


Abstract
Background Current liver function testing for statin monitoring is largely unnecessary and costly. Statins do not cause liver disease. Both reduction in test frequency and use of a single alanine transaminase (ALT) rather than a full seven analyte liver function test (LFT) array would reduce cost and may benefit patients.
Aim To assess LFT testing in relation to statin use and evaluate an intervention to reduce full-array LFTs ordered by GPs for statin monitoring.
Design and setting Two-year cross-sectional time series in two east London clinical commissioning groups (CCGs) with 650 000 patients. One CCG received the intervention; the other did not.
Method The intervention comprised local guidance on LFTs for statin monitoring and access to a single ALT rather than full LFT array.
Results Of the total population, 17.6% were on statins, accounting for 43.2% of total LFTs. In the population without liver disease, liver function tests were 3.6 times higher for those on statins compared with those who were not. Following intervention there was a significant reduction in the full LFT array per 1000 people on statins, from 70.3 (95% confidence interval [CI] = 66.3 to 74.6) in the pre-intervention year, to 58.1 (95% CI = 55.5 to 60.7) in the post-intervention year (P<0.001). In the final month, March 2016, the rate was 53.2, a 24.3% reduction on the pre-intervention rate.
Conclusion This simple and generalisable intervention, enabling ordering of a single ALT combined with information recommending prudent rather than periodic testing, reduced full LFT testing by 24.3% in people on statins. This is likely to have patient benefit at reduced cost.
- diagnostic tests, statins
- liver function tests
- primary health care
- quality improvement
- unnecessary procedures
INTRODUCTION
There are two issues with liver function testing for statin monitoring: one is the frequency of liver function tests (LFTs) and the other is whether a full array of LFTs is routinely required. There have been long-standing concerns about possible statin hepatotoxicity.1 However, more than 30 years of statin use have confirmed that statins do not cause liver disease.2 Statins cause a usually transient elevation of liver transaminases. This is typically less than three times the upper limit of normal with around 2% of LFTs above that level.3–6 Statins are also likely to be beneficial in patients with non-alcoholic fatty liver disease in whom cardiovascular disease is the commonest cause of death, and statins are associated with reduced primary liver cancer.7,8 A UK health technology assessment confirmed alanine transaminase (ALT) as one of the two most useful analytes for routine identification of liver disease.9
Frequency of monitoring was addressed in 2006 in the US National Task Force, which recommended reduced liver function monitoring after starting a statin. A 2014 update by this Task Force confirmed that elevations in liver enzymes caused by statins were safe and did not cause liver disease.10
In 2012 the US Food and Drug Administration changed product requirements for statins to recommend a single LFT before starting statins and thereafter only if clinically indicated.10,11
In the UK, the Summary of Product Characteristics (SPC) for simvastatin 40 mg recommends testing before starting treatment and ‘thereafter when clinically indicated’. For simvastatin 80 mg, testing is recommended before titration and 3 months after, periodically for the first year.12 For atorvastatin, the SPC simply advises testing before starting and ‘periodically thereafter’.13 In 2014 National Institute for Health and Care Excellence (NICE) guidance advised the measurement of liver transaminase before starting a statin, at 3 months and 12 months, but not again unless clinically indicated. In other words, routine annual monitoring is not required by NICE and the US recommendation does not require routinely repeated testing.14
The second issue is the widespread use of a full array of up to seven different tests when clinicians request ‘LFTs’. It is usually impossible to choose a single liver transaminase test on the electronic laboratory request forms that are currently used. Uncertainty about periodic testing and the availability of only a full LFT array has led to widespread overtesting. Concern about raised transaminases has acted as one of the barriers to statin prescribing in the US and as a source of high cost and potential patient harm from overtesting.2,15,16
The two study clinical commissioning groups (CCGs) were served by the same hospital provider and, up until 2015, the full array of up to seven different analytes was the only option for LFT. In 2014 a local consensus panel including hepatologists, GPs, prescribing advisors, and laboratory staff developed guidance for Tower Hamlets CCG to make a single ALT available on the electronic ordering system and to promote the use of a single ALT test as sufficient to monitor statins. It recommended a single ALT before starting but not again unless clinically indicated.17,18 This presented an opportunity for a natural experiment comparing testing in the neighbouring Newham CCG, which used the same laboratory provider and GP electronic health record but which did not have either guidance or access to ALT testing. In east London the university-based Clinical Effectiveness Group has access to data extraction from these GP electronic health records.
How this fits in
Statins do not cause liver disease and current routine liver function monitoring is largely unnecessary and costly. A single alanine transaminase (ALT) test before statin initiation, rather than the traditional full array of up to seven different liver function tests (LFTs), is sufficient for routine testing, repeated once if the patient is on a high-intensity statin. Local guidance considered further testing unnecessary unless clinically indicated. Availability of a single ALT test reduced ordering of full-array LFTs by 24% in patients on statins.
The aim of this study was to estimate the extent to which liver function testing was associated with statin use rather than known liver disease, and to compare changes in the rate and type of LFTs in people taking statins in the intervention and control CCGs.
METHOD
The study conformed to the STROBE and RECORD guidance on reporting observational studies.19,20 Data were taken from GP electronic health records in 95 general practices serving a registered population of 650 000 patients in the inner east London CCGs of Tower Hamlets and Newham. All contributing practices used the same web-enabled record system (Egton Medical Information Services [EMIS]) with agreed data entry templates ensuring consistent data entry and coding. All requests for these LFTs were made by GPs and all results were obtained electronically. This study did not include liver function tests ordered by hospital clinicians. All long-term statin prescriptions were electronically prescribed by GPs. Anonymised data for the preceding month were extracted by the Clinical Effectiveness Group from the electronic GP record beginning April 2014, with repeated extractions monthly until April 2016 (24 months in total).
Anonymised data were obtained for all patients aged ≥30 years, currently registered at the start of each month. Variables included statin prescription within 6 months before the search date, practice, and CCG locality. The authors recorded all LFTs irrespective of underlying condition or medication in eligible patients, including multiple tests on the same patient. For these tests a value and date were extracted for ALT and serum bilirubin tests ordered in that month. A serum bilirubin test was used as a proxy indicator for LFT, which designates a full array of seven different tests. The authors assumed that, where the dates for ALT and serum bilirubin were equal, the value for ALT was recorded as part of a full LFT array, rather than as a single analyte. Serum bilirubin and ALT values below 0.01 were excluded as likely erroneous values. For the last quarter before the intervention ending March 2015, presence or absence of liver disease was collected as latest ever code of liver disease recorded. Counts of tests for both CCGs were combined for this quarter to investigate presence or absence of liver disease by statin prescription. The authors included all diagnostic codes for liver disease including chronic liver disease and cirrhosis, viral hepatitis, biliary tract, metabolic, enzyme and autoimmune disorders, liver disease in pregnancy, liver cancer, and thrombosis. A full code list is available from the authors on request.
In April 2015, the intervention in Tower Hamlets CCG consisted of enabling choice of a single ALT on electronic ordering systems. In addition, locally developed guidance on liver function testing was sent electronically with paper copies to all GPs and promoted at two educational meetings. The guidance is available online.18 Neither the guidance nor single ALT option were available in Newham. Tower Hamlets was the designated ‘intervention’ CCG and Newham the ‘control’ CCG. The guidance was amended in October 2015 to include a single repeat test for people on high-intensity statins to accord with the new NICE standards guidance.21
The intervention aimed to achieve a reduction in the primary outcome, the rate of full-array LFTs in people on statins in the intervention CCG compared with the control CCG. Reduction in total liver function testing in people on statins (both LFT and ALT) was a secondary outcome of interest.
Regression analysis was used to assess differences in monthly trends (change in slope and difference in intercept) for LFT rate per 1000 for the intervention CCG before and after the intervention. Differences in average testing in each CCG in the year before and the year after the intervention were assessed. All analyses were conducted using Stata (version 12.1). The P-values were two-sided with statistical significance set at 0.05.
RESULTS
Table 1 and Figure 1 show the number of LFTs and rate/1000 by statin and liver disease status for Newham and Tower Hamlets combined, for the 3 months ending March 2015, which was the final quarter before intervention.
Number of LFTsa and rate per 1000 population by statin and liver disease status for both CCGs combined, for the final quarter before interventionb
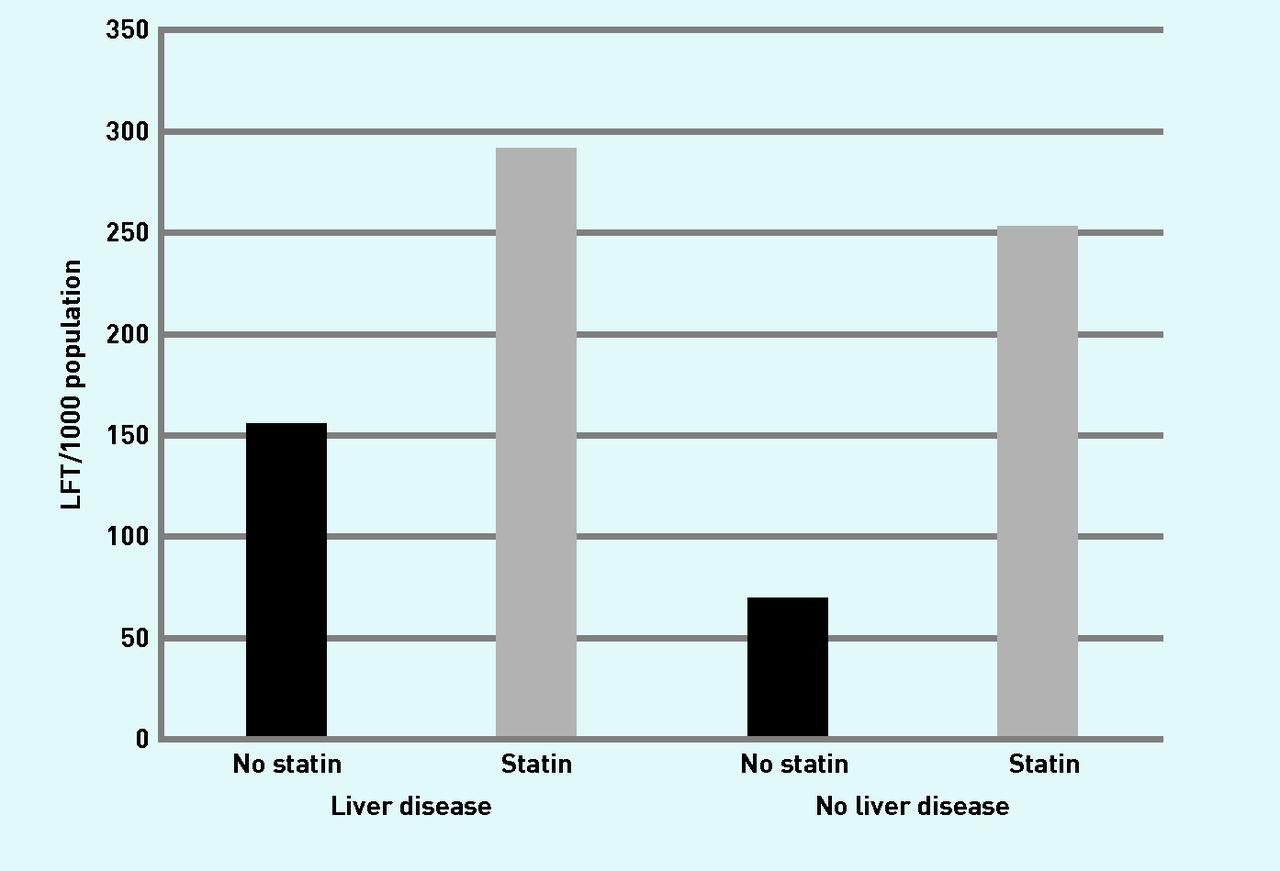
Number of full array LFTs and rate per 1000 population by statin and liver disease status for both CCGs combined, for the final quarter before intervention (ending March 2015).
CCG = clinical commissioning group. LFT = liver function tests.
In the total population, 17.6% (62 285/353 001) were on statins and they accounted for 43.2% (15 793/36 540) of total LFTs. Of these people on statins, 25.4% (15 793/62 285) had LFTs recorded in the quarter compared with 7.1% (20 747/290 716) of people not on statins. Liver disease was recorded in 2.5% (8961/353 001) of the population and LFTs in these people accounted for 5.1% (1847/36 540) of all LFTs. In those with liver disease 36.9% (3304/8961) were on statins and in those without liver disease 17.1% (58 981/344 040) were on statins. The rate of LFT/1000 for people with no liver disease was 3.6 (251.4/69.7) times higher for those on statins compared with those not on statins.
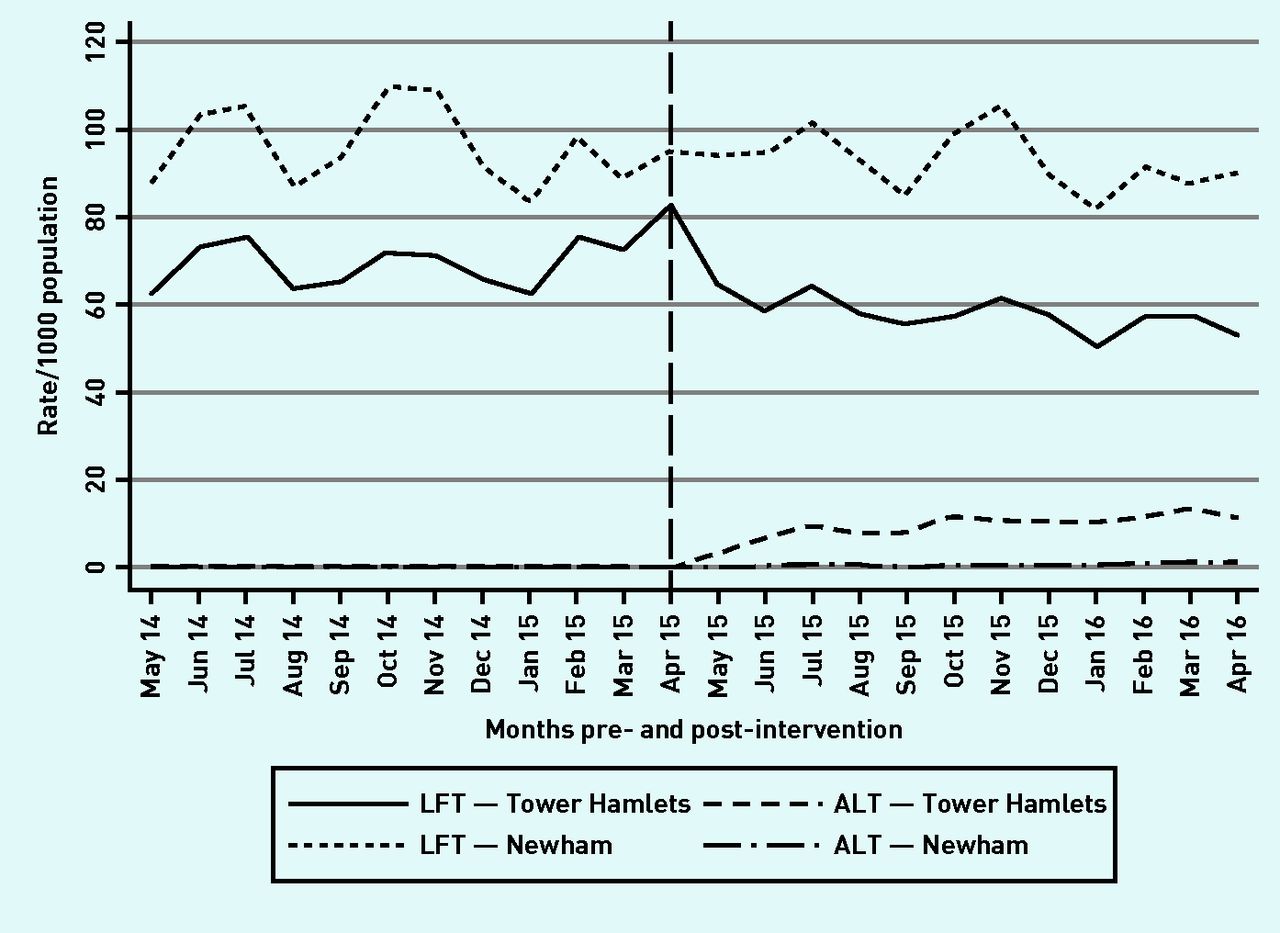
Table 2 shows the number and rate/1000 population of the full LFT array and single ALT test for people on statins by CCG by month. Figure 2 illustrates this graphically.
Number and rate per 1000 population of the full array of LFTs and single ALT test for people on statins, by month; pre- and post-intervention by CCG

Full array LFT/1000 and ALT/1000 by month for people on statins in Tower Hamlets and Newham CCGs. ALT = single alanine transaminase test. LFT = liver function test.
In Tower Hamlets, LFTs for people on statins decreased significantly from an average rate per 1000 of 70.3 (95% confidence interval [CI] = 66.3 to 74.6) in the pre-intervention year, to an average of 58.1 (95% CI = 55.5 to 60.7) in the post-intervention year (P<0.001). The rate per 1000 in the final month (March 2016) was 53.2, which represents a reduction of 24.3% on the average pre-intervention rate.
In Newham, there was no significant decrease in LFTs in people on statins from an average rate per 1000 of 96.3 (95% CI = 90.5 to 102.1) to 93.0 (95% CI = 88.6 to 97.3) post-intervention (P = 0.32). The rate per 1000 in the final month (March 2016) was 90.6, which represented a reduction of 5.9% on the average pre-intervention rate.
In Tower Hamlets, the rate of total liver function testing (LFT + ALT) rate per 1000 reduced from an annual average pre-intervention rate of 70.5 (21 736/308 479) to 65.3 (18 436/282 377) post-intervention, a reduction of 3.7% (2.6/70.4). In Newham total testing (LFT + ALT) rate per 1000 reduced from 96.7 (40 634/420 432) to 93.6 (40 933/437 506) post-intervention, a reduction of 3.2% (3.1/96.7).
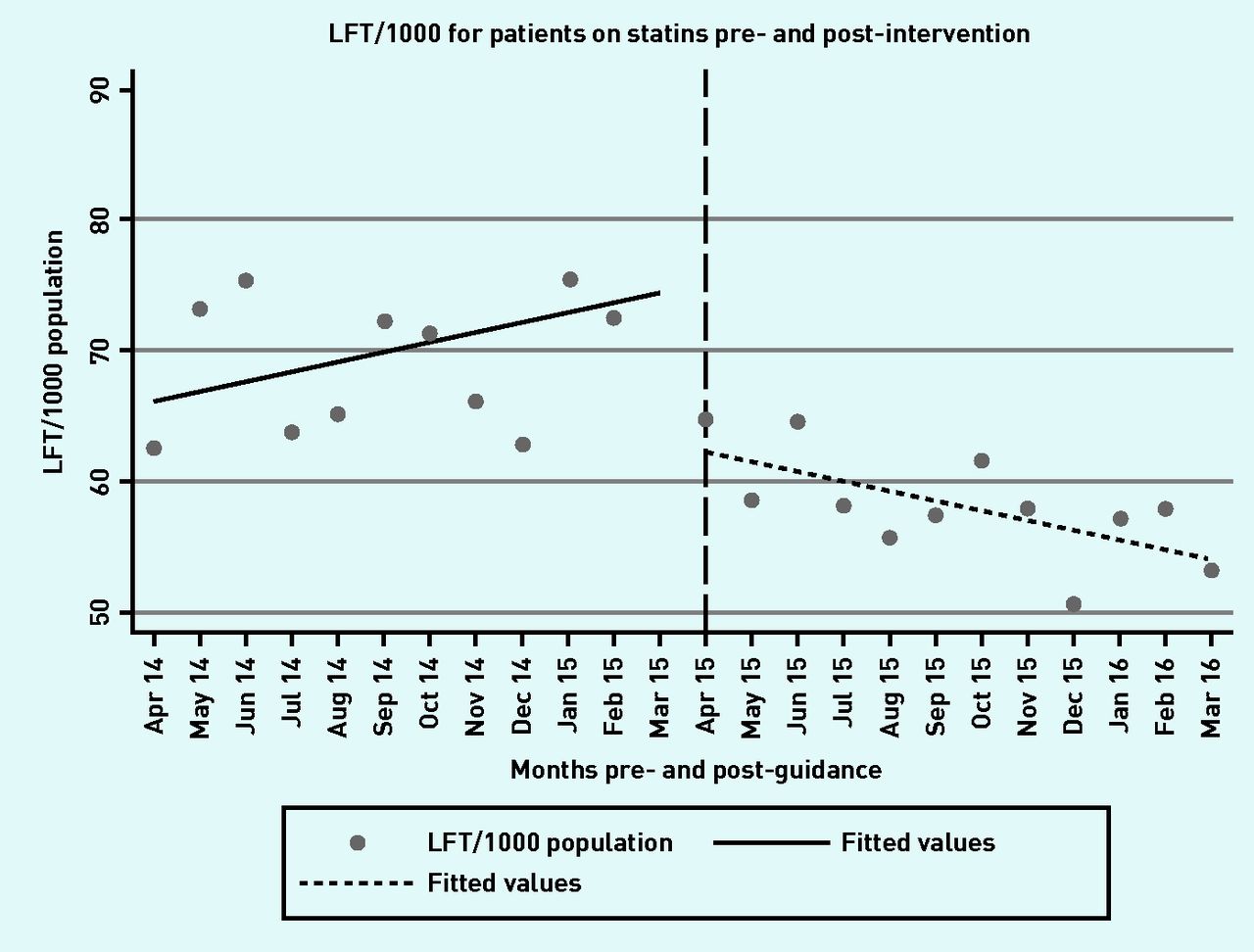
Figure 3 shows LFT/1000 by month for people on statins in Tower Hamlets pre- and post-intervention, and the fitted regression lines. Before the intervention there was a monthly increase of 0.76 in LFT/1000. After the intervention the rate decreased by 0.74 every month. The two slopes differed significantly (95% CI = −0.31 to −2.68; P = 0.016) and the test for difference between the slope intercepts confirmed a significant reduction in LFT rate per 1000 post-intervention of 13.1 (95% CI = −4.88 to −21.32; P = 0.003).

{kind=link}
{kind=link}
{kind=link}
Full array LFT per 1000 patients by month in Tower Hamlets CCG, showing pre- and post-intervention fitted values. LFT = liver function test.
In the study CCGs a full LFT was priced at £45.50 and a single ALT at £6.50. In Tower Hamlets there were 3300 fewer full LFTs in the post-intervention than the pre-intervention year, which represents a saving on the cost of testing alone of £150 150. Subtracting the additional 3033 single ALT tests costing £19 715 represents an overall decreased cost of £130 435. In Newham CCG there was an increase of 185 full LFTs and 114 single ALTs at a total increased cost of £9158.
DISCUSSION
Summary
This study is the first to evaluate the impact of statin use on liver function testing in routine UK practice. The authors describe the changes that occurred in one CCG when new local guidance on liver function testing and a single ALT test were made accessible to GPs. Although people on statins represented 17.6% of the total population, they accounted for almost half, 43.2%, of total LFTs undertaken.
By the end of the post-intervention year in Tower Hamlets there was a 24.3% reduction in the full LFT array in people on statins in comparison with the year preceding the intervention. There was no significant decrease in Newham, the control CCG, and, as a result of increased ALT tests, no significant reduction in overall testing.
Strengths and limitations
The data were collected from all 95 practices across the two CCGs and electronic recording of both prescribing and investigations ensured almost complete recording of data. The results are an accurate reflection of changes in liver function testing by GPs in an entire local area, not just selected practices. However, this study did not include LFTs undertaken by hospital clinicians and the results may underestimate the potential gains. The CCGs studied are not representative of the UK, as they serve exceptionally disadvantaged and ethnically diverse populations with high levels of cardiovascular disease, diabetes, and statin use.22 However, the problem of unnecessary testing is relevant to all areas in the UK.
The authors were not able to directly ascribe all liver function testing in people on statins to the use of statins as testing occurs for other reasons including repeat testing due to abnormal test results. However, the 3.6-fold increase in testing in people on statins without liver disease represents substantial additional testing associated with statin use, and demonstrates that statin use rather than pre-existing liver disease is responsible for a high proportion of all liver function testing. The authors did not analyse repeat testing or abnormal results.
Small numbers of single ALT tests, 165 in Newham and 39 in Tower Hamlets before the intervention, increased slightly to 239 in Newham after the intervention. These are ‘orphan’ results erroneously separated from the full analyte array. In relation to around 60 000 full LFT arrays annually these make no material difference to the results. The apparent increase in ALT use in Newham post-intervention is likely due to patient transfer from Tower Hamlets to neighbouring Newham.
There were baseline differences in LFT testing between CCGs with pre-intervention levels in people on statins of 96/1000 in Newham and 70/1000 in Tower Hamlets. The reasons for this are unclear but the differences may be because of long-standing scepticism about the value of routine monitoring among some Tower Hamlets GPs.
Comparison with existing literature
Liver function testing for statin use is recognised as a substantial contributor to treatment costs in the UK.23 In Finland, an analysis of cost-effectiveness of statins for primary prevention gave monitoring costs for patients taking statins for primary prevention as €147.90 (£108.59) per annum, based on one additional doctor consultation, nurse consultation, and blood test per year.24 Lilford et al have reviewed liver function testing in the wider context of liver disease and also highlighted the cost implications of a reduced analyte panel.9,25
Implications for practice
Prices for laboratory testing vary substantially. The price of the full LFT analyte panel was £45.50 in Tower Hamlets and Newham CCGs. In Tower Hamlets approximately 20 000 LFTs were performed by GPs each year for statin monitoring at a cost per annum of £910 000. The intervention reduced the cost of LFTs by £130 435 and in the control CCG it increased by £9158. Additional savings are likely as practices make more use of the ALT-only option.
A more formal analysis of the full economic costs of reduced testing nationally would be a worthwhile topic for review. However, the magnitude of these costs can be approximately estimated, assuming an illustrative cost per full LFT array of £10, with 20 000 tests in people on statins per CCG in each of the 209 CCGs in England costing £42 million per annum; a reduction of 20% in testing would save £8.4 million per year, offset by increases in ALT testing. These estimates take no account of the costs of consultation time related to testing, phlebotomy, or sensitivity to pricing.
For patients, fewer blood tests will result in fewer false positive results, unnecessary testing, and patient anxiety. For providers it decreases laboratory costs, phlebotomy, and clinical staff time.16,26 Almost 20 years ago, simple changes in test ordering were shown to have a dramatic impact on use.27 Enhanced feedback (publication of test requests per practice) and reminder messages may further improve the results. These each achieved a 10% reduction in laboratory test ordering in a study of 85 GP practices in northeast Scotland.28 There is much to suggest that substantial overuse of a range of other common laboratory tests by both GPs and hospital clinicians might be similarly ameliorable.29 This simple intervention, enabling ordering of a single ALT combined with information recommending prudent rather than routine annual testing, could have substantial patient benefit at reduced cost.
Availability of an option to order a single ALT combined with guidance on prudent testing in people on statins reduced full-array LFT testing in the post-intervention year by 24% in people on statins. There was no significant change in testing in the control CCG.
Acknowledgments
The GPs and their staff were responsible for entering the data on study subjects and the staff of the Clinical Effectiveness Group supported this process by providing standard data entry templates and support for web-based data extraction. The entire enterprise is contingent on local GPs who are able and willing to share their anonymised data for research and development purposes, and the local laboratory staff and hospital who were willing to change their test ordering procedures.
Notes
Funding
This research received no specific funding. The salaries of the principal investigator and other authors who contributed to this study were funded by Newham, City and Hackney, and Tower Hamlets CCGs.
Ethical approval
All data were anonymised and managed according to the UK NHS information governance requirements. Ethical approval was not required for the use of anonymised data in this observational study.
Provenance
Fully submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received July 14, 2016.
- Revision requested August 12, 2016.
- Accepted September 25, 2016.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

