


Abstract
Background GPs prescribe topical corticosteroids to patients with chronic chilblains despite poor evidence for their effectiveness. The authors of the current study therefore decided to assess the effectiveness of topical steroids in a primary care setting.
Aim To assess the effectiveness of topical application of betamethasone valerate 0.1% cream in patients with chronic chilblains.
Design and setting A placebo-controlled, double-blind, crossover, randomised clinical trial in a Dutch primary care setting.
Method The study population consisted of 34 participants suffering from chronic chilblains. Intervention was topical application of betamethasone valerate 0.1% cream twice a day for 6 weeks compared with placebo. Primary outcome was the visual analogue scale on complaints (VOC). Secondary outcome was the visual analogue scale on disability (VOD). Both were assessed with a diary of daily scores on a 100 mm visual analogue scale. The authors took ambient temperatures into account, checked for a carry-over effect, performed additional analysis, and monitored adverse effects.
Results On the primary outcome mean VOC, there was a difference of 0.56 mm (95% confidence interval [CI] = −2.88 to 3.99 mm) in favour of placebo (P = 0.744). On the secondary outcome mean VOD, there was a difference of 0.88 mm (95% CI = −2.22 to 3.98 mm) in favour of placebo (P = 0.567). This study found no carry-over effect and no adverse effects.
Conclusion In this study, topical betamethasone was not superior to placebo in the treatment of chronic chilblains. Topical betamethasone should not be used for chronic chilblains without new evidence.
INTRODUCTION
Chronic chilblains are cold-induced painful or itching lesions on the fingers, feet, ears, or thighs. The condition occurs throughout the world during the winter months when daily mean temperatures drop below 12–15°C.1 Prevalence reported by the Netherlands Institute for Health Services Research (NIVEL) varies between 0.9 per 1000 and 1.7 per 1000 depending on year-to-year variation and coding issues; the condition is more common among females than males (prevalence 0.9–2.1 per 1000 and 0.6–1.2 per 1000, respectively) (NIVEL, personal communication, 2016). Patients report serious restrictions in daily life and urgently feel the need for an effective treatment.2 A literature study updated to 15 March 2016 reveals that vitamin D3, corticosteroid-containing cream, nifedipine, and pentoxifylline, together with a wide range of other therapies, are used to treat the symptoms of patients with chronic chilblains.3,4 Two of the current authors found that vitamin D3 was not superior to placebo.5 GPs advise topical corticosteroids for patients suffering from chilblains.6–10 Only one previous study evaluating the effectiveness of topical steroids in patients with chilblains has been published.11 This case-series with topical fluocinolone provides some evidence for the effectiveness of topical steroids for chronic chilblains but the current discussion on the reliability and reproducibility of original studies calls into question the soundness of recommendations based on it.12 As patients suffering from chilblains usually contact their GP for help, the authors decided to assess the effectiveness of topical corticosteroids in a primary care setting. Topical betamethasone was chosen because fluocinolone cream is not available in the Netherlands.
The aim of this study was to assess the proposed superiority of the topical application of betamethasone valerate 0.1% cream twice a day for 6 weeks compared with placebo cream in patients with chronic chilblains in a primary care setting.
METHOD
Trial design
The authors conducted a placebo-controlled, double-blind, crossover, randomised clinical trial in a primary care setting (Netherlands National Trial Register: number NTR 2171). A washout period was not included in the design because, for obvious reasons, the study was dependent on the winter months. A washout period would have caused too long a research period per participant and problems with high ambient temperatures in spring. Instead this study checked for a possible carry-over effect.
Participants
The study population consisted of consecutively recruited participants who suffered from chronic chilblains during the winters of 2010 to 2012. Participants volunteered after being informed about the trial by their GP during a consultation.
How this fits in
Chronic chilblains are cold-induced painful or itching lesions on the fingers, feet, ears, or thighs. The prescription of topical steroids for patients with chilblains finds support in one study. The current randomised, placebo-controlled trial does not confirm the conclusions of this study. Topical betamethasone should not be used in the treatment of chronic chilblains without new evidence.
The authors included participants aged ≥18 years with complaints of chronic chilblains lasting ≥3 weeks. The diagnosis (International Classification of Primary Care [ICPC] A88.01) was confirmed by one author, based on commonly used diagnostic criteria: complaints emerging in the winter months with itching and/or painful purple-blue discoloured lesions on fingers and/or toes and/or other localisations on the feet and/or on the lateral side of the thigh, without a history of complaints persisting in the summer months.1,7 The validity of the confirmation of the diagnosis had previously been demonstrated.5 The authors excluded people with a known rheumatic disorder (for example, rheumatoid arthritis or systemic lupus erythematosus), those who were using nifedipine or other calcium antagonist, those who had been using a corticosteroid-containing cream in the previous 4 weeks, and females who were pregnant or lactating.
Intervention
The intervention to be compared with placebo consisted of topical application of betamethasone 0.1% cream twice a day. The research medication (betamethasone valerate 0.1% cream and placebo) was produced and certified by an independent pharmacy: Pharmacy Waterland Oost, Volendam, the Netherlands.
Outcomes
Primary outcome was the difference between the visual analogue score (VAS) on complaints (VOC) scale in the betamethasone cream and placebo cream groups, respectively, after 6 weeks of treatment. VOC was assessed by a diary and defined as the 100 mm VAS score on pain or the VAS score on itch, depending on which item had the highest value at the moment of sampling. VOC was calculated using the mean value of the last 7 consecutive days of the 6-week treatment period.
Secondary outcome was the difference between the VAS on disability (VOD) score in the betamethasone cream and placebo cream groups, respectively, after 6 weeks of treatment. VOD was assessed by a diary and defined as the VAS score on inability to function normally in daily life. VOD was calculated using the mean value of the last 7 consecutive days of the treatment period.
Additionally, the chilblain lesions were assessed during face-to-face consultations. Redness, purpleness, oedema, and ulceration of the lesions were scored by one author on a VAS for each item. The authors monitored for any adverse effects from the two therapies (skin irritation and signs of skin atrophy).
Sample size
Sample size calculation was based on the following premises. In an earlier study on the effectiveness of vitamin D3 with 33 participants recruited in a similar way, two of the current authors observed a baseline VOC of 27.97 mm (standard deviation [SD] 18.82).5 An estimate was used of the correlation between two VAS scores from the same individual on two occasions of 0.5. Treatment effect was considered to be clinically relevant in the case of a 10 mm decrease in the VOC.
Based on use of a t-test for the difference between two dependent means, one-tail testing, α 0.05, and β 0.10 (power 90%) the authors calculated a minimum sample size of 32 participants.
Randomisation, blinding, and treatment allocation
Block randomisation with a block size of 10 was used to assign one of the two arms (placebo cream first or betamethasone cream first) to research medication sets with consecutive therapy numbers. This procedure was performed by the pharmacy that produced and issued the research medication sets blind to both research personnel and participants. Treatment allocation was ensured by the similarity of the pharmaceutical products and packaging between the betamethasone cream and placebo cream, which were indistinguishable. Consecutively recruited participants received research medication sets with consecutive therapy numbers. The randomisation key was only released after the last subject had left the study.
Study procedures
The participants were randomised over two arms:
Arm 1: No creams for 1 week to collect baseline data (phase 0), followed by topical application of betamethasone 0.1% cream twice a day for 6 weeks (phase 1), followed by topical application of placebo cream twice a day for 6 weeks (phase 2).
Arm 2: No creams for 1 week to collect baseline data (phase 0), followed by topical application of placebo cream twice a day for 6 weeks (phase 1), followed by topical application of betamethasone 0.1% cream twice a day for 6 weeks (phase 2).
The measuring instrument was a diary to be completed by the subject during the full 13-week research period. Each day the complaints (pain and itch) and disability in normal functions of daily life were documented using a 100 mm VAS for each item. Each day the mean outside air temperature, provided by the Royal Netherlands Meteorological Institute, was documented.
The authors performed six face-to-face assessments: intake (T1), end of week 1 (T2), end of week 4 (T3), end of week 7 (T4), end of week 10 (T5), and end of week 13 (T6). During face-to-face assessments the diary was checked for completeness, therapy compliance was checked by weighing remaining cream, and remaining lesions were documented.
Statistical analysis
The analysis was intention to treat. The authors performed analysis of the primary and secondary outcomes using the two-stage model originally proposed by Grizzle and correcting for temperature changes in the research period for each participant with a mixed effects model (Grizzle’s model using the mixed procedure with random effect, SAS PROC MIXED, SAS version 9.2).13,14 Additional analyses were undertaken and adverse effects monitored using a two sample paired t-test.
RESULTS
Characteristics of the populations
The flowchart (Figure 1) shows the procedure for including participants.
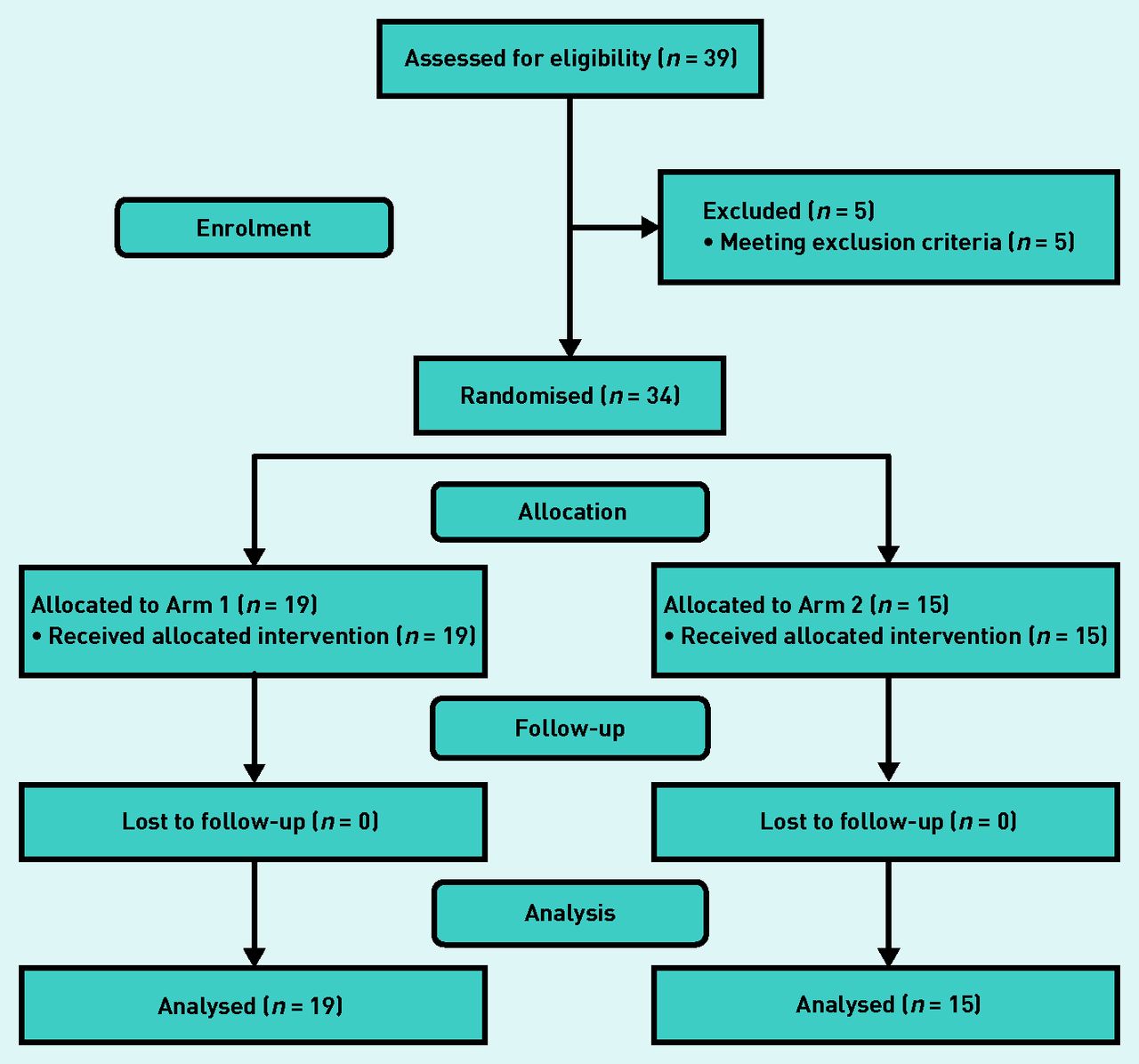
Flowchart for patient inclusion.
Data for 34 participants were available for analysis. The participants had a mean age of 53 years (SD 14.1), 19 were female, and 15 male. Mean duration of complaints at intake was 7 weeks (SD 4.2). At baseline mean VAS score on complaint was 26.80 mm (95% CI = 24.04 to 29.57) and mean VAS score on disability was 17.55 mm (95% CI = 14.90 to 20.20). Eleven participants suffered from a comorbidity that might have been relevant. Five participants smoked. Four participants used possibly relevant drugs (Table 1). Diaries were conscientiously completed. No face-to-face assessments were missed.
Baseline data
Outcomes
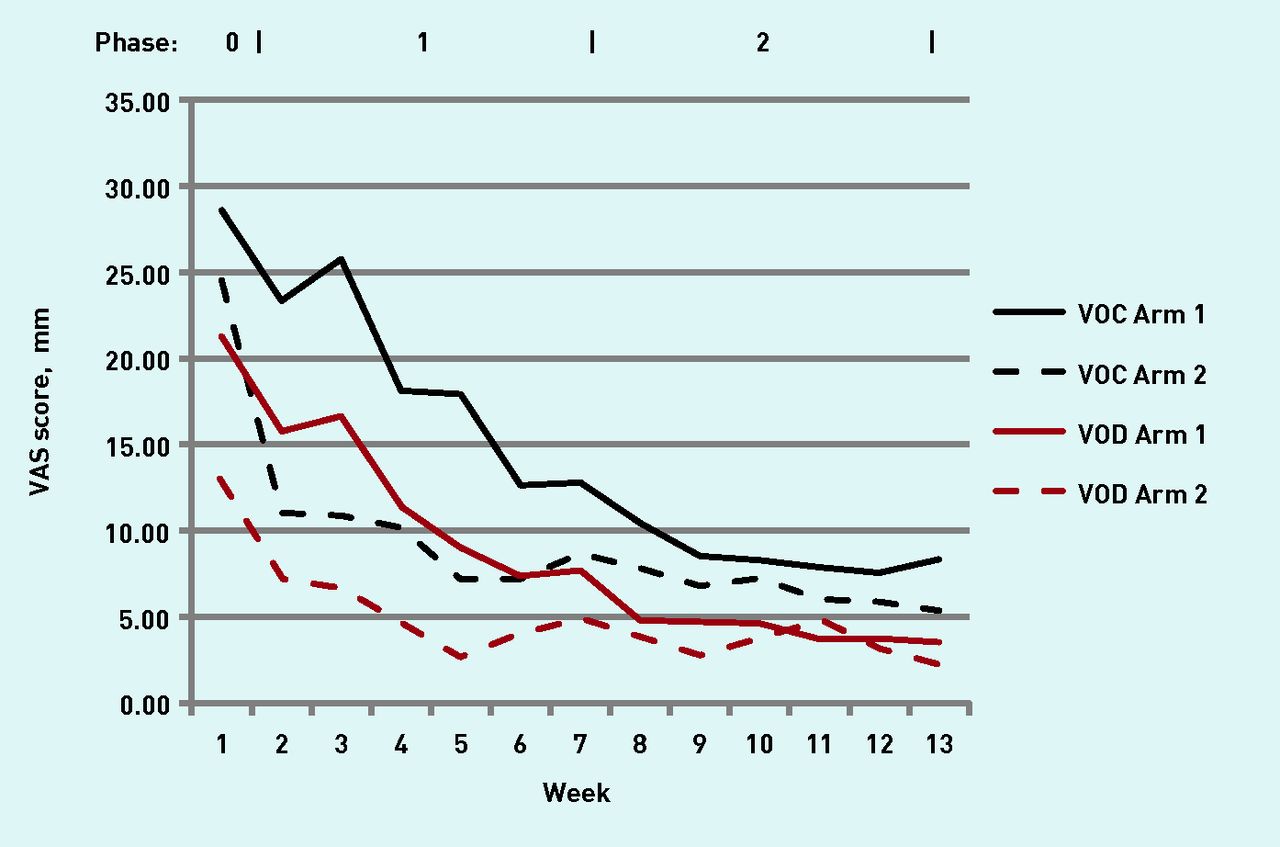
Figure 2 shows plotted scores of ‘complaint’ and ‘disability’ (mean VAS score per week) not corrected for temperature in each arm and phase.
{kind=link}
{kind=link}
Plotted scores on complaints (VOC) and disability (VOD) (not corrected for temperature) for each arm and phase. Arm 1 = betamethasone + placebo. Arm 2 = placebo + betamethasone. VAS = visual analogue scale. VOC = visual analogue scale on complaints. VOD = visual analogue scale on disability.
Primary outcome
Mean VOC at 6 weeks of treatment was 9.10 mm (95% CI = 5.31 to 12.88 mm) in the betamethasone cream group and 8.54 mm (95% CI = 4.75 to 12.33 mm) in the placebo cream group (Table 2). This resulted in a difference of 0.56 mm (95% CI = −2.88 to 3.99 mm) in favour of placebo (P = 0.744).
Results corrected for temperature differences on primary (VOC) and secondary (VOD) outcome
Secondary outcome
Mean VOD at 6 weeks of treatment was 5.07 mm (95% CI = 2.37 to 7.77 mm) in the betamethasone cream group and 4.19 mm (95% CI = 1.49 to 6.89 mm) in the placebo cream group (Table 2). This resulted in a difference of 0.88 mm (95% CI = −2.22 to 3.98 mm) in favour of placebo (P = 0.567).
Carry-over effect
Carry-over effect on the primary outcome
Mean VOC at 6 weeks of treatment was 10.31 mm (95% CI = 5.82 to 14.79 mm) in Arm 1 (betamethasone cream first) and 7.33 mm (95% CI = 2.28 to 12.38 mm) in Arm 2 (placebo cream first). This resulted in a difference of 2.98 mm (95% CI = −3.78 to 9.74 mm) in favour of Arm 2 (P = 0.376) (Table 2).
Carry-over effect on the secondary outcome
Mean VOD at 6 weeks of treatment was 5.57 mm (95% CI = 2.63 to 8.51 mm) in Arm 1 (betamethasone cream first) and 3.69 (95% CI = 0.38 to 7.00) in Arm 2 (placebo cream first). This resulted in a difference of 1.88 mm (95% CI = −2.56 to 6.31 mm) in favour of Arm 2 (P = 0.396) (Table 2).
Additional analyses
The authors found no statistically significant differences between topical betamethasone cream and placebo cream for assessed redness, purpleness, oedema, and ulceration after 6 weeks of treatment (Table 3).
Outcomes on additional analyses (6 weeks of treatment)
Adverse effects
No adverse effects (skin irritation or signs of skin atrophy) were found during betamethasone cream application or during placebo cream use.
DISCUSSION
Summary
There was no clinically or statistically significant difference between treatment with topical betamethasone valerate cream and placebo cream treatment. The authors also found no significant carry-over effect on either the primary or the secondary outcome. Adverse effects were absent.
Strengths and limitations
The main strength of this study was the effort to confirm the findings of the original study that generated weak evidence for the effectiveness of topical steroids in the treatment of chronic chilblains.11 No randomised trial on this topic had previously been performed. Nevertheless, topical steroids are widely prescribed by GPs. The authors used a randomised, placebo-controlled, crossover design and checked for a carry-over effect. The ambient temperature was taken into account as a major confounder.1,3,15,16
The calculated sample size was met. Participant compliance was good. Owing to the recruitment method used for participants in this study, it is possible to generalise the current findings for patients with idiopathic chronic chilblains as seen in primary care.
Chronic chilblains meet the criteria for the definition of a common disease.17 The condition does not endanger health but is annoying to the patient and causes restrictions in everyday life.2 The relatively rare effect studies on patients suffering from chronic chilblains show no consensus concerning outcome measurement. Due to the disease characteristics the authors chose to address the complaints reported by the participants. Primary and secondary outcome were assessed with VAS scores on pain, itch, and disability using a diary. VAS scores are generally used and validated for these purposes.18–20
The decision to test differences on VOC and VOD one-sided is based on a power issue. The aim of the study allows one-sided testing. The prevalence of chronic chilblains is low and inclusion is for obvious reasons limited to the winter months, necessitating the use of a design that requires a limited number of participants.
The authors did not ask participants to change their habits during the study, leaving the possibility of a Hawthorne effect.21 It is not possible to exclude such an effect caused by efforts of participants to diminish their symptoms by changing habits during the study. Nevertheless such an effect is considered to be unlikely because patients with chronic chilblains already try almost everything to relieve their symptoms.2
A remarkable reduction in complaints was found during placebo treatment. First, placebo effect may be responsible.22 Second, almost all studies on chilblains report that 60% to 70% of the patients show improvement on the different treatments.3 Third, the authors compared betamethasone cream with placebo cream and not to no treatment at all. It is possible that treatment with a cream not containing an active pharmaceutical agent is responsible for the reduction of complaints. In the authors’ opinion, however, the reduction of complaints during placebo use reflects a placebo effect as well as the natural course of the disease.
Almost one in four of the participants reported Raynaud’s phenomenon as a comorbidity. This figure may suggest some sort of relationship between chronic chilblains and Raynaud’s phenomenon. Participants suffering from Raynaud’s phenomenon were not excluded. This is because the condition is easy to distinguish from chronic chilblains: Raynaud’s phenomenon is characterised by sudden onset and short episodes with (in typical cases) biphasic discoloration of fingers and toes after exposure to low ambient temperatures, whereas in chronic chilblains prolonged inflammatory symptoms are characteristic.23–25
Comparison with existing literature
The current findings oppose the findings of the original study.11
Implications for practice
The effectiveness of betamethasone valerate 0.1% cream in the treatment of chronic chilblains in primary care is to be called into question. Topical steroids should not be used in the treatment of chronic chilblains without new evidence.
Acknowledgments
The authors thank Mrs CM (Rina) Siemons, research assistant.
Notes
Funding
This work is supported by the Netherlands Organisation for Health Research and Development Programme Common Diseases (grant number 42011006).
Ethical approval
The Dutch Competent Authority (NL 3069509109) and the Medical Research Ethics Committee CMO Arnhem-Nijmegen granted permission for this study (CMO dossier number: 2009/338).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 9, 2016.
- Revision requested September 5, 2016.
- Accepted September 14, 2016.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

