


Abstract
Background Comorbidity is common in heart failure, but previous prevalence estimates have been based on a limited number of conditions using mainly non-primary care data sources.
Aim To compare prevalence rates of comorbidity and polypharmacy in those with and without chronic heart failure due to left ventricular systolic dysfunction (LVSD).
Design and setting A cross-sectional study of 1.4 million patients in primary care in Scotland.
Method Data on the presence of LVSD, 31 other physical, and seven mental health comorbidities, and prescriptions were extracted from a database of 1 424 378 adults. Comorbidity prevalence was compared in patients with and without LVSD, standardised by age, sex, and deprivation. Pharmacology data were also compared between the two groups.
Results There were 17 285 patients (1.2%) who had a diagnosis of LVSD. Compared with standardised controls, the LVSD group had greater comorbidity, with the biggest difference found for seven or more conditions (odds ratio [OR] 4.10; 95% confidence interval (CI] = 3.90 to 4.32). Twenty-five physical conditions and six mental health conditions were significantly more prevalent in those with LVSD relative to standardised controls. Polypharmacy was higher in the LVSD group compared with controls, with the biggest difference found for ≥11 repeat prescriptions (OR 4.81; 95% CI = 4.60 to 5.04). However, these differences in polypharmacy were attenuated after controlling for the number of morbidities, indicating that much of the additional prescribing was accounted for by multimorbidity rather than LVSD per se.
Conclusion Extreme comorbidity and polypharmacy is significantly more common in patients with chronic heart failure due to LVSD. The efficient management of such complexity requires the integration of general and specialist expertise.
INTRODUCTION
Chronic heart failure constitutes a major public health problem.1,2 The prevalence of chronic heart failure is increasing3,4 and, despite improvements in mortality,5 approximately 50% of those diagnosed die within 5 years.6 Chronic heart failure also impacts on quality of life,7 increases ‘treatment burden’,8,9 and presents challenging self-care demands.10
Patients with chronic disease often have multiple conditions.11 More than half of all hospitalisations of patients with heart failure are related to non-cardiovascular causes.12 Comorbidity is common in heart failure,13–15 especially in older patients.16,17 Comorbidities in heart failure increase mortality and resource utilisation,18–20 and lead to a deterioration in self-care.21
However, much of this evidence on comorbidity in heart failure comes from studies of hospital discharge records, studies considering a relatively limited number of chronic conditions, or studies with relatively small sample sizes.22,23 Data from primary care — the location of most healthcare interactions with patients with heart failure — are scarce. The aim of the present study was to examine the prevalence of convergent and divergent comorbidity in chronic heart failure using a large, nationally representative cross-sectional UK primary care dataset. Polypharmacy was also examined because of the potential on adherence, drug–drug interactions, and drug–tissue interactions.
METHOD
This study used data from the Primary Care Clinical Informatics Unit at the University of Aberdeen on 1 424 378 individuals, aged ≥18 years, who were alive and permanently registered with 314 general practices (31% of all practices in Scotland), or registered with a participating practice on 31 March 2007. These practices had recorded routine electronic clinical data as part of the Scottish Programme for Improving Clinical Effectiveness in Primary Care (SPICE-PC), which was a voluntary scheme run by the Scottish Government, and was a nationally representative sample in terms of patients’ age, sex, and socioeconomic status.24 Socioeconomic status was measured using the Carstairs score (grouped into quintiles). The dataset provided information on age, sex, socioeconomic status and 39 long-term conditions. In total, 18 899 individuals were identified as having heart failure through having a Read code for heart failure recorded in their primary care electronic medical record (EMR). Heart failure due to left ventricular systolic dysfunction (LVSD) is one of a number of chronic conditions whose accurate diagnosis and optimal management has been incentivised through the UK Quality and Outcomes Framework (QOF) pay-for-performance programme since 2004. There were 2622 individuals defined as having heart failure without LVSD or had missing data, and these were excluded from the study. The analysis was restricted to 17 285 individuals who had been diagnosed with heart failure due to LVSD and who were identified using QOF indicator heart failure 03.25 The control group was defined as the entire population of adults without LVSD (n = 1 404 471 individuals).
How this fits in
Comorbidity is known to be a common problem in patients with heart failure, but previous studies have been based on a small number of comorbid conditions using mainly non-primary care data sources. The current study compared prevalence rates of comorbidity in those with and without chronic heart failure due to left ventricular systolic dysfunction (LVSD) using nationally representative primary care data from a large dataset of primary care patients in Scotland. Compared with standardised controls, the LVSD group had elevated comorbidity, with 25 out of 31 physical and six out of seven mental health conditions being significantly more common. Polypharmacy was found to be more common in the LVSD group.
To control for differences between the two populations in age, sex, and deprivation levels, a similar approach to that undertaken in previous studies26,27 was adopted, and generated standardised prevalence rates by age groups (18–24; 25–34; 35–44; 45–54; 55–64; 65–74; 75–84; and ≥85 years), sex, and deprivation quintile using the direct method. These age–sex–deprivation standardised rates were then used to calculate odds ratios (ORs) and 95% confidence intervals (95% CI) for those with LVSD compared with those without (controls) for the prevalence of 31 physical conditions. Seven mental health conditions were also compared:
anxiety and stress related (including other neurotic, stress-related, and somatoform disorders;
alcohol problems;
depression;
learning disability;
dementia;
schizophrenia and bipolar disorder (and related conditions); and
anorexia or bulimia.
For all statistical analyses, a P-value <0.05 was considered statistically significant. All analyses were performed in Stata (version 13).
RESULTS
Demographics
There were 17 285 patients (1.2% of the sample) with a Read code for LVSD (Table 1). Males were over-represented in the LVSD group compared with (unadjusted) controls (53.5% versus 49.1% for controls; P<0.001). Individuals with LVSD were on average older (mean age 72.3 years versus 47.6 years for controls; P<0.001). Patients with LVSD were marginally more likely to be living in the most deprived areas when compared with unadjusted controls (LVSD most deprived quintile 20% versus controls 17.8%; P<0.001).
Age, sex, and deprivation status, LVSD versus controls for patients in primary care
Comorbidity: LVSD compared with standardised controls
After standardising for age, sex, and social deprivation (Table 2), higher levels of comorbidity were evident in the LVSD group, who were less likely to have none, one, or two conditions (LVSD 3.2% versus controls 52.0%, OR 0.90; CI = 0.10 to 0.80, LVSD 10.6% versus controls 21.4%, OR 0.47; CI = 0.45 to 0.50, and LVSD 14.8% versus controls 11.5%, OR 0.77; CI = 0.73 to 0.81 respectively). The LVSD group was more likely to have three conditions (LVSD 17.5% versus controls 6.8%, OR 1.22; 95% CI = 1.77 to 1.88). The biggest difference found was for seven or more conditions (LVSD 13.9% versus controls 1.1%, OR 4.10; 95% CI = 3.90 to 4.32). A similar, though even more striking, pattern was found when restricting analysis to physical health comorbidities (Table 2) with a five-fold difference between LVSD and controls being found in those with seven or more conditions (LVSD 9.1% versus controls 0.5%, OR 5.10; 95% CI = 4.79 to 5.43). Mental comorbidity was also more common in those with LVSD who were less likely to have no mental condition (LVSD 71.9% versus controls 84.9%, OR 0.67; 95% CI = 0.65 to 0.70) and were more likely to have one, two, three, or more mental health conditions ranging from OR 1.41; 95% CI = 1.36 to 1.47 (LVSD 20.3% versus controls 11.5%) for one condition to OR 1.39; 95% CI = 1.19 to 1.61 (LVSD 1.2% versus controls 0.5%) for three or more mental health conditions (Table 2).
LVSD status and number of morbidities for patients in primary care
Physical health individual conditions: LVSD compared with controls
For the LVSD group, 25 (including all six concordant conditions) out of 31 physical conditions were significantly more prevalent relative to controls (Figure 1). The largest differences after standardisation for age, sex and deprivation were for ‘concordant’ conditions; coronary heart disease (CHD) (OR 7.98; 95% CI = 7.72 to 8.25) atrial fibrillation (OR 6.84; 95% CI = 6.57 to 7.12) and chronic kidney disease (CKD) (OR 3.81; 95% CI = 3.60 to 4.04. However, large differences were also found for non-cardiometabolic conditions such as chronic pain (OR 3.01; 95% CI = 2.90 to 3.12) and chronic obstructive pulmonary diseases (COPD) (OR 2.65; 95% CI = 2.38 to 2.51).
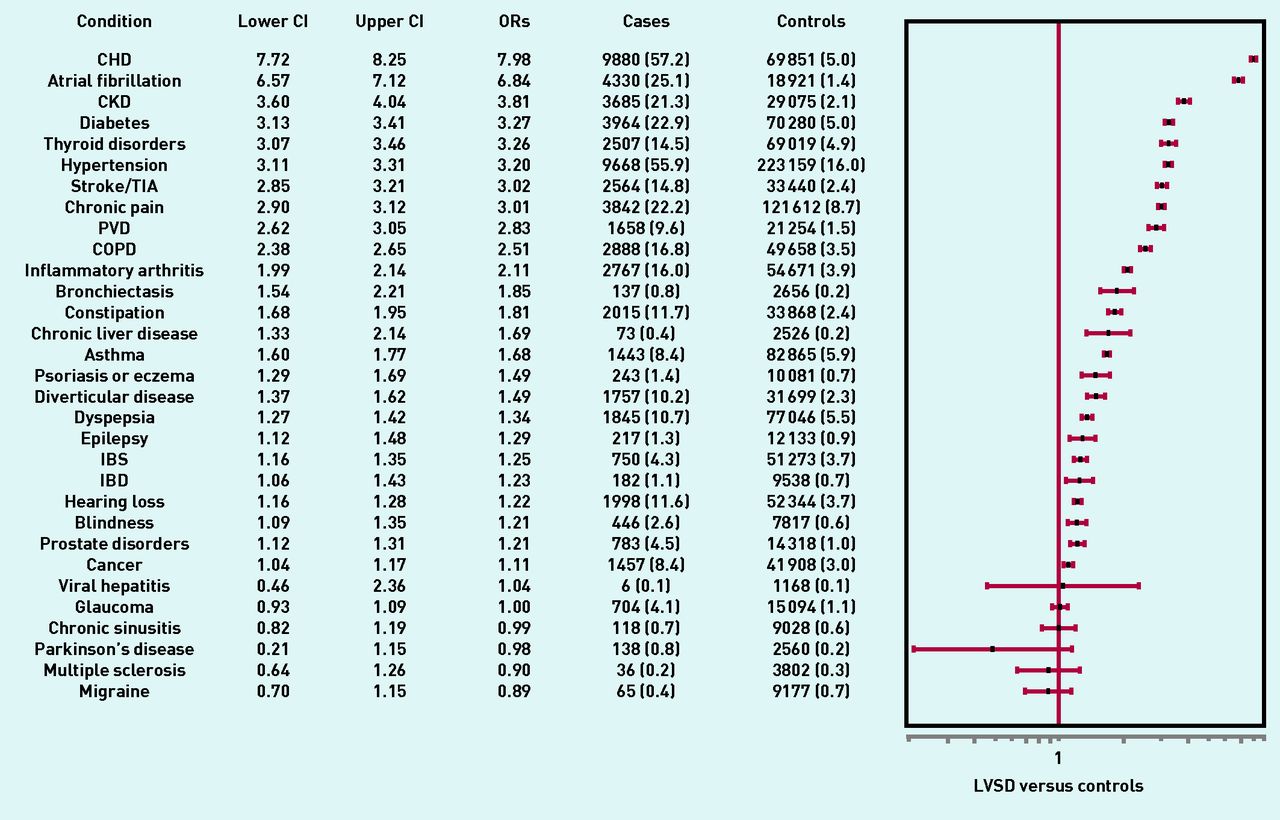
Prevalence and odds ratios for individual physical conditions for patients in primary care (standardised by age, sex, and deprivation score). CHD = coronary heart disease. CI = confidence interval. CKD = chronic kidney disease.
COPD = chronic obstructive pulmonary disease. IBD = inflammatory bowel disease. IBS = irritable bowel syndrome. PVD = peripheral vascular disease. TIA = transient ischaemic attack.
Mental health conditions: LVSD compared with controls
Table 3 highlights that those with LVSD had a significantly higher prevalence of six of the mental health conditions, with no difference found for anorexia/bulimia. The biggest difference after standardisation for age, sex, and deprivation was for anxiety and stress-related conditions (LVSD 11.0% versus controls 3.8%, OR 1.83; 95% CI = 1.73 to 1.94), followed by alcohol problems (LVSD 4.9% versus controls 3.0%, OR 1.73; 95% CI = 1.62 to 1.86). The highest prevalence for a mental health condition was found for depression with prevalence 16.3% for those with LVSD compared with 10.1% of controls (OR 1.52; 95% CI = 1.43 to 1.56).
Prevalence and odds ratios for individual mental conditions for patients in primary care (standardised by age, sex, and deprivation score)
Polypharmacy: LVSD compared with controls
Polypharmacy (defined as five or more repeat drugs) was substantially higher in the LVSD group compared with controls even after standardisation for age, sex, and deprivation (Table 4). However, these differences were substantially attenuated after additional standardisation to account for the number of morbidities, indicating that much of the additional prescribing was accounted for by comorbidity rather than LVSD per se (Figure 2).
LVSD status and number of repeat medications for patients in primary carea

{kind=link}
{kind=link}
Mean number of repeat prescriptions by number of morbidities in patients with LVSD and controls for patients in primary care. LVSD = left ventricular systolic dysfunction.
DISCUSSION
Summary
This analysis has found that comorbidity of physical and mental health chronic conditions are more common in those with LVSD even after standardisation for age, sex, and deprivation. The current study has provided a comprehensive picture of current patterns of comorbidity in primary care in those with chronic heart failure due to LVSD. Comorbidity is clearly the norm in LVSD, as is polypharmacy. Clinical guidelines and healthcare services need to put greater emphasis on the management of such complexity in LVSD, which will require the application and integration of general and specialist expertise.
Strengths and limitations
The strengths of this study were that a large nationally representative primary care database was used and LVSD was adopted as a measure for heart failure prevalence. The percentage of heart failure due to LVSD of 91.5% is similar to that found for all Scottish practices recorded in the QOF in the same year (2017), which was 88.7%.28 A limitation is that no data were recorded on the number of those with LVSD who had been identified using an echocardiogram even though heart failure is routinely investigated in NHS Scotland using an echocardiogram. The study was cross-sectional and there were no data on outcomes (such as mortality, quality of life, and health service utilisation).
Comparison with existing literature
In addition to LVSD, 39 morbidities were included, which is substantially more than most other studies of comorbidity and LVSD.
Direct comparison of the current study with existing literature is difficult as most previous studies focused on older patients, included a smaller number of conditions, did not have control groups, and had not been primary care based. However, the markedly higher prevalence of comorbidity in heart failure is consistent across studies, as is the finding of high levels of ‘concordant’ conditions such as CHD, CKD, and atrial fibrillation. The high level of chronic pain in the LVSD group in the present study appears to be a novel finding, which is worthy of further investigation.
It is possible that the higher level of comorbidities in LVSD, in part, reflects higher rates of diagnosis, because these patients would be invited for annual review under QOF. Similarly, the higher levels of polypharmacy could also relate to this and the fact that QOF recommends placing patients with LVSD on at least two drugs (ACEi/ARB and β-blocker).
Implications for research
Recent heart failure clinical guidelines acknowledge the issue of comorbidity but do not address the specific challenges.29,30 The evidence underpinning recommendations in LVSD guidelines is largely created from randomised controlled trials that exclude older patients and individuals with more comorbidity.31,32 Many evidence gaps remain in the clinical management of comorbidity in LVSD. For example, the safety and efficacy of many treatments for comorbidities, in the context of LVSD, as well as of the multiple drugs recommended for LVSD remain uncertain and more research in this area is required.
Acknowledgments
The authors thank the team at the Primary Care Clinical Informatics Unit at the University of Aberdeen, which provided the data, especially those individuals who completed the initial data extraction and management.
Notes
Funding
The corresponding author’s post and the development of the Applied Research Programme was part-supported by the Chief Scientist Office of the Scottish Government Health Directorates (Applied Research Programme Grant ARPG/07/1); the Scottish School of Primary Care.
Ethical approval
The NHS Grampian and National Research Ethics Services had previously approved the anonymous use of these data for research purposes, therefore this study did not need individual ethics approval.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received October 24, 2016.
- Revision requested November 17, 2016.
- Accepted December 13, 2016.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

