


Abstract
Background There is currently no specific guidance on the role of exercise in managing postpartum depression in the UK and US, and international guidance is inconsistent.
Aim To assess the effectiveness of aerobic exercise on postpartum depressive symptoms.
Design and setting Systematic review and meta-analysis. There was no restriction to study site or setting.
Method The databases MEDLINE, EMBASE, Cochrane Library, PsycINFO, SportDiscus, ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform were searched. Titles and abstracts, then full-text articles, were screened against inclusion criteria: RCTs measuring depressive symptoms in mothers ≤1 year postpartum; and interventions designed to increase aerobic exercise compared with usual care or other comparators. Included studies were assessed using the Cochrane Collaboration’s risk of bias tool. Meta-analysis was conducted. Pre-planned subgroup analyses explored heterogeneity.
Results Thirteen RCTs were included, with 1734 eligible participants. Exercise significantly reduced depressive symptoms when all trials were combined (standardised mean difference −0.44; 95% confidence interval = −0.75 to −0.12). Exploration of heterogeneity did not find significant differences in effect size between women with possible depression and in general postpartum populations; exercise only and exercise with co-interventions; and group exercise and exercise counselling.
Conclusion This systematic review provides support for the effectiveness of exercise in reducing postpartum depressive symptoms. Group exercise, participant-chosen exercise, and exercise with co-interventions all may be effective interventions. These results should be interpreted with caution because of substantial heterogeneity and risk of bias.
INTRODUCTION
Postpartum depression is a global mental health issue, annually affecting 13 million women worldwide.1–3 Postpartum depression can lead to thoughts of self-harm and/or harm of the child,4 and negatively affect children’s development.5,6 There can be reluctance by women to take antidepressants postnatally, particularly if they are breastfeeding.7,8 Cognitive behavioural therapy can be effective but waiting lists are often long in the UK.9 Exercise can have a moderate effect in reducing general adult depression (standardised mean difference [SMD] ]−0.62, 95% confidence interval [CI] = −0.81 to −0.42).10
Practitioner-led group exercise is recommended by the UK National Institute for Health and Care Excellence (NICE) for persistent subthreshold depressive symptoms and mild-to-moderate depression.11 However, women in the postpartum period have particular physical, practical, and psychological challenges to exercising.12,13
A 2009 review provided some support for exercise as an adjunctive treatment for postpartum depressive symptoms.14 Despite its challenges, exercise provides another intervention option when many mothers are reluctant to seek treatment and/or take antidepressants.8
Exercise also offers improved fitness and weight loss, and opportunities for social interaction at a time when women experience decreased exercise and weight retention.15–17
Aim and objectives
The aim and objectives of this study were to undertake a meta-analysis of randomised controlled trials (RCTs) investigating the effect of aerobic exercise interventions, compared with usual care, on depressive symptoms in women up to 1 year postpartum. The study aimed to explore the effect of exercise on depressive symptoms in three subgroup analyses:
women with possible depression and general postpartum populations;
interventions based only on exercise and those with co-interventions; and
interventions providing structured group exercise and those supporting participant choice of exercise.
METHOD
The review was registered on PROSPERO: CRD42016047656.
Data sources and searches
The Cochrane Collaboration’s guidance was followed on reviews of interventions18 and PRISMA guidelines.19 The following bibliographic databases were searched electronically for eligible trials: MEDLINE, EMBASE, the Cochrane Library, PsycINFO, SportDiscus, and ClinicalTrials.gov. The World Health Organization (WHO) International Clinical Trials Registry Platform was searched for trials in progress. Searches were conducted for grey literature in Open Grey (http://opengrey.eu/) and OAIster Worldcat (http://oaister.worldcat.org/).
How this fits in
UK clinical guidance recommends psychological therapy and antidepressants for postnatal depression. However, women can be reluctant to take antidepressants postnatally and the availability of psychological therapies is often limited. Exercise is effective in treating depression in the general adult population; however, there are particular challenges to be overcome in the postnatal period. This systematic review found that exercise is an effective intervention for reducing postnatal depressive symptoms.
Searches were conducted on a range of psychological outcomes; only the results for depression are presented. The following terms were searched as text words and MeSH terms where applicable: exercise, physical activity, postpartum, postnatal, mother, birth, perinatal, depression, anxiety, self-efficacy, quality of life, mother and infant bonding, and child development (the MEDLINE search strategy is available from authors on request). Searches were unrestricted by date or language and undertaken up to September 2016. Bibliographies of eligible studies and reviews were searched for additional trials, and authors contacted if required. Two researchers independently reviewed titles, abstracts, and full-text articles. Eligibility discrepancies were discussed with a third reviewer.
Study selection
Inclusion criteria were:
populations of mothers <1 year postpartum;
interventions designed to increase aerobic exercise (activity causing increased heart rate, respiratory rate, and sweating), including those with co-interventions such as social support or nutrition elements;
comparator groups receiving no care or any form of usual care;
depressive symptoms measured by questionnaire or diagnostic interview; and
RCTs.
Exclusion criteria were trials comparing two types of exercise.
Data extraction and quality assessment
Data describing the population, intervention, and findings were extracted independently by two researchers using standardised, piloted, extraction spreadsheets. Reviewers were not blinded to authors, institution, or journal. Authors were contacted if clarification was required.
Two researchers independently applied the Cochrane Collaboration’s risk of bias tool18 in relation to sequence generation, allocation concealment, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias.18 Blinding of personnel and participants to group allocation was not assessed because of the impracticalities of this in exercise trials. Each study was allocated an overall risk of bias: with a low risk of bias being assigned if the risk of bias was deemed to be low in all subdomains; an unclear risk of bias if the risk was considered unclear in one or more subdomains; and a high risk of bias if the risk was considered high in one or more subdomains.18 Publication bias was assessed by visually inspecting a funnel plot of the SMDs for depressive symptoms.
Data synthesis and analysis
Populations indicating possible depression on screening questionnaires or in the clinical judgement of a health professional are referred to as ‘depressed’ postpartum populations.
Meta-analyses and meta-regressions were conducted using Review Manager 5.3. An SMD18 was calculated for continuous outcomes of depressive symptoms. If more than one measure for depression was reported, the primary continuous outcome measure was used. The final point of follow-up was used because the aim was to report long-term outcomes. A weighted mean difference (WMD) was calculated for all trials using the Edinburgh Postnatal Depression Scale (EPDS) to assess depressive symptoms.20 Where the standard deviation of the difference in score was not reported, this was calculated. A correlation of 0.6 was used in the assumptions to estimate standard deviations of differences, based on a previous sample of postpartum women.21 A random effects model was used throughout because of known clinical heterogeneity between populations and methodological heterogeneity between interventions.
An initial pooled SMD difference was calculated with 95% CI, with all trials included. Statistical significance was defined as having a 95% CI that did not include zero. Clinical heterogeneity was explored (by qualitatively comparing characteristics between trials) and statistical heterogeneity using χ2 tests of heterogeneity and the I2 statistic.
Three a priori subgroup analyses were performed, investigating whether the effectiveness of exercise in reducing postpartum depressive symptoms varied in relation to the population of women (women with possible depression or general postpartum populations); the presence of co-interventions (exercise only or exercise with co-interventions such as diet or social support); and the context of exercise (exercise groups or participant choice; participant choice often consisted of exercise counselling interventions in which participants typically elected to exercise alone, often by walking). For each hypothesis, the trials were categorised into subgroups; and a random effects meta-regression model was used to determine the effects of exercise in each subgroup and the significance of differences between subgroups.
RESULTS
Trial selection
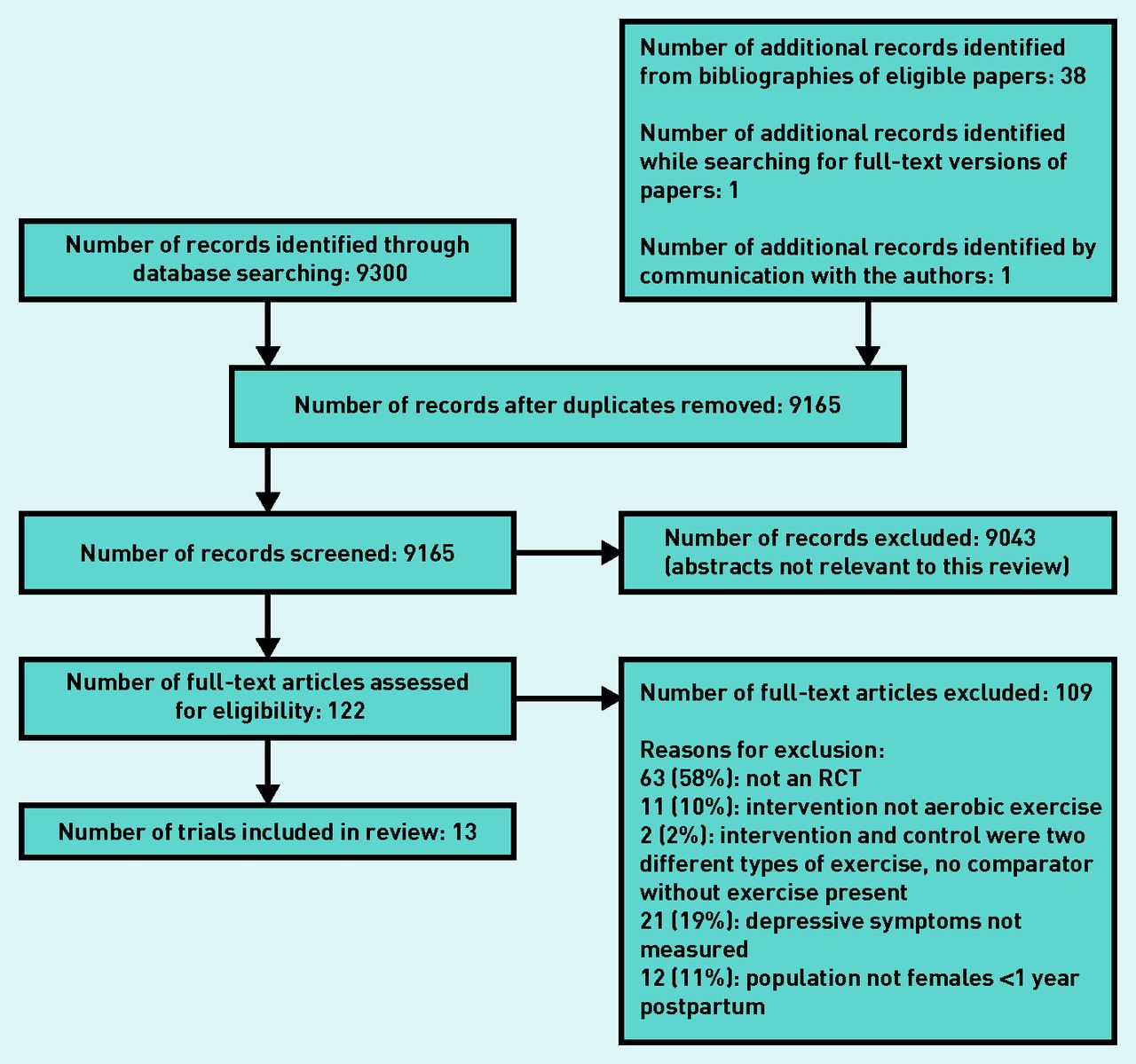
Of the 9165 records identified after the removal of duplicates, 9043 were excluded after reading titles and abstracts. A further 109 full-text records were excluded based on the eligibility criteria. Thirteen trials were included in the meta-analysis (Figure 1).

PRISMA flow chart. The 40 records in the top right-hand box are additional papers found.
Trial characteristics
All 13 RCTs had been peer reviewed and published as journal articles,22–24,26–33 a PhD thesis,25 or abstracts.34 Four trials were conducted in the US,25,27,29,31 three in England, UK,28,33,34 two in Australia,22,26 one in Canada,23 one in India,30 one in Japan,32 and one in Taiwan.24
The total population of the combined studies was 1734 eligible participants, with follow-up data provided by 1307 participants who were included in the primary meta-analysis. Seven trials recruited participants with possible depression,22–25,28,33,34 of which three required participants to score above a threshold on the EPDS questionnaire (from ≥10 to >12),26,27,32 and two required a diagnosis of depression (International Classification of Diseases version 10 [ICD-10]33 or Diagnostic and Statistical Manual of Mental Disorders fourth edition [DSM-IV] criteria).34 Despite not reporting baseline depression threshold criteria, two trials reported mean baseline depression scores indicating depressed populations (EPDS scores of 18.9–19.8,25 Beck Depression Inventory [BDI] 15.8–16.9).27 These trials were therefore considered to have ‘depressed’ postpartum populations. Six trials recruited general postpartum populations (Table 1).26,27,29–32
Trial characteristics
Intervention characteristics
All trials included interventions designed to increase exercise levels. In addition, two trial interventions also aimed to improve diet and encourage a healthy lifestyle,24,27 two also provided social support,22,31 and one also provided education on postpartum issues.26 Six trials had group exercise interventions;22,26,30–32,34 seven trials had interventions in which exercise counselling was provided and the participant was free to choose their own form of exercise (Table 1).23–25,27–29,33 The interventions ranged from 4 weeks’ duration30,32 to 6 months.24,29,33 Most aimed to achieve 30 minutes of moderate activity three to five times weekly,22,23,25,27–29,32–34 although some consisted of once-weekly group exercise.26,30 Eight of the studies reported adherence to the intended intervention.22,23,25,28,29,32–34
Risk of bias in included studies and publication bias
Six trials were considered at unclear risk22,23,28–30,34 and seven at high risk of bias.24–27,31–33 Principal factors introducing a risk of bias were a lack of intention-to-treat analyses (some studies excluded non-adherent participants), a lack of clarity on selective outcome reporting, a lack of robust sequence generation and concealment of randomisation procedures, and unclear blinding of those conducting outcome assessments and analyses (details of the risk of bias in included studies are available from the authors on request).
The funnel plot was visually inspected for the main analysis including all trials. There appeared to be a lack of smaller studies with results indicating an increase in depression in exercise intervention groups compared with comparator groups. This may be an indication of publication bias (details available from the authors on request).
Provision of additional data
Authors of four trials provided additional data for this review: DaCosta et al,23 Surkan et al,27 Lewis et al,29 and Boath et al.34
Data analysis
Overall effect of exercise on depression scores
Exercise interventions significantly reduced depressive symptoms (SMD −0.44, 95% CI = −0.75 to −0.12, n = 1307, I2 85%, 13 trials) (Figure 2).22–34 The WMD was −1.54 EPDS units, 95% CI = −2.97 to −0.12, n = 652, I2 87%.22,23,25,26,28,30–34

{kind=link}
{kind=link}
Meta-analysis of the effect of exercise on depressive symptoms (standardised mean difference). CI = confidence interval. SD = standard deviation.
Population
Exercise interventions had a significant effect in reducing depressive symptoms in ‘depressed’ postpartum populations (SMD −0.32, 95% CI = −0.63 to −0.00), I2 55% (Table 2),22–25,28,33,34 and in general postpartum populations (−0.57, 95% CI = −1.12 to −0.02, I2 92%) (Table 2).26,27,29–32 The effect of exercise interventions in the ‘depressed’ and general postpartum populations was not significantly different (test for subgroup differences χ2 0.62, P = 0.43, I2 0%) (further details available from the authors on request).
Subgroup analyses: population, intervention type, and exercise context
Intervention type
Exercise-only interventions had a non-significant effect in reducing depressive symptoms (SMD −0.56, 95% CI = −1.13 to 0.01, I2 89%).23,25,28–30,32–34 Exercise with co-interventions had a significant effect on reducing depressive symptoms (−0.35, 95% CI = −0.66 to −0.04, I2 72%).22,24,26,27,31 The effect of exercise-only interventions and exercise co-interventions on depressive symptoms was not significantly different (test for subgroup differences: χ2 0.41, P = 0.52, I2 0%) (Table 2) (further details available from the authors on request).
Exercise context
Group exercise interventions had a significant effect in reducing depressive symptoms (SMD difference −1.10, 95% CI = −1.99 to −0.21, I2 93%).22,26,30–32,34 Participant choice interventions such as exercise counselling with personal choice of exercise (often exercise alone) had a significant effect in reducing depressive symptoms (−0.20, 95% CI = −0.33 to −0.06, I2 0%).23–25,27–29,33 The effects of group exercise and participant choice exercise on depressive symptoms were not significantly different (test for subgroup differences: χ2 3.89, P = 0.05), I2 74%) (Table 2) (further details available from the authors on request).
DISCUSSION
Summary
There is no specific guidance on the role of exercise in management of perinatal mental health in the UK or the US.7,35 This systematic review provides support for exercise as an effective treatment for reducing postpartum depressive symptoms, whether or not women meet robust criteria for postpartum depression. Additionally, characteristics of exercise interventions have been explored that are most likely to be effective for the postpartum population.
Strengths and limitations
Caution should be taken when interpreting the present results, as a substantial level of heterogeneity was present. Heterogeneity was present in the design of the trials, including exercise-only interventions and those also promoting a healthy diet or social support among peers. Exercise contexts also varied between structured, group-based exercise and tailored exercise counselling with participant choice of exercise. A random effects model was used in analyses to account for this variation, and potential causes of heterogeneity were explored in subgroup analyses; however, there were insufficient numbers of trials to explore this heterogeneity in depth. The last follow-up point was used because the focus of the present study was on long-term outcomes; the median duration of follow-up was 6 months from recruitment (IQR 3.6 months).
The methodological quality of several of the included trials was low. Exclusion of non-adherent participants, insufficiently robust sequence generation, and unclear blinding of outcome assessors resulted in an increased risk of bias. Only two included trials in ‘depressed’ populations recruited women with a diagnosis of depression (ICD-10 or DSM-IV);33,34 the remainder used screening questionnaires such as the EPDS 20 to indicate women with possible depression. The EPDS has the advantage of being relatively short and simple to complete, but has been reported to have considerable heterogeneity in sensitivity and specificity for detecting postpartum depression across different settings and populations.36
There was a lack of assessment of exercise duration and intensity in included studies; of those that did provide this information, only two included an objective measure of exercise.31,33 Exercise intensity can be difficult to determine accurately by self-report. For future research, objective accelerometry would allow for greater accuracy and more meaningful comparison between intervention types.
This review has several strengths. Recommended methods were followed; searching was systematic and not limited by language of publication. The review was restricted to RCTs to reduce the potential for confounding. The effectiveness of exercise was explored in different populations, intervention types, and exercise contexts, which has not been previously attempted.
Comparison with existing literature
The evidence in this field has increased substantially since the review by Daley et al in 2009.14 Although the primary effect size in this review is smaller than that reported by Daley et al (SMD −0.44, 95% CI = −0.75 to −0.12 rather than −0.81, 95% CI = −1.53 to −0.1014), the CI surrounding the effect is narrower here, indicating more precision.
In this review, the effect of exercise in depressed postpartum populations was smaller than that reported in a recent review of exercise in general adult depressed populations (SMD −0.62, 95% CI = −0.81 to −0.42),10 indicating that there may be differences in the way general adult populations and postpartum populations respond to exercise or differing abilities to adhere to an exercise regime. Women in the postnatal period have the time constraints of new parenthood and barriers to exercise such as fatigue. These factors could be explored by qualitative research with postnatal women.
The effect of exercise on postpartum depressive symptoms reported in this review compared favourably with that reported in a review of low-intensity psychological interventions (such as online cognitive behavioural therapy and self-help literature) versus usual care for depression in the general population (SMD −0.42, 95% CI = −0.55 to −0.29).37 Despite some temporary changes in the composition of breastmilk following maximal exercise, the literature does not suggest any detrimental effects of moderate levels of aerobic exercise,38 as evaluated by the trials in this review. Such interventions are often among the first treatments offered to individuals presenting with depression.11 The effect reported here of exercise on postpartum depressive symptoms is also comparable with those reported for antidepressants in depressed adult populations (SMD −0.49, 95% CI = −0.67 to −0.32 for tricyclic antidepressants and −0.24, 95% CI = −0.35 to −0.12 for selective serotonin reuptake inhibitors compared with placebo).39
Exercise interventions also offer the additional health benefits of improved physical fitness and weight loss, outcomes particularly relevant to postpartum women, who often experience decreased exercise levels and excess weight.15–17 The finding that both group exercise and participant choice of exercise (often solitary exercise) may be effective in reducing postpartum depressive symptoms is also noteworthy. Current guidance from NICE on the treatment of postpartum mental illness refers clinicians to exercise advice for the general adult population, recommending only group exercise,11 which may not be the most feasible or acceptable option for women after having a baby.40
Implications for practice
National and international guidance on the use of exercise to reduce depressive symptoms in the postpartum period is lacking. Although acknowledging considerable uncertainty about the present findings because of substantial heterogeneity, given the high prevalence of postpartum depression and the potential for exercise to be a low-cost, freely available intervention, aerobic exercise should be considered as a management option for postpartum women with depressive symptoms and as a potential preventative measure more generally in postpartum women.
Notes
Funding
This study presents independent research funded by the University of Birmingham, the National Institute for Health Research (NIHR) School for Primary Care Research, and the Collaboration for Leadership in Applied Health Research and Care West Midlands. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
All authors declare no support from any organisation for the submitted work; there are no financial relationships with any organisations that might have an interest in the submitted work. Ruth Victoria Pritchett (née Blamey) reports that she is an author of one of the trials in this review, Amanda J Daley reports that she is an author of two of the trials included in this review, and Kate Jolly reports that she is an author of one of the trials included in this review.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received January 19, 2017.
- Revision requested March 27, 2017.
- Accepted April 5, 2017.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

