher prevalence of serious illness in this clinical population. In a region of Norway, 25% of patients had consulted local OOH primary care in the 4 weeks before their death, which was unexpected in a quarter of cases.7 There has been almost no research into other health outcomes following contact with OOH services.
Evidence that informs improvement in OOH care should consider recognition of patients who are at higher risk of clinical deterioration. Although safety-net advice can be given to all patients who are not escalated at initial assessment, identification of a patient group with a high likelihood of deterioration could drive alternative service models, including active review, rather than the default passive option of patient-initiated request for re-assessment. High-profile failings in OOH care have resulted in part from a lack of active review models.8,9 Features identifying patients at higher risk of deterioration after initial assessment could be studied by examining those cases in which patients were kept at home following their initial assessment in OOH primary care and who re-attended within a short time period, having clinically deteriorated. This study undertakes a service evaluation using data from the Oxfordshire OOH service to examine the population of patients who returned to the service within 3 days of an initial assessment and required hospital-based care when re-assessed.
How this fits in
Out-of-hours (OOH) primary care is a challenging clinical environment with acute illness syndromes. This study is the first to examine the ‘failure rate’ of OOH where patients return to the service and require escalation to secondary care within 3 days of initial contact. Older patients seen at times of low call volume have a higher risk of requiring escalation within 3 days. OOH providers should consider opportunities to develop proactive monitoring for patients at risk of deterioration after initial assessment.
METHOD
The Oxfordshire out-of-hours electronic medical record was used to develop a database of patients presenting to the service over 4 years (June 2010 to August 2014). All patient identifiers were removed on entry to the database. Patients without an NHS number (14 572 patients) were not included in the database, as repeat visits to the service could not be assessed. The 75 patients who had presented more than 50 times to the service over a period of 4 years were censored at visit 50. Demographic data included age and Index of Multiple Deprivation (IMD) score.10 Service data included call volume, number of contacts before the index consultation, and time period.
Contact volume was assessed using the total number of contacts received for each hour of the day over the 4-year period. Contact volume was categorised as follows: low <2500, moderate 2500–5000, high ≥5000–10 000, and very high ≥10 000. The number of days’ difference was calculated using calendar days beginning at midnight. Patients who had two separate contacts with the service within the same 1-hour time period were excluded from the analysis. Where more than two contacts were made with the service within 3 days, the earliest contact was taken as the initial contact.
Demographic and service characteristics were determined that were independently associated with referral to secondary providers (hospital admission, emergency department referral, acute ophthalmology, or psychiatry referral, or 999 ambulance) at re-attendance to the OOH service within 3 days of their initial visit with multivariable logistic regression. Data on referral to secondary care providers from the in-hours GP or ambulance, or direct presentations to secondary care services, were not available to this analysis. Analyses were performed using SPSS (version 22).
Validation of clinical coding
At the end of each OOH consultation, clinicians assign at least one clinical code (for example ‘cardiac’), which were used in this study to determine clinical presentation for that contact. To validate the clinical codes applied by the OOH clinicians, estimates were made, based on previous coding validity studies,11 that 230 records would be required to establish the coding validity with a confidence level of 90% and 5% margin of error. A random selection of 230 records was obtained using SPSS, and the clinical code was compared by one author to the conclusion drawn by the clinician in the medical notes. The positive predictive value (PPV) of the clinical code for medical diagnosis or conclusion was 90%. If only those codes that positively described an established clinical presentation were assessed (for example, ‘cardiac’ but not ‘miscellaneous’ or ‘referred to acute trust’), the PPV was 97.5%.
RESULTS
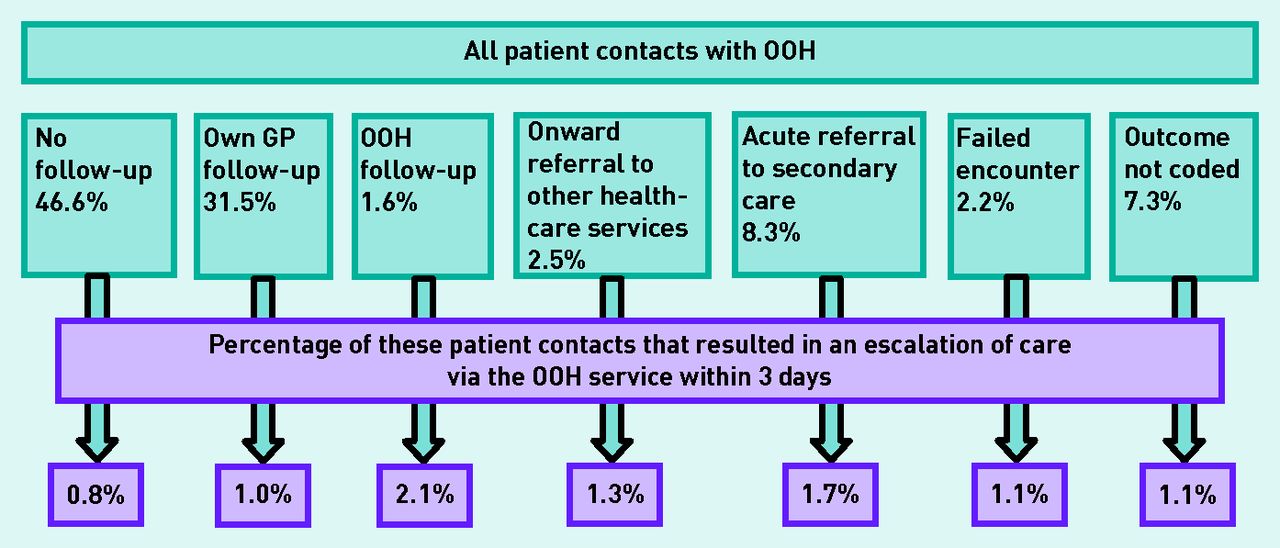
Of 496 931 presentations to the OOH service, 58.3% were female, with median age 35 years (interquartile range [IQR] 13–66 years). Of this population, 78% were discharged with no follow-up or advised to contact their own GP. Almost 1% (4832 cases, 4465 individuals) of this population (57.5% female) required escalation to secondary care providers within 3 days of their initial visit: the ‘delayed escalation’ population. The flow of the patients through the service is described in Figure 1. The demographics of the overall and ‘delayed escalation’ populations are described in Table 1.

{kind=link}
Outcomes of patient contacts with OOH primary care and the proportions of patient contacts with each outcome where escalation of care was required within 3 days.
OOH = out-of-hours.
Demographics of the overall population and ‘delayed escalation’ population
The ‘delayed escalation’ population made initial contact with the service most often on Saturdays (1837 out of 4832 contacts; 38%), although the risk of delayed escalation was greatest on Fridays (1.4% of total Friday contacts). Almost half (48.4%) of urgent referrals to secondary care at re-attendance were acute hospital admissions made directly to a specialty. Emergency department referrals accounted for 29.7%, 999 ambulances 18.3%, acute psychiatry 2.8%, and ophthalmology 0.8%.
Factors increasing risk of referral to secondary care within 3 days
Multivariable logistic regression was used to test which demographic and service delivery factors were associated with initial patient contacts that resulted in delayed escalation to secondary care within 3 days. All of the demographic factors available from the database were included, and service variables that uniquely identified features of service demographics. As contact volumes were universally lower in the overnight period, contact volume was included in the analysis without an additional variable for time period.
Significant factors were increasing age, higher frequency of attendance to the OOH service before this contact, and when presenting to the service during periods of low contact volumes, mostly in the overnight period (Table 2). The same factors were significant when the analysis was restricted to those patients who were not referred to secondary care following their initial contact (4122 patient contacts) (Appendix 1).
Factors included in logistic regression analysis
Risk of delayed escalation by clinical problem
Patients presenting with social, mental health, gastrointestinal, and cardiac problems carried the highest risk of re-presentation with deterioration, in addition to those contacted because of abnormal pathology results (Table 3).
Clinical presentations associated with highest risk of requiring ‘delayed escalation’
Clinical problems at the initial consultation and at re-attendance in the delayed escalation population
Table 4 displays the top 10 most common clinical presentations for the ‘delayed escalation’ patient group at their initial consultation and at re-attendance. The highest-frequency presentations were gastrointestinal, genitourinary, respiratory, and musculoskeletal at both the initial consultation and on re-attendance. More patients presented with surgical, cardiac, neurological, and respiratory problems at the contact that resulted in escalation of care.
The 10 most commonly assigned clinical codes on initial consultation and re-attendance
Risk of delayed escalation by consultation outcomes
Referral to acute psychiatric services was the outcome of contact with OOH that carried the greatest risk of re-assessment with hospital admission within 3 days. This suggests that patients were accepted for further assessment by the psychiatry services but were discharged back to community care within 3 days.
Other consultation outcomes associated with higher risk were referral to social services, 999 ambulance referrals, consultations where the patient left after triage but before definitive assessment, and patients where the OOH service had planned to follow-up their care (Table 5).
Consultation outcomes associated with the highest risk of requiring ‘delayed escalation’
Outcomes from the initial consultation
A third (32.2%) of ‘delayed escalation’ patient contacts were advised to see their own GP for review, and over a third (36.3%) were discharged with no follow-up planned. The proportions of patients given this advice in the overall population contacting OOH were 31.5% and 46.6%, respectively. Patients in the ‘delayed escalation’ group were referred to secondary care at their initial consultation almost twice as often as the overall population (14.7% versus 8.3%); these patients were discharged back to the community only to require escalation back to hospital within 3 days. In the group of patients referred at their initial contact, 42.5% were referred to hospital by emergency ambulance, 24.1% were acute hospital admissions made directly to a specialty, 27.5% were referred to the emergency department, and 4.6% and 1.3% were referred to acute psychiatry and acute ophthalmology, respectively.
Contacts were mainly during daytime weekend shifts (60.8%). Of the patients, 55.6% were female and the median age was 57 years (IQR 24–78 years).
DISCUSSION
Summary
Almost one per cent of patients required urgent admission to secondary care within 3 days of an initial consultation in this UK OOH primary care service. Patients who were older, had used the service more often, and presented to the service at times of low calls were at higher risk. Over two-thirds of the patients who required escalation of care after re-attending within 3 days were initially discharged with either no follow-up or advice to contact their own GP.
Patients presenting with social, mental health, gastrointestinal, and cardiac problems were at highest risk of requiring delayed escalation of care. The social descriptor is often used to indicate a functional decline, which means that the patient can no longer manage in their usual home environment without a clear medical cause. This may indicate that acute illness can initially present as a functional decline, particularly for frail, older patients with multimorbidity, and a medical diagnosis can become more manifest over ensuing days.
Strengths and limitations
This is the first assessment of factors associated with risk of clinical deterioration in UK OOH care. The evaluation included a large volume of patient contacts with validated clinical coding. An important limitation is that full data linkage with in-hours GP notes and Accident and Emergency or other urgent care contacts is not systematically available in the UK, therefore the present data are likely to significantly underestimate the number of patients who will be referred urgently to secondary care within 3 days, because many more will be referred by their usual GP. The percentage risk of delayed escalation was greatest for Friday contacts (1.4%), when patients are reliant on OOH primary care in event of deterioration within 3 days. This is likely to better approximate the true rate of re-presentation.
Comparison with existing literature
The present findings mirror research based in emergency department settings, where older adults use emergency services at a higher rate and are more likely to be admitted or to re-attend than younger adults.12 In an emergency department short-stay unit, age but not overnight presentation was associated with rapid re-presentation to acute care following discharge. The present finding that ‘gastrointestinal’ was the most common clinical presentation in this patient group matches prehospital triage research showing that ‘acute abdominal’ cases had the highest chance of being initially ‘undertriaged’ by telephone, and then upgraded to more severe on face-to-face assessment.13
Implications for research and practice
The present analysis suggests a number of measures that could reduce the number of patients who have delayed escalation to secondary care, which could be applied either separately or in combination.
Presentation at times of low call volume for the OOH service was associated with higher risk of ‘delayed escalation’. Periods of low call volume are commonly covered by smaller numbers of clinicians. Therefore, the pressures of the service may lead to deferred decision-making by telephone triage until more staff are available, for example, to offer a home visit the following day. Norwegian OOH GPs described the challenges of balancing practical issues and clinical need when offering home visits with limited clinician resources.14 The GP’s tolerance of risk has been shown to be an important factor for decisions about admission from OOH care. GPs self-rating as cautious refer more often than those rating themselves as good at living with risk and uncertainty.6 GPs choosing to work in overnight OOH shifts, which are considered to be more pressured, may be a selected group of clinicians who have higher risk tolerance. Increasing the number of clinicians available in this time period may allow more timely review of higher-risk patient groups and encourage more clinicians to consider these shifts.
Over two-thirds of the ‘delayed escalation’ population were discharged at their initial consultation and just 3.5% were offered follow-up by the OOH service. Active followup could allow OOH services to detect deterioration earlier, and offer the potential for enhanced input to meet clinical need without an emergency admission. The patient group targeted for follow-up should include older patients, particularly those presenting with unexplained functional decline, patients initially presenting overnight, and patients with mental health, cardiac, and gastrointestinal problems where there is diagnostic doubt. A records-based follow-up list, with a planned telephone review period of 12 or 24 hours, could be employed. This would be particularly beneficial over the weekend, when the OOH service has continuity of care, and could also allow secondary care to highlight patients requiring community follow-up after discharge.
Patients who had contacted the OOH service previously were more likely to require escalation of care within 3 days. In European OOH services these patients have been shown to have higher occurrences of chronic disease and psychiatric illness;15,16 these are populations in which the decision to admit is likely to be more challenging. Enhanced sharing of information with the in-hours GP practice could facilitate shared management plans and reduce the risk of deterioration out-of-hours. Similarly, the present finding that 14.7% of the ‘delayed escalation’ population had been referred to secondary care at their initial consultation suggests that feedback on the outcomes of admissions from the OOH service would be highly beneficial in informing further management of these challenging patients. At present, OOH clinicians have no access to feedback on the decisions they make regarding referral. They would not learn about subsequent referral to secondary care, an immediate discharge following an admission, or even, unless it was particularly noteworthy, a death. Without such feedback, clinicians are unable to learn from their experiences in this higher risk setting.
Improving the detection and management of patients who are on a declining trajectory requires research to understand the presenting features, the final diagnosis, and the outcome of escalation of care in this patient group. Improving care delivery through support for decision-making and follow-up models requires research into the type of clinicians used in OOH care pathways, availability of diagnostic testing, staffing levels at the time of assessment, and optimal timing of clinical review. This will allow OOH follow-up to be targeted at the highest-risk patients, and will enable development of decision support such as use of point-of-care testing, which could identify conditions notoriously difficult to detect clinically at an early stage (for example, acute kidney injury), as well as reduce inappropriate referral decisions. This will allow understanding of the impact of clinician experience and pressure on referral decisions and evaluation of whether the admissions were clinically justified or could have been prevented with alternative management strategies.
The present findings need to be confirmed and extended through multicentre studies or collaborations between different OOH service providers covering different UK populations that share data on re-attendance and escalation. Furthermore, definitive clinical outcome data after escalation to secondary care will be most efficiently gathered through local data-sharing partnerships between an OOH provider and secondary care organisations to enable linkage of patient data. New models of care incorporating active review by the OOH service will also need to be evaluated alongside routine care from different OOH service providers to assess their clinical-and cost-effectiveness. It is appreciated that increasing the number of GPs available in OOHs services, however desirable, is not easy at the present time. Understanding how to support decision-making by different healthcare professionals assessing patients in an OOH service, focusing more directly on those patients who are particularly at risk of missing a needed referral, and putting in place more active follow-up when such patients are seen, are potential strategies, however, to improve the safety of OOH primary care.
Acknowledgments
The authors acknowledge the input and assistance of Ms Helen Hunt, Urgent and Ambulatory Care Service Clinical Lead for Oxford Health NHS Foundation Trust, in this project.
Appendix 1. Clinical presentations associated with highest risk of requiring ‘delayed escalation’ in the subgroup of patients where care was not escalated on their initial contact
| OR (95% CI) | Wald | P-value | |
|---|---|---|---|
| Age | 1.010 (1.009 to 1.011) | 323.16 | 0.000 |
| Sex | 1.035 (0.972 to 1.103) | 1.16 | 0.281 |
| Deprivation | 1.000 (0.997 to 1.003) | 0.02 | 0.886 |
| OOH contacts before index consultation | 1.018 (1.012 to 1.024) | 38.8 | 0.000 |
| Call volume | 0.902 (0.877 to 0.929) | 49.0 | 0.000 |
OOH = out-of-hours. OR = odds ratio.
Notes
Funding
Gail N Hayward was funded by an NIHR Academic Clinical fellowship and Academic Clinical Lectureship while working on this study. Daniel S Lasserson is funded by the NIHR Oxford Biomedical Research Centre and NIHR Oxford Collaboration for Leadership in Applied Health Research and Care (CLAHRC). Charles Vincent is funded by the Health Foundation. No additional funding was sought for this study. The authors’ funders had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. The researchers are entirely independent from the funders.
Ethical approval
Ethical approval was not required for this study. Oxford Health NHS Foundation Trust evaluated the protocol and prospectively approved the work as a service evaluation and quality improvement project, conducted by Gail N Hayward who was part of the direct care team.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received May 16, 2016.
- Revision requested June 7, 2016.
- Accepted August 2, 2016.
- © British Journal of General Practice 2017
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

