


INTRODUCTION
Idiopathic pulmonary fibrosis (IPF) is the commonest interstitial lung disease (ILD) and is characterised by progressive scarring of the lungs. It typically presents in the sixth or seventh decade.1 The prognosis of IPF is poor and is worse than most cancers, with a median survival from diagnosis of 2.5–3.5 years.1 In 2012, over 5000 people died of IPF in the UK accounting for 1% of all deaths and 4.6% of respiratory deaths.2 On average, a general practice of 10 000 patients will see 2–3 new cases every 3 years,3 although this is likely to be an underestimate, contrasting with 500 per 10 000 for chronic obstructive pulmonary disease (COPD). The rising incidence and prevalence means that GPs will be pivotal in the early detection and long-term management of patients with IPF.
DIAGNOSIS
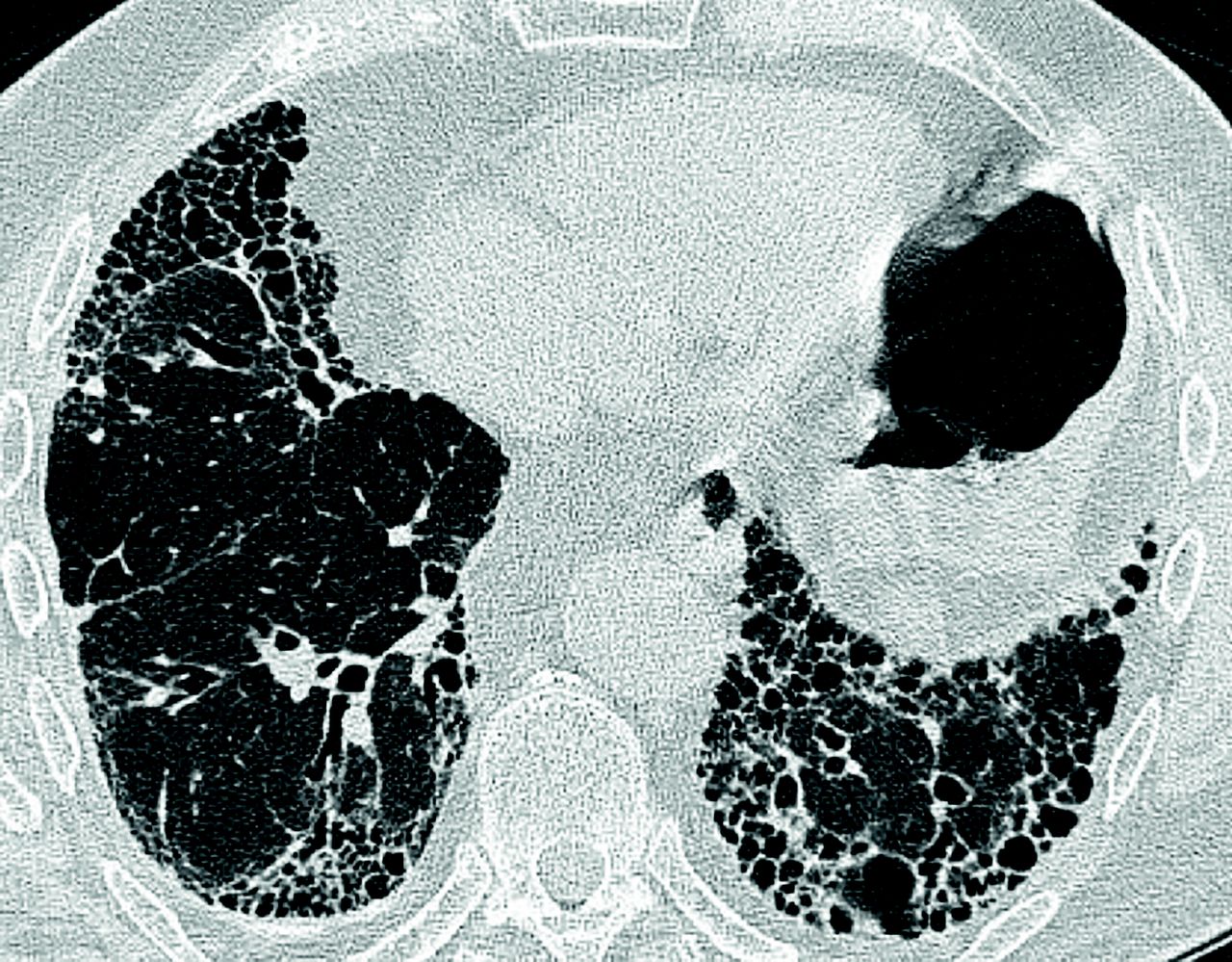
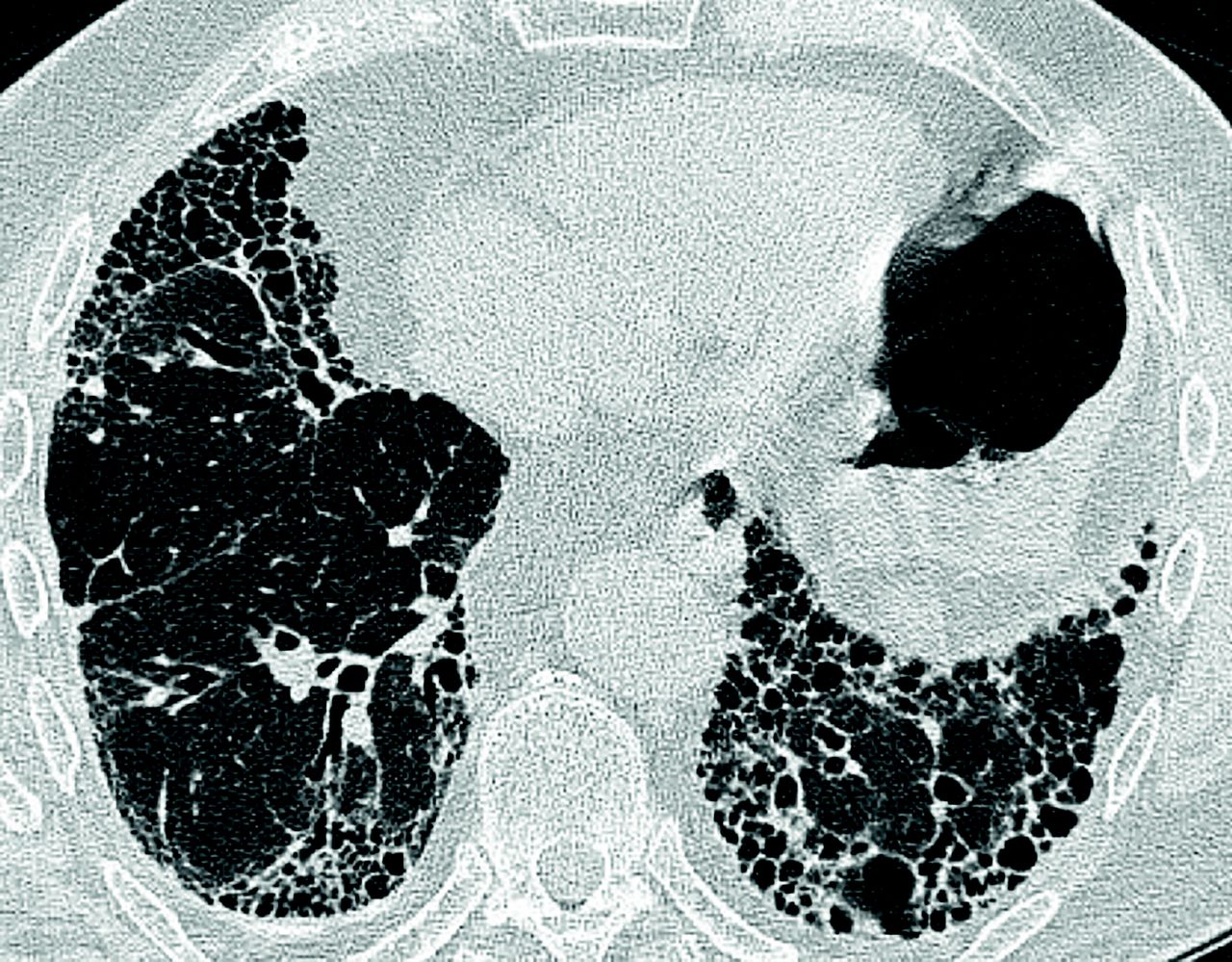
Patients with IPF typically present first to their GP. Distinguishing these symptoms from more common conditions such as COPD can be challenging. A history of persistent progressive breathlessness and/or cough in a patient >45 years who may, but not exclusively, have velcro crackles on auscultation and finger clubbing should warrant further management with radiological imaging (chest X-ray and high-resolution computed tomography [Figure 1]) and/or referral to an IPF specialist.3
{kind=link}
CT thorax showing classical usual interstitial pattern seen in IPF with subpleural reticulation, basal predominance, and honeycombing. CT = computed tomography. IPF = Idiopathic pulmonary fibrosis.
©Manchester University NHS Foundation Trust image library.
MANAGEMENT
Antifibrotic therapy
There are now two antifibrotic therapies approved for management of IPF by the National Institute for Health and Care Excellence (NICE): pirfenidone and nintedanib. Prescribing is restricted by NICE to ILD specialist centres in England and is licensed for patients with a forced vital capacity (FVC) between 50–80% predicted. NICE mandates that treatment should be stopped if there is a decline in FVC >10% within a 12-month period. Both therapies have shown similar reduction in FVC decline and in pooled data pirfenidone decreases mortality in IPF.
Adverse effects of antifibrotics
Both antifibrotics have similar effects on lung function. The decision as to which treatment to start is based on joint decision making between patient and physician because it is important to discuss the intentions of treatment to slow decline or stabilise disease. The patient’s expectations of a new treatment need to be addressed by advising them that the antifibrotic treatments have not been shown to improve breathlessness. Strategies to manage symptoms with breathlessness management techniques, oxygen assessment, and pulmonary rehabilitation must occur in parallel to starting antifibrotic medication. The choice of antifibrotic is a joint decision between patient and physician after discussing the relative potential side effect profiles and contraindications of each treatment.
Both pirfenidone and nintedanib have side effect profiles that require careful education and management to maintain adherence and maximise efficacy. Adverse effects of pirfenidone include nausea, vomiting, dyspepsia, and skin disorders such as rashes and photosensitivity. Pirfenidone is generally well tolerated and most adverse events are mild to moderate in nature. Common adverse events with nintedanib include diarrhoea, nausea, vomiting, and cough. Again, adverse events tend to be mild to moderate in severity.
Holistic management
The crucial role of the ILD nurse specialists
ILD specialist nurses are pivotal in the care of patients with IPF. NICE suggests that all patients and partners affected by IPF should have access to a specialist nurse through all phases of the disease.3 ILD specialist nurses are involved throughout the patient journey from initial diagnosis, to continued management, and during end-of-life care. The ILD specialist nurses provide an important link between the multidisciplinary team and the GP.
Managing adverse effects of antifibrotic medication
The majority of antifibrotic side effects are gastrointestinal. Patients are advised to take antifibrotics during a meal and divide the dosage across the meal. Indigestion should be treated with a proton-pump inhibitor. Diarrhoea, particularly with nintedanib, may be managed with rehydration and antidiarrhoeal medication, for example, loperamide. Anti-emetics may also be used to treat nausea. Pirfenidone may cause a skin rash or photosensitivity Preventive advice should be given, including avoiding direct sun exposure, wearing protective clothing, and applying UVA and UVB sunscreen factor 50. Ongoing side effects may require supervised dose reduction and re-titration once the symptoms have subsided.
Symptom management
IPF has a significant impact on a patient’s quality of life.4 This may be as a result of physical symptoms including cough and breathlessness or psychosocial factors such as depression and anxiety. Following a diagnosis of IPF, best supportive care should be offered in parallel to antifibrotic medication.
This care should include advice about how to manage any symptoms. Chronic breathlessness is common in patients with IPF and can trigger frequent hospital admissions. There has been a move towards non-pharmacological management of breathlessness. The use of patient education, anxiety management, support for carers, and fan therapy have all been shown to improve breathlessness control.5 Cough in IPF is usually severe and not easily amenable to treatment. Unfortunately, there is little evidence base for effective cough treatments in IPF and thus needs to be a major focus of research.
The use of ambulatory oxygen in IPF remains controversial. It is aimed at improving exercise capacity and relieving symptoms of breathlessness. Timely referral for ambulatory oxygen therapy assessment is recommended by NICE.3
All patients with IPF should have access to pulmonary rehabilitation.3 Pulmonary rehabilitation improves clinical outcomes and symptoms in IPF.3 Provision of pulmonary rehabilitation for patients with IPF can be patchy and is delivered largely via COPD-targeted programmes. Improved access for patients with IPF and condition-specific programmes are key targets for improving IPF care.
CONCLUSION
There have been significant changes to IPF management following the advent of two antifibrotic therapies. Patients will want to be informed of potential therapies and, to this effect, the GP plays an important role in both timely detection and referral of patients to specialist ILD centres and maintaining up-to-date knowledge to effectively inform patients. The GP is pivotal in all aspects of IPF management and can aid in smoking cessation, psychological support, and management of comorbidities. The GP provides a crucial link between primary care and the specialist ILD team with the aim of improving patient quality of life and end-of-life care.
Notes
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: www.bjgp.org/letters
- Received July 15, 2017.
- Revision requested September 30, 2017.
- Accepted October 10, 2017.
- © British Journal of General Practice 2018
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

