


Abstract
Background Acute upper respiratory infections (AURI) are the leading causes of antibiotic prescribing in primary care although antibiotics are often not indicated.
Aim To gain an understanding of the knowledge, attitudes, and practices (KAP) of GPs in Singapore and the associated latent factors to guide the implementation of an effective programme to reduce antibiotic use in primary care.
Design and setting: An anonymous survey on the KAP of antibiotic use in AURI of GPs in Singapore.
Method KAP survey questionnaires were posted to all GPs from a database. To ascertain the latent factors affecting prescribing patterns, exploratory factor analysis was performed.
Results Among 427 responses, 351 (82.2%) were from GPs working in private practice. It was found that 58.4% of GPs in the private versus 72.4% of those in the public sector recognised that >80% of AURIs were caused by viruses (P = 0.02). The majority of GPs (353/427; 82.7%) felt that antibiotics were overprescribed in primary care. Significant factors associated with low antibiotic prescribing were good medical knowledge and clinical competency (adjusted odds ratio [aOR] 3.2, 95% confidence interval [CI] = 2.4 to 4.3), good clinical practice (aOR 2.7 [95% CI = 2.0 to 3.6]), availability of diagnostic tests (aOR 1.4 [95% CI = 1.1 to 1.8]), and desire to improve clinical practice (aOR 1.5 [95% CI = 1.2 to 1.9]). The conservative practice of giving antibiotics ‘to be on the safe side’ is significantly less likely to be associated with low antibiotic prescribing (aOR 0.7 [95% CI = 0.5 to 0.9]).
Conclusion This is the first KAP survey on antibiotic prescribing for AURI among GPs in Singapore. With the latent factors identified, future interventions should be directed at addressing these factors to reduce inappropriate antibiotic prescribing.
INTRODUCTION
Acute upper respiratory infections (AURI) are leading causes of attendance in general practice. Despite the fact that the majority of AURI are caused by viruses and that antibiotics are not recommended for the common cold, acute rhinitis,1 and acute bronchitis,2 antibiotics continue to be overprescribed in these settings.3,4 Acute respiratory syndromes account for approximately 75% of ambulatory antibiotic prescription in the US.5 In the UK, the use of antibiotics in general practice, accounting for 74% of antibiotics use overall, increased by 6.4% from 2010 to 2014.6 Inappropriate antibiotic use exposes patients to unnecessary drug toxicities, drug–drug interactions, increased healthcare costs, and risk of infections by community-acquired drug-resistant organisms.7–10 In Singapore, AURI accounted for 30% of all primary care consultations.11 Antibiotics were among the top 10 drugs prescribed in primary care polyclinics in the public sector.12 In just a decade (from 1997 to 2007–2008), the prevalence of multidrug-resistant Streptococcus pneumoniae in Singapore jumped from 33.3% to 74.6%.8
The decision to prescribe antibiotics to a patient with AURI is complex and many factors are involved. These include:
physicians’ fears of patients having medical complications;13
insufficient physician knowledge;14
belief that antibiotic resistance was not a problem at the community level;15
underestimating the effect that inappropriate prescribing of antibiotics has on microbial resistance; and16
The above reasons influencing antibiotic prescribing can be partly accounted for by socioeconomic and cultural environments, which differ between geographical locations and communities.19,20
The World Health Organization (WHO) in its Global Action Plan on Antimicrobial Resistance21 has identified optimising antimicrobial medicines as one of its strategic objectives. To guide the design and implementation of strategies to reduce antibiotic use for AURI in Singapore, the authors conducted a survey of GPs to ascertain their knowledge, attitudes, and practices (KAP) in antibiotic prescribing for AURI in Singapore. The authors believe that this is the initial step for reducing antibiotic use in primary care.
How this fits in
It is known that antibiotics are overprescribed in primary care and drug resistance is one of the most pressing issues today. So far there have been no studies in Singapore examining the factors affecting antibiotic prescribing for acute upper respiratory infections (AURI) among primary care physicians. This study found that good medical knowledge and clinical practice, together with availability of diagnostic tools and GPs’ desire to improve clinical practice, are important factors in reducing antibiotic prescribing. These findings will help guide future studies and interventions on antimicrobial stewardship in the primary care setting.
METHOD
Survey questionnaire
After reviewing the related literature, a survey instrument was developed (Appendix 1) with questions on the KAP of primary care physicians towards antibiotics prescribing for AURI in Singapore. It was tested for practicality and ease of use on 10 junior doctors working in a medical department, feedback was collected, and adjustments then made. Questions were either on a 4-point (1 = never, 2 = infrequently, 3 = frequently, 4 = always) or a 5-point Likert scale (range from 1 = strongly disagree to 5 = strongly agree). In addition, demographic data were collected.
Conducting the survey
In total, 1417 survey questionnaires were posted to all primary care physicians at three different time points between 2012 and 2015 in both public (polyclinic) and private healthcare sectors (‘polyclinic’ in the Singapore clinical setting refers to having multiple primary care clinical consultation rooms under one roof). The distinction between public and private sectors was made as providers in the private sector might have a financial incentive to prescribe and dispense antibiotics. Public providers consist of practitioners working in the authors’ institution’s healthcare cluster. The healthcare cluster belongs to National Healthcare Group, Singapore. Tan Tock Seng Hospital and the polyclinics (public) included in this study are in this healthcare cluster. This is one of two such clusters operating polyclinics scattered across Singapore. The postal addresses of all the private providers were obtained from the Singapore Medical Council database. The anonymous responses were returned using the prepaid envelopes provided. The questionnaire did not contain any identifiers and could not be traced to the participating GP. Individuals who participated were asked not to respond if they received the same survey again.
Statistical analysis
In order to determine the latent factors influencing antibiotic prescribing by primary care physicians, exploratory factor analysis (EFA) was performed. Factor extraction was done using principal component factoring, and varimax rotation was used to preserve the independence of the factors. The number of factors was decided by inspecting the scree plot, eigenvalues, and the cumulative variance explained. The Kaiser–Meyer–Olkin (KMO) test was performed to check for overall sampling adequacy and Cronbach’s α was used to measure the internal consistency of each factor. Logistic regression was performed to identify independent factors associated with low prescribing, adjusted for practice type. Low prescribing was defined as the prescribing of antibiotics by GPs to fewer than 20% of their patients with AURI, as only 20% of AURI are caused by bacteria.
All analyses were done using STATA (version 13) and R 3.0.2 at a 5% significance level.
RESULTS
The authors received 427 responses (Table 1), of which 351 (82.2%) were from GPs working in a private practice and the rest were from GPs working in the public sector (polyclinic). The distribution of GPs was similar to that reported in the Singapore Ministry of Health’s primary care survey.22 Among the survey participants, 148 (34.7%) held a postgraduate qualification in family medicine. Among those in private practice, two (0.57%) had completed their primary medical degree within the previous 5 years, 16 (4.56%) in the previous 6–15 years, and 333 (94.9%) >15 years previously In the public sector, the numbers were 20 (26.3%), 28 (36.8%), and 28 (36.8%) respectively.
Demographics of responders
Selected KAP responses are summarised in Table 2. Two hundred and five of 351 (58.4%) of GPs in the private versus 55 of 76 (72.4%) of those in the public sector recognised that >80% of acute respiratory infections were caused by viruses (P = 0.02). Regarding clinical indications for giving antibiotics, 377/427 (88.3%) of responders thought antibiotics were indicated in acute otitis media, 334 (78.2%) for acute sinusitis, and 390 (91.3%) for tonsillitis. About half (228 of 427, 53.4%) thought that antibiotics were indicated in tracheobronchitis, 103 (24.1%) for laryngitis/pharyngitis, and 13 (3.04%) for rhinitis.
Knowledge, attitude, and practices responses
Among GPs from the private sector, 139/351 (39.6%) deemed themselves to have a low antibiotic prescribing practice, compared with 61/76 (80.3%) of GPs in the public sector polyclinics (P<0.01). Low prescribers were more likely to have obtained their primary medical qualification in Singapore (P<0.01), but did not necessarily have a postgraduate qualification in family medicine (P = 0.45). GPs felt that the most serious problems they foresaw in overprescribing antibiotics were:
the development of antibiotic resistance (390; 91.3%);
possible adverse reactions (28; 6.6%);
increased costs (3; 0.7%); and
drug–drug interactions (1; 0.2%).
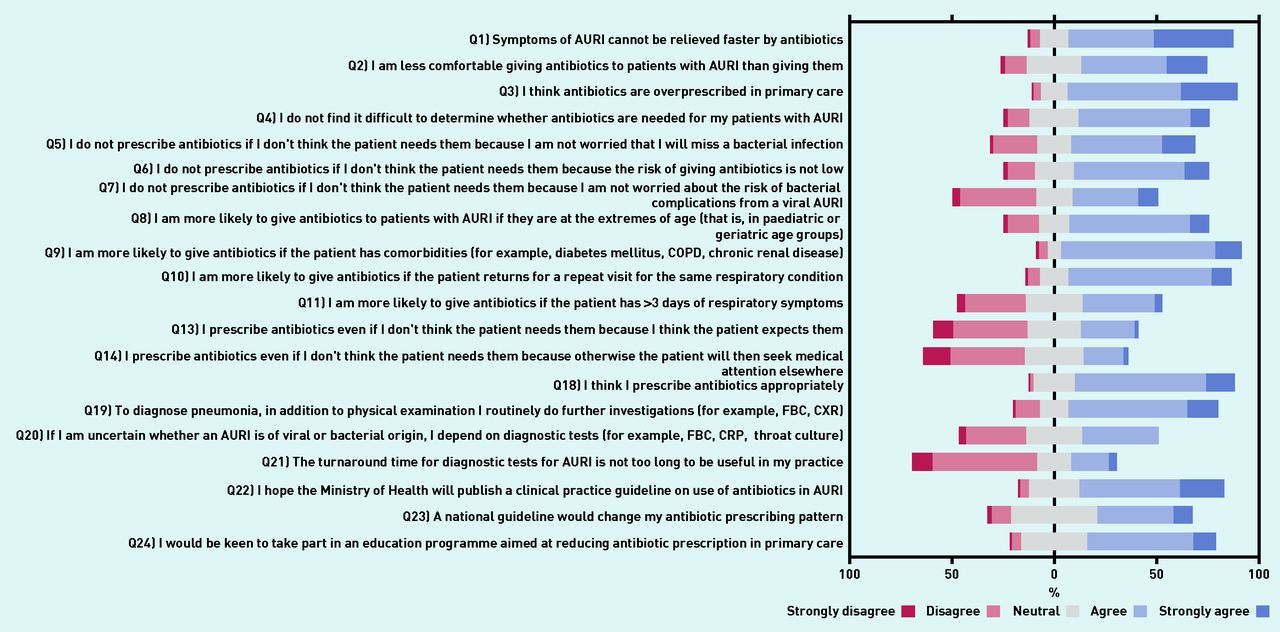
The Likert scale responses are presented in Figures 1 and 2. The majority of GPs (353/427; 82.7%) thought that antibiotics were overprescribed in the primary care setting (Q3) but most (333/427; 78.0%) also thought that they prescribed antibiotics appropriately (Q18). Not surprisingly, GPs were more likely to prescribe antibiotics to patients who were at the extremes of age (290/427; 67.9%) (Q8), had comorbidities (376/427; 88%) (Q9), and returned for repeat visits for the same respiratory condition (339/427; 79.4%) (Q10). Only 38.4% thought that they were more likely to prescribe antibiotics if the patient had >3 days of respiratory symptoms (Q11).

Five-point Likert scale responses. AURI = acute upper respiratory tract infections. COPD = chronic obstructive pulmonary disease. CRP = C-reactive protein. CXR = chest X-ray. FBC = full blood count.

{kind=link}
{kind=link}
Four-point Likert scale responses. AURI = acute upper respiratory tract infections.
The majority (70.5%) hoped that the Ministry of Health would publish clinical practice guidelines on antibiotic use in AURI (Q22) although only half (46.3%) felt that the national guidelines would change their prescribing practices (Q23). Encouragingly, 62.5% would be keen to take part in an education programme aimed at reducing antibiotic prescribing in primary care (Q24). Based on the number of factors with eigenvalue >1 in the scree plot, the authors extracted six factors from the factor analysis for inclusion in the multivariable model (Appendix 2). The six-factor model accounting for 57.5% of the total variance (KMO test = 0.82) was deemed most suitable. The latent factors are: Factor 1 — medical knowledge and clinical competency (seven items; loadings ranged from 0.36 to 0.70; α = 0.74); Factor 2 — conservative practice (giving antibiotics ‘to be on the safe side’) (four items; loadings ranged from 0.51 to 0.77; α = 0.66); Factor 3 — GPs’ perceived patient expectations (three items; loadings ranged from 0.62 to 0.73; α = 0.61); Factor 4 — good clinical practice (four items; loadings ranged from 0.58 to 0.61; α = 0.64); Factor 5 — availability of diagnostic tests (three items; loadings ranged from 0.56 to 0.82; α = 0.62); Factor 6 — desire to improve clinical practice (three items; loadings ranged from 0.70 to 0.83; α = 0.73) (Table 3). Conservative or prudent practice (giving antibiotics ‘to be on the safe side’) was moderately correlated with perceived patient expectations (r = 0.42).
The latent factors of antibiotic prescribing
On multivariable analysis, medical knowledge and clinical competency (OR 3.2 [95% CI = 2.4 to 4.3]), good clinical practice (OR 2.7 [95% CI = 2.0 to 3.6]), availability of diagnostics (OR 1.4 [95% CI = 1.1 to 1.8]), and the desire to improve clinical practice (OR 1.5 [95% CI = 1.2 to 1.9]) were significantly associated with low prescribing, after adjusting for the practice type (Table 4). Notably, clinical competency and good clinical practice were most strongly associated with low prescribing. Conservative practice (prescribing antibiotics ‘to be on the safe side’) was significantly less likely to be associated with low prescribing (OR: 0.7 [95% CI = 0.5 to 0.9]).
Effects sizes of the six latent factors on low prescribing
DISCUSSION
Summary
In order to reduce antibiotic prescribing among GPs, it is vital to understand the ‘local’ beliefs and practices, that is, the cultural and socioeconomic environment, before implementing any interventions. This study has identified physicians’ medical knowledge and clinical competency, good clinical practice, availability of diagnostic tests, and desire to improve clinical practice as significant factors associated with low antibiotic prescribing. Being conservative and giving antibiotics ‘to be on the safe side’ is also significantly less likely to be associated with low antibiotic prescribing.
Strengths and limitations
The authors acknowledge that this study could have been limited by bias due to non-participation. However, the profile of GPs who participated in the study was representative of the GP population in Singapore and hence any potential selection bias is likely to be minimal. In addition, although the study’s findings were self-reported, the protection of the identity of study participants in the study processes ensured that social desirability bias was very unlikely to have occurred and that the answers provided by the GPs were likely to be authentic. The fact that GPs were not compensated for their time and were not incentivised to participate in the study lends credibility to the findings, as the GPs would have returned the survey questionnaire purely out of their desire to improve clinical practice and patient care.
Comparison with existing literature
Half (47.8%) of GPs were unaware of a scoring system to assess the likelihood of streptococcal throat infection and half (50.8%) thought that a purulent nasal discharge was indicative of a bacterial infection. In addition, a large proportion (up to 91.3%) of GPs thought that empirical antibiotics were indicated for AURI. This analysis showed that medical knowledge and clinical competency (Factor 1) was the most significant factor associated with low prescribing (aOR 3.2, 95% CI = 2.4 to 4.3). As was similarly observed in the Netherlands, the knowledge gap among GPs on the effects of antibiotics on AURI could lead to high rates of antibiotic prescribing in the community.23 An education programme for providers in the UK has shown effectiveness in reducing antibiotic prescribing in primary care24 and a similar programme may be adopted in Singapore. Two-thirds (62.5%) of the GPs in the current study have expressed interest in participating in educational programmes aimed at reducing antibiotic prescribing in primary care.
GPs have been observed to prescribe antibiotics more readily if their patients are at the extremes of age, have significant comorbidities, or have a longer duration of symptoms of AURI, just ‘to be on the safe side’.9,25 This is probably related to fear of complications in these vulnerable groups.16 Although antibiotics were not justified for the prevention of serious complications for AURI,26 the current analysis showed that such conservative practice (Factor 2) played a significant role in antibiotic prescribing. Such an approach is significantly less likely to be associated with low prescribing (aOR 0.7 [95% CI = 0.5 to 0.9]).
Good clinical practice (Factor 4) was strongly associated with low prescribing (aOR 2.7 [95% CI = 2.0 to 3.6]). Physicians who took the time to explain and convince their patients that antibiotics were not necessary tended to be low prescribers. Patient volume might be a contributory factor, with busier physicians being more liberal in prescribing antibiotics to hasten the consultation process.9,25 Interventions should be designed to educate the GPs that antibiotics are not ‘quick fix’ solutions to speed up consultations, and to simplify the decision-making process.16
As discussed earlier, the fear of misdiagnosis of viral AURI or the development of complications from it contribute to increased antibiotic prescribing by GPs. Not surprisingly, the availability of diagnostic tests (Factor 5) was observed to influence prescribing decisions in this study’s multivariate analysis (aOR 1.4 [95% CI = 1.1 to 1.8]) and 281/427 (65.8%) of the participants expressed a willingness to use a point-of-care (POC) test to guide their antibiotic prescribing. A systematic review by Aabenhus and colleagues showed that using POC C-reactive protein testing reduced antibiotic use for AURI in primary care settings without affecting patient-reported outcomes, including recovery from and duration of illness.27 The use of another inflammatory marker, procalcitonin, has been investigated in a few primary care studies. The studies showed a reduction in the prescribing of antibiotics when procalcitonin-guided therapy was used, without significant effects on safety.28,29 However, the use of procalcitonin in the primary care setting is limited due to a lack of feasible POC tests. Further clinical implementation studies on POC C-reactive protein tests should be conducted in Singapore to assess for the acceptability of the tests in clinical practice and the effectiveness in improving antibiotic prescribing practices.
It was found that GPs’ desire to improve on prescribing practices (Factor 6) was associated with low antibiotic prescribing (aOR 1.5 [95% CI = 1.2 to 1.9]) Most GPs were keen to take part in education programmes aimed at reducing antibiotic use. The majority (301 of 427; 70.5%) would like to have national clinical practice guidelines on the use of antibiotics in AURI. However, only about half (46.3%) expressed that such guidelines would change their prescribing practices. Further qualitative studies are required to understand the perception of GPs on the usefulness of guidelines and the preferred form of the guidelines to support their antibiotic prescribing practices.
GPs’ perceived patient expectation of receiving antibiotics (Factor 3) was often cited as a reason for antibiotic prescribing by primary care providers. In the current study, however, the perceived patient expectation was not a significant factor associated with antibiotic prescribing. This could be due to a lower level of health literacy in people in Singapore, who were less likely to discuss clinical management decisions with their healthcare providers. In previous studies in Western and Asian populations, patients have been observed to have a variable knowledge about the role of antibiotics in the common cold and cough,30,31 and those with a suboptimal knowledge of antibiotics tended to request antibiotics from their GPs. Patients who requested antibiotics were more likely to have them prescribed.30,32 Perceived patient expectation of receiving antibiotics causes inappropriate prescribing as GPs attempt to pre-empt their patients’ wishes. Unfortunately, these perceptions were often inaccurate.33 In a study conducted in emergency departments, physicians were more likely to prescribe antibiotics to patients they believed expected to receive them but they only correctly identified one in four such patients.34 Another reason why this study did not observe an association between perceived patient expectation and antibiotic prescribing may be that the more patriarchal doctor–patient relationships in Singapore result in fewer patient requests to doctors. In a study of doctor–patient relationships in Singapore, doctors believed that many of their patients were incapable of rational decision making, reflecting the elitism of the educated class, which is held in high regard in Asian societies.35 In a study among local medical students, there was a lower propensity for Singapore students to view the doctor–patient relationship as a partnership compared with students in the US.36 With an increasingly educated and assertive population in Singapore, GPs might progressively tailor their prescribing practices to satisfy their patients. A recent study in the UK reported that high antibiotic prescribing volume was a significant positive predictor of all ‘doctor satisfaction’ and ‘practice satisfaction’ scores, and was the strongest predictor of overall satisfaction out of 13 prescribing variables.37
Implications for research and practice
To the authors’ knowledge, this is the first KAP survey on antibiotic prescribing for AURI in primary care in Singapore. Interventions addressing these factors, including a tailored educational programme and national antibiotic guidelines, could improve antibiotic prescribing practices and reduce unnecessary antibiotic use in primary care settings. Future research directed at patient factors influencing antibiotic use will help in designing these educational programmes in the bid to reduce antibiotic use in the community.
Appendix 1. Knowledge, attitudes, and practices survey and variable types
| Variable list | Type of variable |
|---|---|
| Where is your current place of medical practice? | Categorical (3 levels) |
| How long ago did you graduate from medical school? | Categorical (3 levels) |
| Where did you attend medical school? | Binary |
| What is your highest medical qualification? | Categorical (4 levels) |
| What percentage of AURI are caused by viruses? | Scale (1–5) |
| What is the proportion of patients with AURI to whom you prescribe antibiotics? | Scale (1–5) |
| Q1) Symptoms of AURI cannot be relieved faster by antibiotics | Scale (1–5) |
| Q2) I am less comfortable giving antibiotics to patients with AURI than giving them | Scale (1–5) |
| Q3) I think antibiotics are overprescribed in primary care | Scale (1–5) |
| Q4) I do not find it difficult to determine whether antibiotics are needed for my patients with AURI | Scale (1–5) |
| Q5) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried that I will miss a bacterial infection | Scale (1–5) |
| Q6) I do not prescribe antibiotics if I don’t think the patient needs them because the risk of giving antibiotics is not low | Scale (1–5) |
| Q7) I do not prescribe antibiotics if I don’t think the patient needs them because I am not worried about the risk of bacterial complications from a viral AURI | Scale (1–5) |
| Q8) I am more likely to give antibiotics to patients with AURI if they are at the extremes of age (that is, in the paediatric or geriatric age groups) | Scale (1–5) |
| Q9) I am more likely to give antibiotics if the patient has comorbidities (for example, diabetes mellitus, COPD, chronic renal disease) | Scale (1–5) |
| Q10) I am more likely to give antibiotics if the patient returns for a repeat visit for the same respiratory condition | Scale (1–5) |
| Q11) I am more likely to give antibiotics if the patient has more than 3 days of respiratory symptoms | Scale (1–5) |
| Q12) If I do not prescribe antibiotics to my patients with AURI, they will usually ask for them | Scale (1–4) |
| Q13) I prescribe antibiotics even if I don’t think the patient needs them because I think the patient expects it | Scale (1–5) |
| Q14) I prescribe antibiotics even if I don’t think the patient needs them because otherwise the patient will then seek medical attention elsewhere | Scale (1–5) |
| Q15) If I don’t think my patient needs antibiotics, I will not prescribe them | Scale (1–4) |
| Q16) If a patient who does not need antibiotics asks for them, I will explain to them why I think they do not need them | Scale (1–4) |
| Q17) I am able to convince my patients who do not need antibiotics that they will not benefit from them | Scale (1–4) |
| Q18) I think I prescribe antibiotics appropriately | Scale (1–5) |
| Q19) To diagnose pneumonia, in addition to physical examination I routinely do further investigations (for example, FBC, CXR) | Scale (1–5) |
| Q20) If I am uncertain whether an AURI is of viral or bacterial origin, I depend on diagnostic tests (for example, FBC, CRP, throat culture) | Scale (1–5) |
| Q21) The turnaround time for diagnostic tests for AURI is not too long to be useful in my practice | Scale (1–5) |
| Q22) I hope the Ministry of Health will publish a clinical practice guideline on the use of antibiotics in AURI | Scale (1–5) |
| Q23) A national guideline would change my antibiotic prescribing pattern | Scale (1–5) |
| Q24) I would be keen to take part in an education programme aimed at reducing antibiotic prescription in primary care | Scale (1–5) |
AURI = acute upper respiratory tract infections. COPD = chronic obstructive pulmonary disease. CRP = C-reactive protein. CXR = chest X-ray. FBC = full blood count.
Questions were either on a 4-point (1 = never, 2 = infrequently, 3 = frequently, 4 = always) or a 5-point Likert scale (range from 1 = strongly disagree to 5 = strongly agree).
Appendix

Scree plot of number of factors and the eigenvalues. Factor 1 = medical knowledge and clinical competency; Factor 2 = conservative practice; Factor 3 = GPs’ perceived patient expectations; Factor 4 = good clinical practice; Factor 5 = availability of diagnostic tests; Factor 6 = desire to improve clinical practice — this was also moderately correlated with perceived patient expectations (r = 0.42).
Notes
Funding
There was no funding for this study.
Ethical approval
This study was approved by the Domain Specific Review Board, National Healthcare Group (Singapore) (approval number: 2012/01190).
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 16, 2016.
- Revision requested August 28, 2016.
- Accepted September 30, 2016.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

