


Article Figures & Data
Figures
- Figure 1.
Number of people aged ≥65 years prescribed each of the study drugs. ACEI = angiotensin-converting enzyme inhibitor. ARB = angiotensin II receptor blocker. NSAID = non-steroidal anti-inflammatory drug.
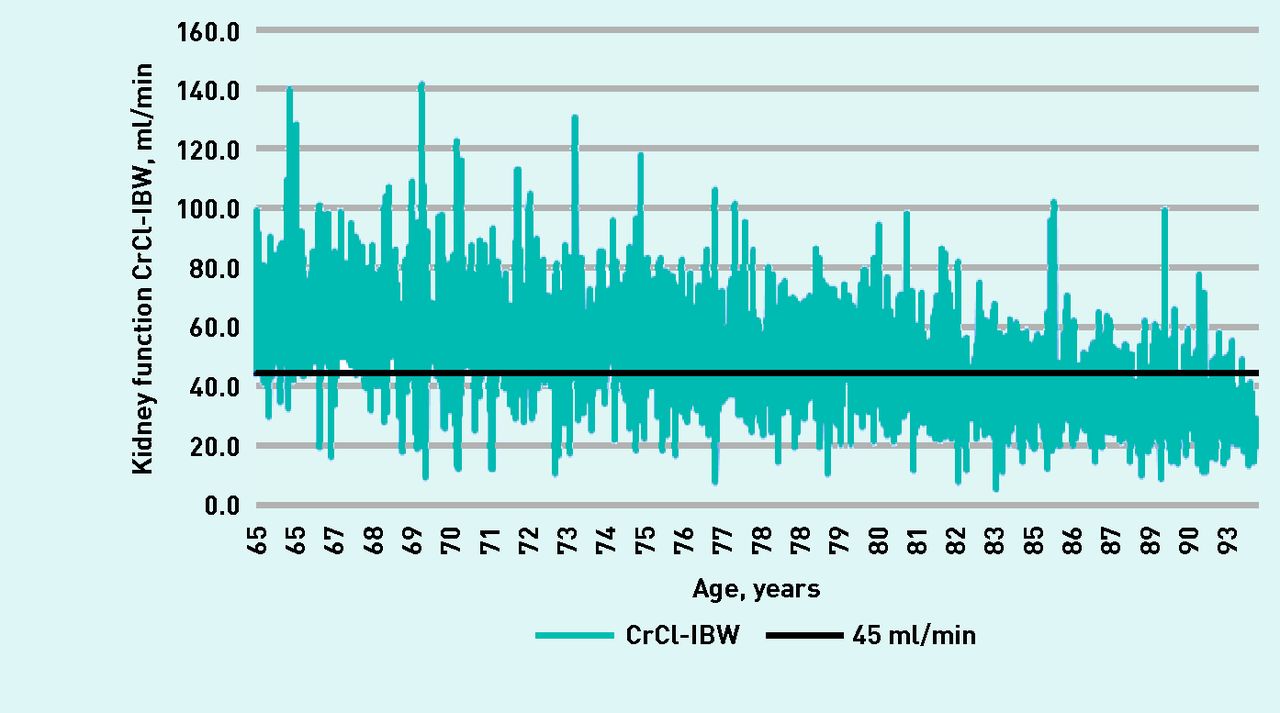
- Figure 2.
Range of kidney function using creatinine clearance (Cockcroft–Gault) calculated using estimated ideal body weight (CrCl-IBW) in the previous 15 months, for nitrofurantoin prescribed at each age level ≥65 years.
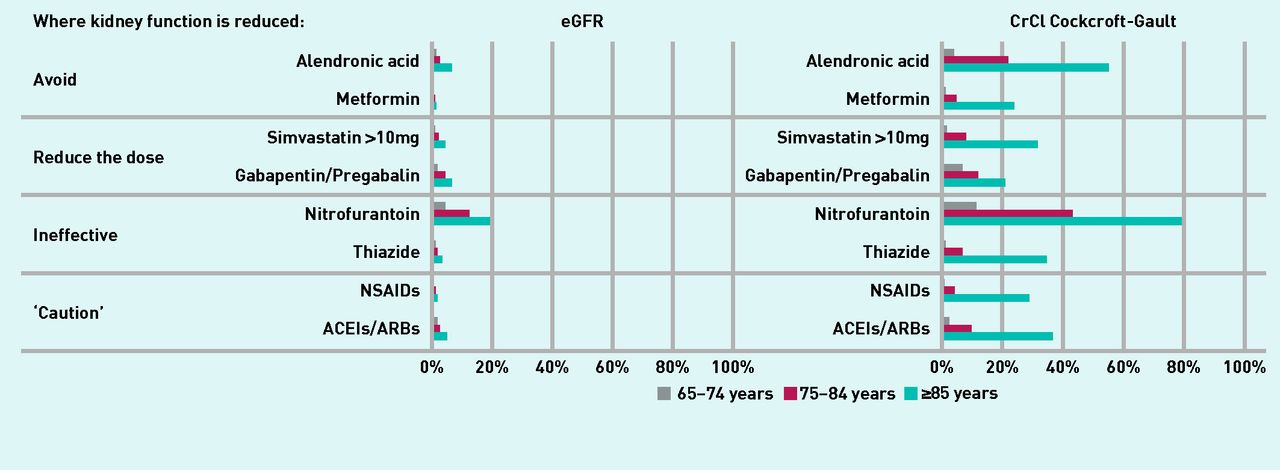
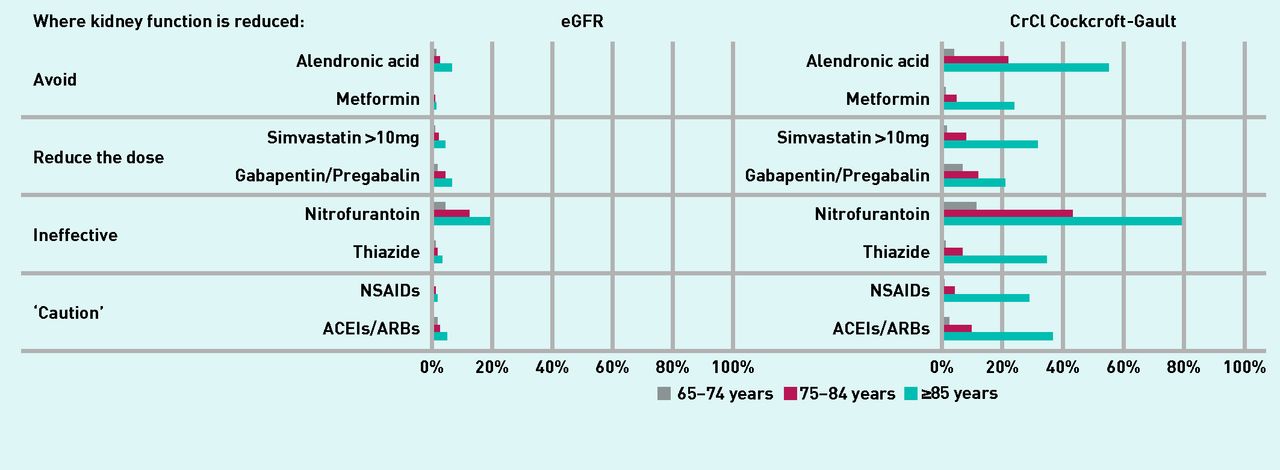
- Figure 3.
Percentage of patients found with a kidney function too low for recommended use of the drug using estimated glomerular filtration rate compared with creatinine clearance (Cockcroft–Gault) in the three older age bands. ACEIs = angiotensin-converting enzyme inhibitor. ARBs = angiotensin II receptor blockers. CrCI = creatinine clearance. eGFR = estimated glomerular filtration rate. NSAIDs = non-steroidal anti-inflammatory drugs.

{kind=link}
{kind=link}
{kind=link}
Tables
Category: recommendation when kidney function is reduced Drug BNF13/SPC recommendation Prescribing outside recommendations, or dose suggested may need review, in a case-note review study,24 % References where prescribing outside recommendations was reported Evidence of potential impact for patients Comments from independent expertsa Avoid Alendronic acid SPC: not recommended BNF: avoid if CrCl <35 ml/min 4.0 Breton et al5
Khanal et al22Alendronic acid accumulates in the bones, with a terminal half-life >10 years41
MHRA review of risks: associated with an increased risk of atypical stress fractures of the proximal femoral shaft; low but increased risk of atrial fibrillation33
Agreed to be included Metformin SPC: contraindication
<30 ml/min2.0 Breton et al5
Khanal et al (2015)22
Schmidt-Mende et al (2012)25Increased risk of lactic acidosis especially with dehydration34
Suggested by a renal physician and a geriatrician as they see admissions to hospital caused by metformin when kidney function is low Reduce the dose Simvastatin SPC/BNF: CrCl <30 ml/min: dosages
>10 mg/day should be carefully considered and, if deemed necessary, implemented cautiously8.8 Breton et al5 Total drug (AUC) 2–3 times greater when kidney function is low [personal communication Merck Sharp & Dohme, 2011] (that is, greater than the effect of the drug interaction with amlodipine: AUC for simvastatin increased by 1.58–1.77 fold35)
MHRA: increased plasma concentrations of simvastatin are associated with an increased risk of myopathy and/or rhabdomyolysis35
Agreed to be included as a widely-used drug with an alternative available (atorvastatin does not need dose alteration when kidney function is low)42 Gabapentin and pregabalin Table of reduced doses at specified levels of CrCl 0.2 Breton et al5 High risk from the common adverse effects of somnolence, dizziness, ataxia, and fatigue43,44
There has been a 46% rise in prescribing of gabapentin and 53% rise in pregabalin prescribing since 201136
Added at the suggestion of the renal pharmacist because of frequent side effects seen in the renal unit Ineffective Thiazides BNF: likely to be ineffective at CrCl <30 ml/min 17.0 Howard et al26 Unlikely to be effective below 30 ml/min45
Increased risk of adverse events such as electrolyte imbalance25
Agreed to be included Nitrofurantoin BNF: likely to be ineffective at CrCl <45 ml/min SPC: contraindicated <45 ml/min; may be used with caution 30–44 ml/min — only prescribe to such patients to treat lower urinary tract infection with suspected or proven multidrug-resistant pathogens when the benefits of nitrofurantoin are considered to outweigh the risks of side effects 0.2 (on repeat) Farag et al27
Geerts et al28
Howard and Wood21MHRA: The antibacterial efficacy depends on the renal secretion of nitrofurantoin into the urinary tract. In patients with renal impairment, renal secretion of nitrofurantoin is reduced. This may reduce the antibacterial efficacy, increase the risk of side effects (for example, nausea, vomiting, loss of appetite), and may result in treatment failures37
The drug may not work increasing risk from infection.46 An audit in a large GP practice found older people with renal impairment were more likely to need further antibiotics21
Raised blood levels increases the risk of pulmonary, hepatic, neurological, haematological, and gastrointestinal side effects during treatment; <50 ml/min significantly increased the risk of pulmonary adverse events leading to hospitalisation (HR = 4.1, 95% CI = 1.39 to 13.09)28
Agreed to be included; issue raised after discussion with a pharmacist with international expertise in antibiotics Caution as adverse drug reactions are likely NSAIDs BNF: caution in reduced kidney function (study parameter set at <30 ml/min) 1.7 Evans et al29
Guthrie et al30
Howard et al26
Ingrasciotta et al31Sodium and water retention may occur and renal function may deteriorate, possibly leading to renal failure; deterioration in renal function has also been reported after topical use13
Chronic use of NSAIDs is a risk factor for progression of CKD8
Frequently cited as causing admissions38
Agreed to be included: NSAIDs affect all stages of kidney function and are frequently a cause of hospital admission ACEIs and ARBs BNF: caution in reduced kidney function (study parameter set at <30 ml/min) 26.0 Breton et al5
Handler et al32
Khanal et al22
Schmidt-Mende et al25Ramipril SPC: CrCl <60 ml/min maximum dose is 5 mg47
Hyperkalaemia and other side effects of ACEIs are more common, and the dose may need to be reduced13
Can cause impairment of kidney function which may progress and become severe (at particular risk are older people)13
STOP-ACEi study is investigating whether the risk to the kidney may outweigh any beneficial effect if <30 ml/min39
Although ACEIs and ARBs are used in renal disease, they can also be nephrotoxic so the consultant experts suggested inclusion ↵a Independent experts were a renal physician with a national role, geriatrician, hospital renal pharmacist, and an antibiotics expert pharmacist. ACEIs = angiotensin-converting enzyme inhibitors. ARBs = angiotensin II receptor blockers. AUC = area under the curve. BNF = British National Formulary. CrCl = creatinine clearance. HR = hazard ratio. MHRA = Medicines and Healthcare products Regulatory Agency. NSAIDs = non-steroidal anti-inflammatory drugs. SPC = summary of product characteristics.
- Table 2.
Number of drugs prescribed for people aged ≥65 years with a kidney function estimate (CrCl-CG IBW) in the previous 15 months below that for recommended use
Drug Aged ≥65 years Aged 65–74 years Aged 75–84 years Aged ≥85 years Total Kidney function <recommended % 95% CI Total Kidney function <recommended % 95% CI Total Kidney function <recommended % 95% CI Total Kidney function <recommended % 95% CI Alendronic acid 3400 804 23.6 19.2 to 28.1 1120 49 4.4 3.6 to 5.1 1532 342 22.3 20.1 to 24.6 748 413 55.2 48.6 to 61.8 Metformin 6276 267 4.3 1.2 to 7.3 3491 30 0.9 0.81 to 0.91 2319 124 5.3 4.9 to 5.8 466 113 24.2 16.4 to 32.1 Simvastatin >10 mg 19 434 1465 7.5 6.6 to 8.5 9894 167 1.7 1.65 to 1.72 7494 643 8.6 8.4 to 8.8 2046 655 32.0 29.9 to 34.1 Gabapentin or pregabalin 1209 132 10.9 0 to 25.7 598 43 7.2 5.0 to 9.4 450 56 12.4 7.6 to 17.3 161 33 20.5 0.3 to 40.7 Nitrofurantoin 3185 1262 39.6 35.8 to 43.4 1206 141 11.7 10.0 to 13.4 1242 535 43.1 39.1 to 47.0 737 586 79.5 75.1 to 83.9 Thiazide 10 805 797 7.4 5.7 to 9.1 5371 62 1.2 1.11 to 1.20 4189 303 7.2 6.9 to 7.6 1245 432 34.7 31.1 to 38.3 NSAID 2483 86 3.5 0 to 11.2 1577 8 0.5 0.44 to 0.57 762 36 4.7 3.5 to 5.9 144 42 29.2 0.5 to 57.9 ACEI/ARB 26 109 2521 9.7 9.0 to 10.3 12 663 288 2.3 2.24 to 2.31 10 280 1062 10.3 10.2 to 10.5 3166 1171 37.0 35.5 to 38.5 ACEI = angiotensin-converting enzyme inhibitor. ARB = angiotensin II receptor blocker. CrCl-IBW = creatinine clearance (Cockcroft–Gault) calculated using estimated ideal body weight. NSAID = non-steroidal anti-inflammatory drug. Patients with no eGFR on the record, or kidney function data older than 15 months, were excluded for the final analysis (9911/96 900 (10.2%) patient drug events).
- Table 3.
The odds of having a kidney function too low for the drug with increased age compared with those aged 65–74 years, using eGFR, creatinine clearance (Cockcroft–Gault) calculated using actual body weight, and using ideal body weight
Drug Kidney function calculation 65–74 years 75–84 years ≥85 years Odds ratio Odds ratio 95% CI Odds ratio 95% CI Alendronic acid eGFR 1 1.96 1.08 to 3.56 5.49 3.07 to 9.81 CrCl-AW 1 5.11 3.59 to 7.26 24.12 16.93 to 34.36 CrCl-IBW 1 6.28 4.61 to 8.57 26.95 19.56 to 37.13 Metformin eGFR 1 2.26 0.80 to 6.35 6.15 1.87 to 6.35 CrCl-AW 1 5.90 3.20 to 10.88 48.64 26.70 to 88.61 CrCl-IBW 1 6.52 4.36 to 9.75 36.93 24.33 to 58.05 Simvastatin >10 mg eGFR 1 2.45 1.89 to 3.17 4.98 3.71 to 6.70 CrCl-AW 1 5.03 4.06 to 6.23 30.64 24.73 to 37.95 CrCl-IBW 1 5.47 4.60 to 6.50 27.43 22.93 to 32.80 Gabapentin/pregabalin eGFR 1 2.73 1.27 to 5.89 4.28 1.78 to 10.26 CrCl-AW 1 2.97 1.55 to 5.72 9.96 5.25 to 18.88 CrCl-IBW 1 1.83 1.21 to 2.79 3.33 2.03 to 5.45 Nitrofurantoin eGFR 1 3.03 4.20 to 4.18 5.24 3.78 to 7.27 CrCl-AW 1 6.79 5.16 to 8.92 41.33 30.87 to 55.36 CrCl-IBW 1 5.64 4.58 to 6.95 29.23 22.75 to 37.56 Thiazides eGFR 1 2.19 1.42 to 3.37 5.29 3.32 to 8.43 CrCl-AW 1 5.60 3.96 to 7.93 49.67 35.52 to 69.44 CrCl-IBW 1 6.68 5.07 to 8.80 45.50 34.52 to 59.98 NSAIDs eGFR 1 4.20 1.05 to 16.84 3.68 0.38 to 35.57 CrCl-AW 1 3.50 1.52 to 8.03 43.93 20.31 to 95.03 CrCl-IBW 1 9.73 4.50 to 21.03 80.76 36.94 to 176.55 ACEIs/ARBs eGFR 1 1.81 1.49 to 2.21 3.84 3.09 to 4.78 CrCl-AW 1 4.73 3.98 to 5.61 29.01 24.27 to 34.38 CrCl-IBW 1 4.95 4.33 to 5.65 25.22 21.99 to 28.93 ACEIs = angiotensin-converting enzyme inhibitors. ARBs = angiotensin II receptor blockers. CrCl-AW = creatinine clearance (Cockcroft-Gault) calculated using actual body weight. CrCl-IBW = creatinine clearance (Cockcroft-Gault) calculated using ideal body weight. eGFR = estimated glomerular filtration rate. NSAIDs = non-steroidal anti-inflammatory drugs.
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

