


Article Figures & Data
Figures
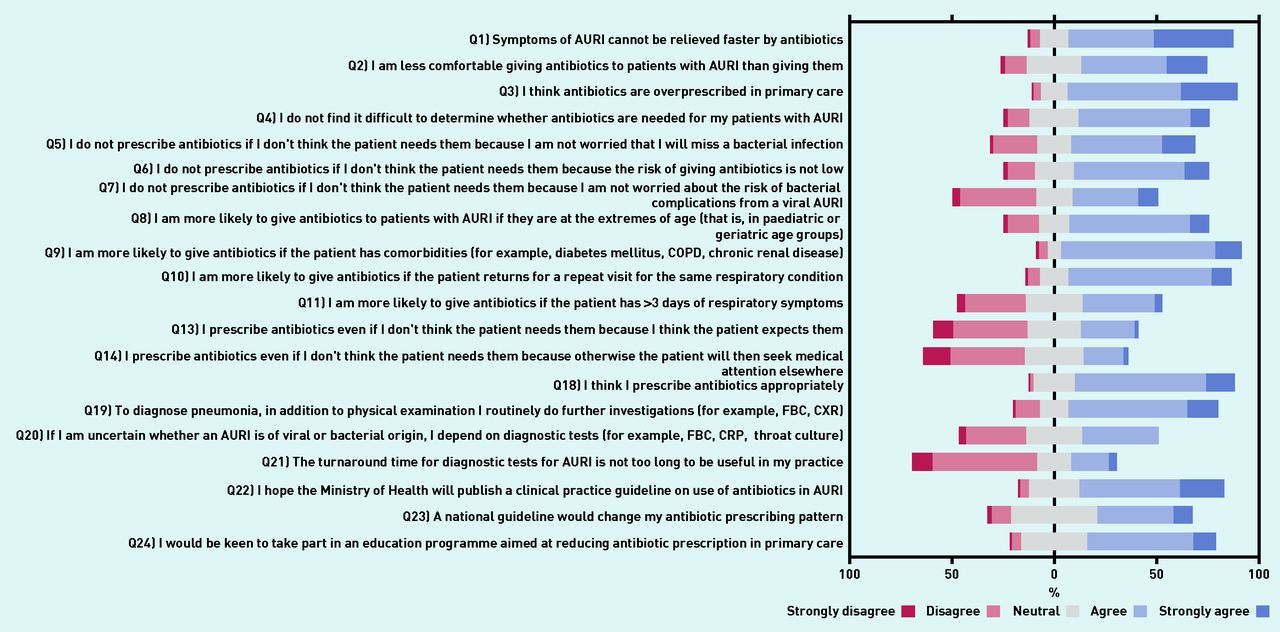
- Figure 1.
Five-point Likert scale responses. AURI = acute upper respiratory tract infections. COPD = chronic obstructive pulmonary disease. CRP = C-reactive protein. CXR = chest X-ray. FBC = full blood count.
- Figure 2.
Four-point Likert scale responses. AURI = acute upper respiratory tract infections.
- Appendix 2.
Scree plot of number of factors and the eigenvalues. Factor 1 = medical knowledge and clinical competency; Factor 2 = conservative practice; Factor 3 = GPs’ perceived patient expectations; Factor 4 = good clinical practice; Factor 5 = availability of diagnostic tests; Factor 6 = desire to improve clinical practice — this was also moderately correlated with perceived patient expectations (r = 0.42).



{kind=link}
{kind=link}
{kind=link}
Tables
Private sector (n= 351) Public sector (polyclinic) (n= 76) P-value Postgraduate family medicine qualifications (n= 148) Primary medical qualification only (n= 279) P-value Place of practice, n (%) Private (solo) N/A N/A 44 (29.7) 67 (24.0) Private (group) N/A N/A 61 (41.2) 179 (64.2) Polyclinic N/A N/A 43 (29.1) 33 (11.8) <0.01 Number of years from medical school graduation n (%) ≤5 years 2 (9.1) 20 (90.9) 32 (72.7) 12 (27.3) 6 to 15 years 16 (36.4) 28 (63.6) 2 (9.1) 20 (90.9) >15 years 333 (92.2) 28 (7.8) <0.01 114 (31.6) 247 (68.4) <0.01 Highest medical qualification, n (%) Postgraduate family medicine qualifications 105 (29.9) 43 (56.6) <0.01 N/A N/A N/A Primary medical qualification only Reference N/A N/A N/A GPs from private practice (n= 351) GPs from polyclinic (n= 76) P-value What percentage of AURI are caused by viruses? n (%) <20% 14 (5.0) 0 (0) 20–39% 21 (6.0) 1 (1.3) 40–59% 107 (30.5) 18 (23.7) 60–79% 4 (1.1) 2 (2.6) >80% 205 (58.4) 55 (72.4) 0.03 There is a scoring system to assess the likelihood of streptococcal infection in pharyngitis/tonsillitis (modified Centor score), n (%) 163 (46.4) 60 (78.9) <0.01 Purulence of nasal discharge/sputum (yellow/green) indicates increased likelihood of bacterial infection, n (%) 197 (56.1) 20 (26.3) <0.01 I think empirical antibiotics are indicated in the following acute respiratory infections, n (%): Acute otitis media 315 (89.7) 62 (81.6) 0.05 Rhinitis 12 (3.4) 1 (1.3) 0.48 Acute sinusitis 281 (80.1) 53 (69.7) 0.07 Laryngitis/pharyngitis 92 (26.2) 11 (14.5) 0.04 Tonsillitis 332 (94.6) 58 (76.3) <0.01 Tracheobronchitis 199 (56.7) 29 (38.2) <0.01 What is the proportion of patients with AURI to whom you prescribe antibiotics? n (%) Low prescriber (<20%) 139 (39.6) 61 (80.3) <0.01 What is the most serious problem you foresee in overprescription of antibiotics? n (%) Drug–drug interaction 0 (0) 1 (1.3) Increased antibiotic resistance 319 (90.9) 71 (93.4) Increased costs 2 (0.6) 1 (1.3) Possible side effects/allergies/adverse events 25 (7.1) 3 (3.9) Other 5 (1.4) 0 (0) 0.18 AURI = acute upper respiratory tract infections.
No. Factor characteristics Survey questions included in the factor loading Factor scores, mean (SD) α High prescribing Low prescribing 1 Medical knowledge and clinical competency Q1) Symptoms of AURI cannot be relieved faster by antibiotics −0.36 (0.06) 0.41 (0.06) 0.74 Q2) I am less comfortable giving antibiotics to patients with AURI than giving them Q3) I think antibiotics are overprescribed in primary care Q4 I do not find it difficult to determine whether antibiotics are needed for my patients with AURI Q5) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried that I will miss a bacterial infection Q6) I do not prescribe antibiotics if I don’t think the patient needs them because the risk of giving antibiotics is not low (for example, an allergic reaction) Q7) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried about the risk of bacterial complications from a viral AURI 2 Conservative practice (giving antibiotics ‘to be on the safe side’) Q8) I am more likely to give antibiotics to patients with AURI if they are at the extremes of age (that is, in paediatric or geriatric age groups) 0.12 (0.06) −0.13 (0.08) 0.66 Q9) I am more likely to give antibiotics if the patient has comorbidities (for example, diabetes mellitus, COPD, chronic renal disease) Q10) I am more likely to give antibiotics if the patient returns for a repeat visit for the same respiratory condition Q11) I am more likely to give antibiotics if the patient has >3 days of respiratory symptoms 3 GPs’ perceived patient expectations Q12) If I do not prescribe antibiotics to my patients with AURI, they will usually ask for them −0.06 (0.07) 0.07 (0.07) 0.61 Q13) I prescribe antibiotics even if I don’t think the patient needs them because I think the patient expects them Q14) I prescribe antibiotics even if I don’t think the patient needs them because otherwise the patient will then seek medical attention elsewhere 4 Good clinical practice Q15) If I don’t think my patient needs antibiotics, I will not prescribe them −0.31(0.07) 0.35 (0.07) 0.64 Q16) If a patient who does not need antibiotics asks for them, I will explain to them why I think they do not need them Q17) I am able to convince my patients who do not need antibiotics that they will not benefit from them Q18) I think I prescribe antibiotics appropriately 5 Availability of diagnostic tests Q19) To diagnose pneumonia, in addition to physical examination I routinely do further investigations (for example, FBC, CXR) −0.15 (0.06) 0.17 (0.08) 0.62 Q20) If I am uncertain whether an AURI is of viral or bacterial origin, I depend on diagnostic tests (for example, FBC, CRP, throat culture). Q21 The turnaround time for diagnostic tests for AURI infections is not too long to be useful in my practice 6 Desire to improve clinical practice Q22) I hope the Ministry of Health will publish a clinical practice guideline on use of antibiotics in AURI −0.16 (0.07) 0.18 (0.07) 0.73 Q23) A national guideline would change my antibiotic prescribing pattern Q24) I would be keen to take part in an education programme aimed at reducing antibiotic prescription in primary care AURI = acute upper respiratory tract infections. COPD = chronic obstructive pulmonary disease. CRP = C-reactive protein. CXR = chest X-ray. FBC = full blood count.
Univariate OR (95% CI) P-value Multivariable aOR (95% CI)a P-value Factor 1: Medical knowledge and clinical competency 2.5 (2.0 to 3.3) <0.01 3.2 (2.4 to 4.3) <0.01 Factor 2: Conservative practice (giving antibiotics ‘to be on the safe side’) 0.8 (0.6 to 0.9) 0.01 0.7 (0.5 to 0.9) <0.01 Factor 3: GPs’ perceived patient expectations 1.1 (0.9 to 1.4) 0.21 − − Factor 4: Good clinical practice 2.1 (1.7 to 2.7) <0.01 2.7 (2.0 to 3.6) <0.01 Factor 5: Availability of diagnostic tests 1.4 (1.1 to 1.7) <0.01 1.4 (1.1 to 1.8) <0.01 Factor 6: Desire to improve clinical practice 1.4 (1.2 to 1.7) <0.01 1.5 (1.2 to 1.9) <0.01 aOR = adjusted odds ratio.
↵a Adjusted for practice type.
Variable list Type of variable Where is your current place of medical practice? Categorical (3 levels) How long ago did you graduate from medical school? Categorical (3 levels) Where did you attend medical school? Binary What is your highest medical qualification? Categorical (4 levels) What percentage of AURI are caused by viruses? Scale (1–5) What is the proportion of patients with AURI to whom you prescribe antibiotics? Scale (1–5) Q1) Symptoms of AURI cannot be relieved faster by antibiotics Scale (1–5) Q2) I am less comfortable giving antibiotics to patients with AURI than giving them Scale (1–5) Q3) I think antibiotics are overprescribed in primary care Scale (1–5) Q4) I do not find it difficult to determine whether antibiotics are needed for my patients with AURI Scale (1–5) Q5) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried that I will miss a bacterial infection Scale (1–5) Q6) I do not prescribe antibiotics if I don’t think the patient needs them because the risk of giving antibiotics is not low Scale (1–5) Q7) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried about the risk of bacterial complications from a viral AURI Scale (1–5) Q8) I am more likely to give antibiotics to patients with AURI if they are at the extremes of age (that is, in the paediatric or geriatric age groups) Scale (1–5) Q9) I am more likely to give antibiotics if the patient has comorbidities (for example, diabetes mellitus, COPD, chronic renal disease) Scale (1–5) Q10) I am more likely to give antibiotics if the patient returns for a repeat visit for the same respiratory condition Scale (1–5) Q11) I am more likely to give antibiotics if the patient has more than 3 days of respiratory symptoms Scale (1–5) Q12) If I do not prescribe antibiotics to my patients with AURI, they will usually ask for them Scale (1–4) Q13) I prescribe antibiotics even if I don’t think the patient needs them because I think the patient expects it Scale (1–5) Q14) I prescribe antibiotics even if I don’t think the patient needs them because otherwise the patient will then seek medical attention elsewhere Scale (1–5) Q15) If I don’t think my patient needs antibiotics, I will not prescribe them Scale (1–4) Q16) If a patient who does not need antibiotics asks for them, I will explain to them why I think they do not need them Scale (1–4) Q17) I am able to convince my patients who do not need antibiotics that they will not benefit from them Scale (1–4) Q18) I think I prescribe antibiotics appropriately Scale (1–5) Q19) To diagnose pneumonia, in addition to physical examination I routinely do further investigations (for example, FBC, CXR) Scale (1–5) Q20) If I am uncertain whether an AURI is of viral or bacterial origin, I depend on diagnostic tests (for example, FBC, CRP, throat culture) Scale (1–5) Q21) The turnaround time for diagnostic tests for AURI is not too long to be useful in my practice Scale (1–5) Q22) I hope the Ministry of Health will publish a clinical practice guideline on the use of antibiotics in AURI Scale (1–5) Q23) A national guideline would change my antibiotic prescribing pattern Scale (1–5) Q24) I would be keen to take part in an education programme aimed at reducing antibiotic prescription in primary care Scale (1–5) AURI = acute upper respiratory tract infections. COPD = chronic obstructive pulmonary disease. CRP = C-reactive protein. CXR = chest X-ray. FBC = full blood count.
Questions were either on a 4-point (1 = never, 2 = infrequently, 3 = frequently, 4 = always) or a 5-point Likert scale (range from 1 = strongly disagree to 5 = strongly agree).
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

