


Self-harm is increasingly common in adolescence, with reported prevalence rates in the UK varying from 68%1 to 10%.2 Though frequently low risk and transient, in some young people the behaviour can persist into adulthood and/or become life threatening. Although GPs regard the identification and support of young people who self-harm as part of their role,3 there are particular challenges with this as self-harm is one of the most complex mental health issues with which young people present. These challenges broadly relate to understanding young people’s self-harm and talking about it with them in short, time-limited consultations. Additional dilemmas surround recording self-harm and how to intervene in ways that help.
UNDERSTANDING YOUNG PEOPLE’S SELF-HARM
Self-harm encompasses behaviours that young people do to hurt themselves, such as self-cutting, self-burning, and ingesting toxic substances or objects.
Young people who present with self-harm to primary care are a heterogeneous population, which includes a minority who are intent on ending their own life4 but who are not easily distinguishable in their help-seeking behaviour from the majority whose self-harm is reported as an attempt at self-help, a coping strategy ‘that they wished they did not need and might someday be able to quit’.5
The relationship between stressful life events and common mental health problems such as depression and anxiety for those of any age is well documented, and for young people such stressful life events need to be understood in the context of the inevitable developmental milestones of growing up. Young people often report that their self-harm helps them to cope with overwhelming distress associated with bullying, and with peer pressures experienced directly and/or through social media. Triggers for self-harm can include exam pressures, attempting to cope with difficult family relationships characterised by separation and/or loss, caring for loved ones with physical and/or mental health issues, and in worst cases relationships characterised by abuse and trauma. As young people mature, many will find different ways of dealing with their emotional and psychological distress, and their self-harm will become less frequent as a consequence.
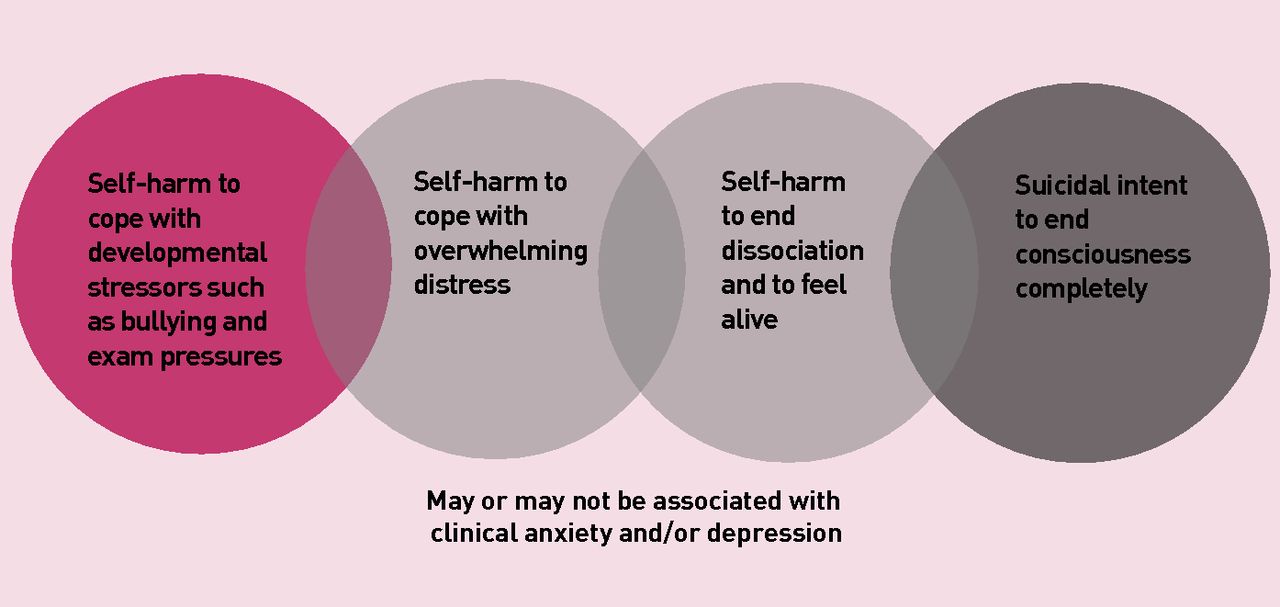
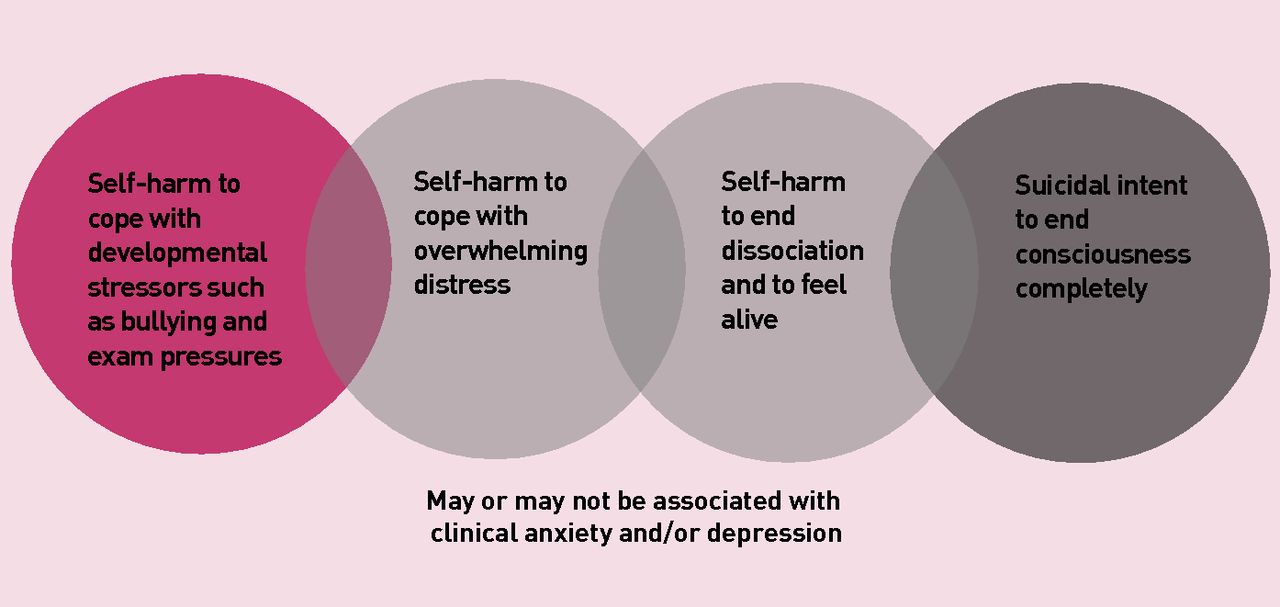
GPs interviewed in one study perceived self-harm as a ‘spectrum of risk for suicide’ 3 and in our research we suggest a continuum of self-harm behaviours (Figure 1) including: self-harm as a response to coping with psychosocial stressors associated with developmental milestones, self-harm with co-occurring clinical symptoms (anxiety and depression are the most common), and self-harm that signals a young person’s intent to end consciousness completely.6 Adopting a more nuanced understanding can help GPs who report not knowing how to respond to young people’s self-harm2 and in turn inform decisions about signposting and treatment.
{kind=link}
Continuum of self-harm behaviours in young people.
TALKING ABOUT SELF-HARM
Talking about self-harm presents a challenge for the young person and the primary care clinician for different reasons. Of those young people who do self-harm only 12% will seek professional help and rarely will young people presenting to primary care identify their self-harm as the reason they are attending. This may be because the young person has poor interpersonal and communication skills, or has concerns about whether shared information will be kept confidential and/or the negative consequences of disclosure.7 Young people sometimes struggle to explain their self-harm behaviours and fear not being taken seriously or not being treated respectfully because of their age when they ask for help.6
A challenge for the primary care clinician is how get to the multifaceted nature of young people’s distress within short, 10-minute appointments.8 GPs regard screening tools as too formal for time-limited consultations,3 yet clinicians need to assess the risks of self-harm engaged in by the young person by asking questions in a way that does not exacerbate risk or cause the young person even greater distress. This is a skill that requires confidence and may mean raising the issue of self-harm during an unrelated consultation, for example, when a young person attends for an immunisation or blood test. Whether or not a young person discloses their self-harm, National Institute for Health and Care Excellence (NICE) guidelines advocate an important role for primary care in its assessment and treatment.9 GPs as a first point of contact, in a non-stigmatised health setting, provide an opportunity for supportive consultations.
Alongside clinical literature on self-harm exists a parallel body of literature about self-help for self-harm with contributions from those who have engaged in the behaviour, including some from young people. Taken together, these literature sources offer some consensus about how to have initial helpful conversations with young people about their self-harm. Young people feeling listened to is revealed as a key theme, as is a recognition of self-harm as an expression of personal distress. Giving the opportunity to young people to talk about their self-harm in their own words is also experienced as helpful. Guided self-help information is best worked through with professionals rather than being given to the young person to read after a consultation.
Conducting helpful conversations, within a short, 10-minute consultation, remains a significant challenge for primary care. However, young people and clinicians in our research in this area identified that the doubling up of appointments and telephone consultations worked well.6 Young people generally understand that GPs and practice nurses are busy health professionals and accept that consultations will be short. Making ‘time’ for the young person presenting with self-harm can therefore be communicated in other ways, in particular by involving the young person in treatment options and referral decisions.3,6
RECORDING SELF-HARM
One reason why studies are inconclusive about primary care interventions that work for young people’s self-harm is because sampling of young people engaging in the behaviour is beset with issues of inconsistent recording. Often the type of self-harm young people engage in and their reasons given for doing so is missing in their patient record.6 Recording behaviour as deliberate self-harm (DSH) is discouraged by the Royal College of Psychiatrists in 2014 (http://www.rcpsych.ac.uk/healthadvice/problemsdisorders/self-harm.aspx) because of its connotations of blame and associated stigma. Often because of how information gets added to young people’s medical records whether self-harm is a past or active problem, recurrent or one-off behaviour may be missing and GPs may be underestimating the prevalence of self-harm in the 11 to 14 years age range.3 One way to improve recording is for clinicians to discuss with young people what is being written in their medical record and for primary care staff, including administrators, to receive training to support consistency of recording.
INTERVENTIONS FOR YOUNG PEOPLE’S SELF-HARM
Despite young people’s self-harm being on the increase, studies of GP-based interventions are lacking and/or inconclusive.10 In part this lack of evidence about what works may be explained by the heterogeneity of young people’s self-harm, as discussed earlier.
When young people present to their GP’s surgery with self-harm associated with psychosocial distress related to developmental milestones, self-help resources can play a role in supporting young people to manage this distress/stress. Examples of self-help are many and varied: from online interactive approaches based on principles of cognitive behavioural therapy through to blog sites and personalised safe-kits that include ‘tools’ to help young people cope with their urges to self-harm. For young people whose self-harm co-presents with clinical symptoms of anxiety and depression, GPs are likely to be prescribing medication, and NICE guidelines advocate using self-help alongside medication in a supportive package of care.11 In our study young people reported that they found these self-help resources useful,6 but more robust evaluations of their effectiveness are needed. For young people whose self-harm is persistent and/ or life threatening, GPs do refer to mental health services but are concerned that young people will not access this specialist help.3 Young people’s engagement with a range of interventions for self-harm including short consultations in primary care requires further longitudinal evaluations so that we can better understand what works.
Notes
Provenance
Commissioned; not externally peer reviewed.
- © British Journal of General Practice 2017
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

