


Abstract
Background Polypharmacy (≥5 medications) is common in older patients and is associated with adverse outcomes. Patients’ beliefs about medication can influence their expectations for medication, adherence, and willingness to deprescribe. Few studies have examined beliefs about prescribed medication among older patients with polypharmacy in primary care.
Aim To explore medication-related beliefs in older patients with polypharmacy and factors that might influence beliefs.
Design and setting A mixed methods study utilising data from a randomised controlled trial aiming to decrease potentially inappropriate prescribing in older patients (≥70 years) in Ireland.
Method Beliefs were assessed quantitatively and qualitatively. Participants completed the Beliefs about Medicines Questionnaire by indicating their degree of agreement with individual statements about medicines on a 5-point Likert scale. Semi-structured qualitative interviews were conducted with a purposive sample of participants. Interviews were transcribed verbatim and a thematic analysis conducted. Quantitative and qualitative data were analysed separately and triangulated during the interpretation stage.
Results In total, 196 patients were included (mean age 76.7 years, SD 4.9, 54% male), with a mean of 9.5 (SD 4.1) medications per patient. The majority (96.3%) believed strongly in the necessity of their medication, while 33.9% reported strong concerns. Qualitative data confirmed these coexisting positive and negative attitudes to medications and suggested the importance of patients’ trust in GPs in establishing positive beliefs and potential willingness to deprescribe.
Conclusion Participants reported strong beliefs in medications with coexisting positive and negative attitudes. The doctor–patient relationship may have influenced beliefs and attitudes towards medicines, highlighting the importance of strong doctor–patient relationships, which need to be considered in the context of deprescribing.
INTRODUCTION
Polypharmacy (prescribing of many drugs [appropriately] or too many drugs [inappropriately]) is common in older patients.1,2 The prevalence of polypharmacy (≥5 medications) increased from 17.8% in 1997 to 60.4% in 2012 in persons aged ≥65 years in Ireland, and doubled to 20.8% between 1995 and 2010 in Scotland.3,4 Polypharmacy is associated with adverse drug reactions, poor medication adherence, geriatric syndromes (for example, urinary incontinence), potentially inappropriate prescribing (medications where their risks outweigh the benefits and when a safer alternative is available) and increased drug expenditure.5–8 Consequently, there has been an increased emphasis on deprescribing (process of medication cessation) and interventions to improve the appropriate use of polypharmacy such as medication reviews delivered by clinical pharmacists.9
Patients’ beliefs about treatment are an important influence on prescription medication use. Patients may influence prescribing decisions on the basis of their expectations or reluctance to take medicines in some cases. Patients’ strong beliefs in medicines, expectations, and resistance to change are often cited as important barriers to deprescribing inappropriate medication in older adults by GPs.10–13 Patient belief may also influence medication adherence (taking medications as prescribed). Several studies across a wide variety of conditions have highlighted that people with strong beliefs (as measured by the Beliefs about Medicines Questionnaire [BMQ])14 in the necessity of taking medication to maintain their health are more adherent to medications than those with higher levels of concern about medication.15,16 However, the majority of these studies have involved one group of medicines or specific illness groups, while comparatively few studies have examined beliefs about prescribed medication among older patients with polypharmacy in primary care. Considering the important role beliefs may play in medication use, it is important to explore the beliefs of patients with polypharmacy.
The aim of this study was to explore patients’ beliefs about and attitudes towards medication, within a population of community-dwelling older patients with polypharmacy, and explore factors that might influence medication beliefs.
METHOD
Study design
A convergent parallel mixed methods design was adopted.17 Secondary analysis of available quantitative and qualitative data was conducted separately (described below), and the findings triangulated during the interpretation stage.17,18 Although quantitative and qualitative data were available on the majority of cases, a mixed methods matrix was not conducted due to missing data.18
How this fits in
Inappropriate polypharmacy in older patients imposes a significant burden and may lead to adverse drug events, poor adherence, and geriatric syndromes. Consequently, there has been an increased emphasis on deprescribing and interventions to improve the appropriate use of polypharmacy. Patients’ strong beliefs in medicines are often reported as important barriers to deprescribing by GPs. However, beliefs about medication in patients with polypharmacy have scarcely been investigated. Using qualitative and quantitative data, this study explored patients’ beliefs about and attitudes towards medication, within a population of community-dwelling older patients with polypharmacy. Study participants reported strong beliefs in medications with coexisting positive and negative attitudes. Doctor–patient trust may have influenced beliefs and attitudes towards medicines, highlighting the importance of strong doctor–patient relationships in the context of deprescribing.
Context and study setting
Data were obtained from OPTI-SCRIPT (OPTImizing PreSCRIbing for Older People in Primary Care), a pragmatic cluster randomised controlled trial conducted in Ireland (ISRCTN41694007). The trial involved 21 GP practices and 196 community-dwelling patients aged ≥70 years, with pre-existing potentially inappropriate prescribing.19 The study found that a multifaceted intervention (incorporating academic detailing and GP-led medicines review) was effective in reducing potentially inappropriate prescribing in the intervention group (see Appendix 1 and 2 for more detail).19–21 The present study uses cross-sectional data collected at baseline from all participants (May 2012 to February 2013), and qualitative data collected during the OPTI-SCRIPT process evaluation (January 2013 to August 2013).22
Quantitative data collection and analysis
Medication data
Medication data were collected through review of electronic or paper-based patient charts, depending on the practice system. The number of repeat medications per participant (n = 196) was recorded and classified according to the Anatomical Therapeutic Chemical (ATC) classification system of the World Health Organization (WHO). The prevalence of polypharmacy (≥5 regular medicines) and excessive polypharmacy (≥10 regular medicines) was calculated.3
Questionnaires
Demographic information and patients’ beliefs about medication were collected at baseline via postal questionnaire with telephone follow-up for non-responders. Participant beliefs were captured using the BMQ.14 The BMQ consists of a specific and a general part. The BMQ-Specific assesses patients’ beliefs about medication prescribed for them and comprises two scales assessing personal beliefs about the necessity of prescribed medication for controlling illness and concerns about the potential adverse consequences of medications. The necessity–concern differential acts as a cost–benefit analysis, where patients weigh up the concerns (costs) they have about medication against their perception of their necessity (benefit). It is scored −20 to 20, with positive results indicating that the patient perceives that the benefits outweigh the risks. The BMQ-General measures beliefs about medicines in general. Responders indicate their degree of agreement with each statement about medicines on a Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Scores obtained for the individual items within each scale are summed to give a scale score. Higher scores indicate stronger beliefs in the concepts represented by the scale.
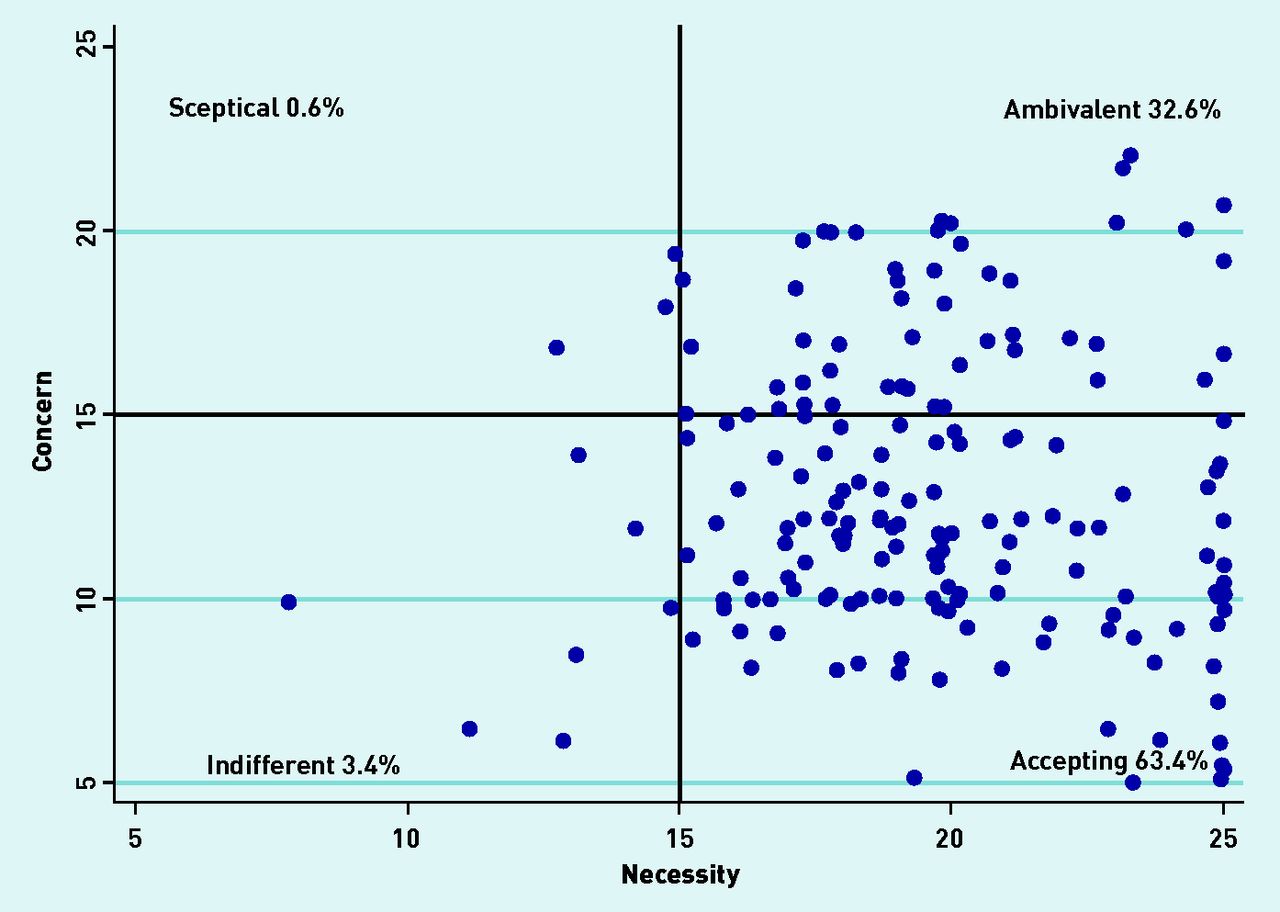
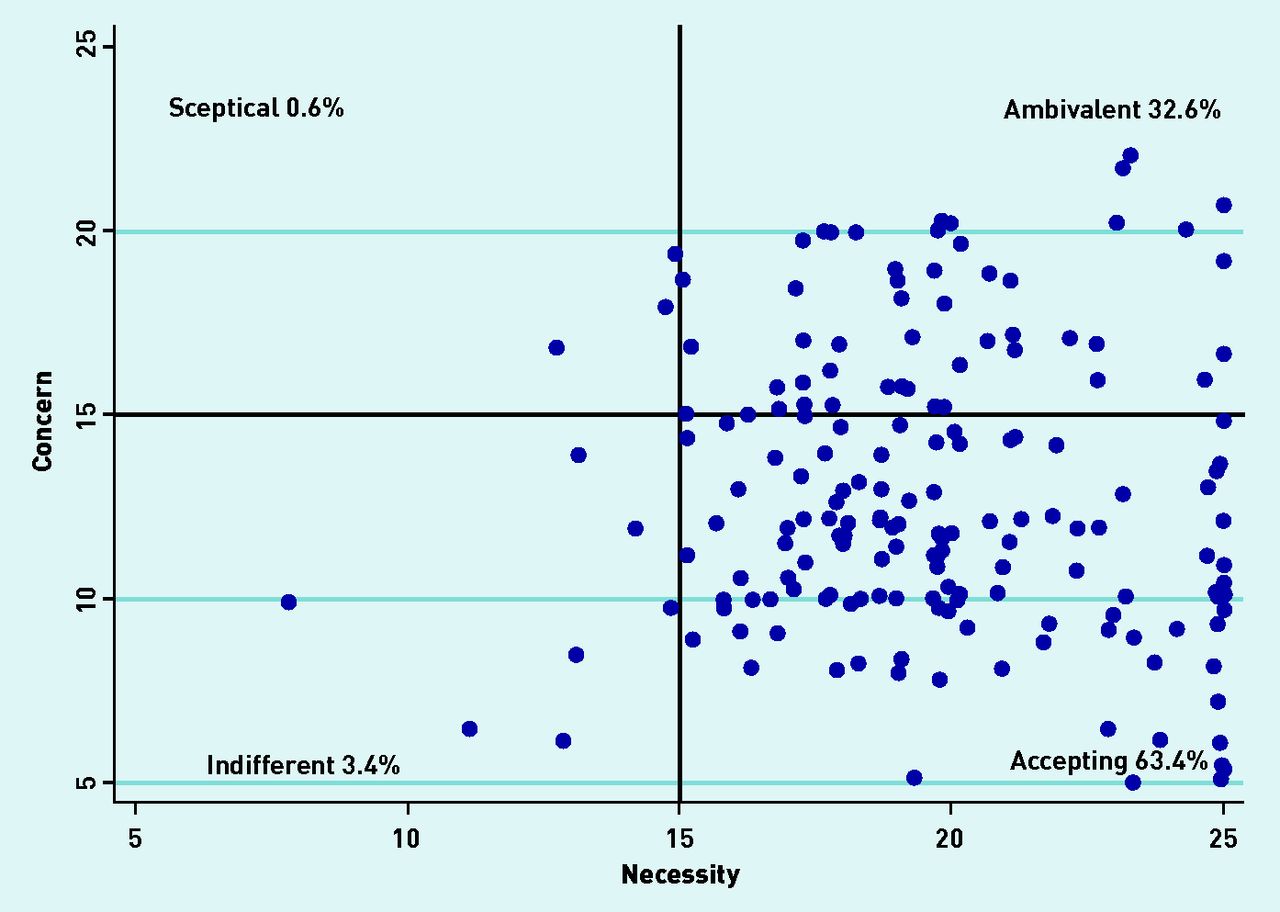
Participants were excluded if more than two items on the BMQ were missing. Mean and median scores for the four subscales, and the necessity–concerns differential, were calculated. The separate necessity and concern scales were divided at the scale midpoint to create four attitudinal groups, as used in previous studies:23
sceptical (low necessity, high concerns);
indifferent (low necessity, low concerns);
ambivalent (high necessity, high concerns); and
accepting (high necessity, low concerns).
Multivariable regression analyses adjusting for demographic factors were used to study associations between BMQ subscales and participant characteristics with the subscales as dependent variables. All analysis was conducted using Stata version 13.
Qualitative data collection and analysis
Qualitative data were collected from one-to-one semi-structured interviews with a purposive sample of participants in the intervention arm of the OPTI-SCRIPT study, to ensure coverage across GP practices, patient sex d, and types of medications. All interviews were conducted via telephone by one interviewer and were audio-recorded (on loudspeaker). The interview topic guide (Appendix 3) covered aspects of the trial evaluation, and the following two broad sections were pertinent to this current study: participants’ perceptions of their medications and experiences of GP consultations (Box 1).
Broad prescribing-related interview questions
Could you tell me a little about your medications?
Prompts: What do you take? How many medicines? Are your medicines important/necessary? Why do you take them? Are there any side effects?
Could you tell me how you feel about taking these medications?
Prompts: How does having to take your medicines impact on you?
Could you tell me a little about your interactions with your GP?
Prompts: How often do you see them? What do you discuss about your medications? What type of information about your medications do you get?
All interviews were transcribed verbatim by one interviewer and analysed using a thematic analysis following a six-step process.24 Two researchers independently reviewed the individual transcripts several times to familiarise themselves with the data. Small sections of data were assigned a code that summarised the content. Codes with common features were grouped together in emerging themes, before finally being assigned to overarching themes.24 Quotations were used as exemplars of key themes. NVivo 10 was used to assist with organising the data for analysis. All participant data were pseudo-anonymised by assignment of a unique study ID.
RESULTS
Characteristics of participants
Of the 196 participants aged ≥70 years in the OPTI-SCRIPT study, 54% were male and the mean age was 76.7 (SD 4.9) years (Table 1). Recruited patients were demographically similar to the general population of those aged ≥70 in Ireland (Appendix 2). A total of 1862 drugs were recorded with a mean of 9.5 (SD 4.1) per person. Just under half (46%) of participants had excessive polypharmacy (≥10 medicines). Cardiovascular medication was the most frequently prescribed medication category (26.9%), the majority of which were statins, followed by drugs for the alimentary tract and metabolism (18.2%) (Appendix 4).
Characteristics of study sample (n = 196)
Most participants (96.3%) believed in the necessity of their medication for maintaining health (that is, had scores greater than the scale midpoint). Overall, 33.9% reported concerns about potential adverse consequences of taking their medication (with scores greater than the scale midpoint). For the vast majority (94%), the difference between the necessity and concern scores was positive, indicating strong beliefs that the benefits of their medications outweighed the costs (Table 2). When participants were categorised by belief group, the majority were found to be either accepting (63.4%) or ambivalent (32.6%) towards their medication (Figure 1).
Patients’ beliefs about medicines
{kind=link}
Attitudinal analysis of patients’ beliefs about medicines (n = 175)
Most participants believed that medicines were generally beneficial. Only 3% indicated a high belief (with scores greater than the scale midpoint) that medicines were generally harmful and just over 5% had a high belief (with scores greater than the scale midpoint) that medicines were generally overused (Table 2).
Results from multivariate regression analysis with the four BMQ subscales as the dependent variables, adjusting for demographic factors (Table 3), demonstrated an increase in the number of repeat medications was significantly associated with an increased score on the necessity subscale (0.23, 95% CI = 0.11 to 0.35, P<0.01).
Linear regression analysis of beliefs about medicines subscales and number of repeat medications
Participant views on medication
From 14 patients approached, 11 participants were interviewed, 54% of whom were male, with a mean age of 77 years. Interviews ranged from 6.21 to 20.27 minutes (Table 1). Of the 11 participants, six (54.5%) were categorised as accepting, three (27.3%) were ambivalent, and two (18.2%) had insufficient data to calculate based on baseline BMQ. From the interview data, three main themes emerged: necessity and concern conflict, knowledge of medications, and relationships with healthcare providers.
Necessity and concern conflict
The majority of participants reported that they accepted medications that were necessary to ‘keep you ticking over’ (P655, female, 76 years) and ‘keeping the engine running’ (P161, male, 80 years). Some participants were however concerned about long-term medication use and potential adverse side effects, particularly for medications prescribed for prevention of future problems:
‘Well maybe, you know you read the leaflets, but I mean you read them and there is everything on it, you know, there could be side effects, and they just like have them a hundred and one, and you say to yourself, Oh my God. If you get them [medication] for blood pressure, they say they could cause your blood pressure to go up, they could cause heart attacks, you know all this. So you don’t know whether you are doing right or wrong having a particular medication, I don’t know.’
(P74, female, 72 years)
‘Well, there is one worry that you do have at the back of your mind, that when, I’m so long on the tablets, you know what I mean, and there might be something happening and I don’t know about it because I feel OK, but you don’t know.’
(P125, male, 75 years)
Medications prescribed for symptomatic relief were viewed as beneficial and more readily accepted, often despite potential side effects:
‘I should say, I didn’t take them [medication] one particular morning and didn’t take the tablet that night, but by God, I knew all about it the next day. I didn’t realise I really relied on those tablets as much as I am. And I’d say if I didn’t have those I don’t know where I would be.’
(P1315, male, 81 years)
‘COPD [chronic obstructive pulmonary disease] is a nuisance but you just have to take the old inhalers and that. I don’t like being on steroids. Recently, as you know I’ve osteoarthritis, and I was in recently getting injections in my back, for the pain in my back you know, and you know the little thing they put in your arm, to knock you out, that thing, it tore the skin, and just the eh, anaesthetist who was putting, he said “You must be on steroids”, it makes my skin very thin. So that’s the bad effect of the steroid, but then, if I need them to breath! Catch 22, isn’t it.’
(P655, female, 76 years)
Knowledge of medications
Participants reported variation in the level of knowledge about medications prescribed for them. Some participants were well informed and comfortable discussing their medications, whereas others expressed a lower level of understanding:
‘… coz we really don’t know what we are taking half the time …’
(P125, male, 75 years)
‘So the new tablet now, I don’t know the name of it, I do call them by the colours, I do be telling him, the pink one and the green one and the yellow one and the white one …’
(P639, male, 78 years)
Relationships with healthcare providers
The majority of participants described positive relationships with their GPs, citing satisfactory aspects of consultation style, including approachability, being listened to, and feeling comfortable:
‘I would say, I find that practice very approachable, both Dr X and Dr Y, they’re both, you can just speak to them you know, like a friend. Anything I’d have to say I could talk freely with them, you know, there is no kinda, doctor–patient where you are nearly afraid as we were years ago, there’s nothing like that, I feel very comfortable with them I suppose is the word.’
(P655, female, 76 years)
‘I always find it rewarding because he [GP] is a very knowledgeable man and he is very dedicated.’
(P1347, female, 84 years)
GPs who were perceived as supportive and engaged fostered a sense of trust, and participants were confident they would make the right treatment decisions, even where reviewing or stopping medications was concerned:
‘I trust Dr X, you know with anything she does, you know she only gives me something for a reason, she doesn’t just give me it for the sake of it, “Oh I’ll have to get rid of her” or something like that, no. She is very thorough and very conscientious.’
(P2338, female, 72 years)
‘Well I mean the doctor said it to me you know, “Oh I don’t like you taking Difene”, I say why, “Because it’s very hard on the stomach” you know, and I think it’s the kidneys or the liver or something, you know, I accept what they tell me. Well that’s what we go to the doctor for isn’t it — to be told what’s good for your body.’
(P655, female, 76 years)
‘I think that is what you would be looking for [review of medication], because nobody wants to take more medications than they need to.’
(P1345, male, 81 years)
Familiarity was a key element, with established relationships and positive past experiences increasing patient confidence:
‘I go with him [GP]. He’s been very good over the years and I’m always led by him. What he says I’ll take his word for it as right.’
(P125, male, 75 years)
‘I have a very good GP, Dr Y and he has a few assistants there, and eh, they’re all very attentive there I must say, all very very good and he’s available at all times, you know, all you do is lift the phone and you get an appointment.’
(P639, male, 78 years)
Some participants did express dissatisfaction about aspects of how medications were prescribed, in terms of information provided, particularly where hospital prescribing was concerned:
‘You see people of my age going in to the pharmacist and coming away with a big parcel of stuff, now I wouldn’t know, their general, whether they need all them things or not, but I would get the impression that they’re not keeping, you know, there is probably no need for a lot of the stuff that they’re taking you know.’
(P1616, male, 75 years)
‘I’m saying specifically if you go, you go to the hospital rather than your doctor, with something that needs to be done up in the hospital, they treat you, and they say well go on this, you know, do whatever, but they never tell you how long, and you stay on the thing then for, indefinitely like.’
(P74, female, 72 years)
Three interviewees spontaneously discussed the role of pharmacists in prescribing, reporting positive interactions, particularly citing helpful innovations the pharmacists provided such as pill boxes:
‘And I now I have got these things, they do it all in the chemist with these packs, it’s plastic like a tray, and it’s brilliant, and I’m quite happy with that.’
(P2338, female, 72 years)
DISCUSSION
Summary
Using a mixed methods approach, this study among older community-dwelling patients with polypharmacy highlighted that the majority believed in the necessity of their medication.
However, this belief was underscored by complex attitudes. Participants reported strong beliefs in medications with coexisting positive and negative attitudes. Furthermore, the doctor– patient relationship may influence beliefs and attitudes towards medicines and deprescribing.
Strengths and limitations
Combining qualitative and quantitative data allows a richer analysis. Participants completed questionnaires without a researcher present, which may have decreased responder bias. Despite contacting participants to obtain missing data, not all participants answered the BMQ in full.
This was taken into account in the analysis, but may have impacted on the results. The qualitative data is limited as it was obtained as part of a larger process evaluation of the OPTI-SCRIPT trial.
Consequently, the sample was limited to trial participants who may not be representative of all older patients, the topic guide was not designed to explore issues of polypharmacy specifically, and interviews were shorter on average (14 minutes) than may be expected. Although the themes presented here emerged strongly from the data, a more detailed interview arguably may have produced a more nuanced account. Overall, the results are consistent with limited previous qualitative studies in this area, increasing confidence in the findings.
Comparison with existing literature
Older patients with multimorbidity (presence of >1 chronic health condition)25 and polypharmacy may be critical of taking numerous medications and conceptualise this as a burden.26,27 Similar to a previous Swedish study,28 the majority of our participants (94%) had strong beliefs in their benefits, however, approximately one-third of participants had strong concerns. For the majority, belief in necessity outweighed any concerns, similar to patterns observed in a frail elderly population.29 This highlights the complexity of attitudes to prescription medication use, as people possess coexisting accounts of positive and negative attitudes to their medications.26,30 Patients may be grateful for the symptom relief provided, but many prescribed medications are used to extend life or for secondary prevention of disease. The qualitative findings highlighted that these medications were harder for patients to accept. Patients are expected to take these medications long term, often without experiencing any immediate tangible benefit, but being aware of the potential risk of adverse effects, thereby creating uncertainty about the total overall benefit.
Despite some patients potentially holding negative views towards medications, evidence suggests most patients adapt to long-term medication use.26,31,32 This current study’s patient population were primarily categorised as accepting of the necessity of taking medications (63%). The multivariable regression revealed that, as the number of medications increased, so did the score on the BMQ necessity subscale, indicating that, as this number increased, beliefs in the necessity became stronger. Patients described their medications as necessary to keep them ‘ticking over’, indicating a practical acceptance. At the same time, however, some participants reported poor knowledge of their medications, a common trait among patients taking multiple drugs, and older people in general tend to have poorer health literacy.28,33,34 This highlights the complex interplay of strong beliefs in the context of limited knowledge. Indeed, a previous study involving frail older patients found no relationship between strong beliefs and medication knowledge.29 Despite having concerns and reporting poor knowledge, the majority of the participants in this current study were accepting and reported a strong belief in the necessity of medications. One explanation for this paradoxical position may lie within the qualitative findings on the doctor–patient relationship — specifically trust.
Interpersonal trust (between patient and clinician) is a key element of the doctor– patient relationship, one particularly valued by older patients.35–38 These current results highlight that, for patients with polypharmacy, medication taking is often characterised by uncertainty, elements of risk, and information asymmetry between patient and GP (that is, GPs have more information than patients, creating an imbalance of power). Trust is necessary in such conditions of uncertainty as it reduces complexity, allowing people to make decisions.39,40 In this context, trust in the GP may enable patients to negotiate the complexity and uncertainty of polypharmacy. Trust can influence patients’ attitudes towards medications, with patients likely to develop negative attitudes towards medications where their trust in a prescriber is negatively influenced.30,32,41
Along with lack of guidelines and the involvement of multiple prescribers, patients’ strong beliefs in medicines are often reported as important barriers to deprescribing by GPs.10,11 However, strong beliefs exist against a backdrop of positive and negative attitudes. The participants in this current study had strong beliefs in medicine, yet also expressed willingness to trial stopping medications, similar to other cohorts.42 This willingness may arise from interpersonal trust, because evidence suggests that patients report willingness to trial the cessation of medications when recommended by a physician they trust.13
Implications for research and practice
In light of the increased prevalence of polypharmacy and associated adverse consequences, it is imperative to develop effective interventions to improve appropriate polypharmacy and patient outcomes.9,16 Increasingly, there is a focus on deprescribing, with recent reviews stressing the importance of shared decision making.43,44 Patients’ strong beliefs in medicines are often reported as important barriers to deprescribing by GPs.10,11 However, the findings highlight that strong beliefs often mask a complex interplay of positive and negative attitudes, in the context of limited knowledge and a willingness to stop medications. Patients’ beliefs and attitudes about medications may be influenced by the doctor–patient relationship. Patient trust may facilitate a willingness to tolerate polypharmacy in a context of uncertainty, but it may equally influence patients’ willingness to deprescribe. This study provides evidence to support GPs building strong relationships with patients with complex multimorbidity and polypharmacy to enhance deprescribing.41 Practical strategies to achieve this include active identification of complex patients, and the adoption of a policy of continuity of care such as assigning these patients a named doctor.25 Strategies that improve continuity of care may also reduce secondary care costs, particularly for the heaviest users of health care.45
Acknowledgments
The authors gratefully acknowledge the time provided by the GP practices and the patients who participated in the OPTI-SCRIPT study.
Appendix 1. Overview of the OPTI-SCRIPT cluster RCT methods and findings
| Aim | To test the effectiveness of a multifaceted intervention in reducing the level of PIP in primary care. |
| Recruitment | GP practices from the Health Research Board Centre for Primary Care Research network were invited to participate by e-mail with a follow-up telephone call. Practices were eligible if they had at least 80 patients aged ≥70 years and were based in the greater Dublin area. |
| Participants | 21 general practices (intervention n = 11, control n = 10). 196 patients ≥70 years (intervention n = 99, control group n = 97) with ≥1 PIP drugs. |
| Outcome measure | Proportion of participant patients with PIP and the mean number of potentially inappropriate prescriptions per group. |
| Intervention group | The intervention consisted of:
|
| Control group | Control practices delivered usual care. Usual care for public GMS patients allows GPs to give a prescription on a monthly or 3-monthly basis. Control practices received simple patient-level PIP feedback in the form of a list summarising the medication class to which the individual patient’s potentially inappropriate medication belonged. Control practices did not receive an academic detailing visit or were not prompted to carry out medicines review with the individual patients. |
| Results | Upon intervention completion:
|
GMS = general medical services. OR = odds ratio. PIP = potentially inappropriate prescribing. RCT = randomised controlled trial.
Appendix 2. Comparison of OPTI-SCRIPT participating practices and patients with national populations
| Characteristic | Study participants n (%) | National population % |
|---|---|---|
| GP practice | ||
| Practice type | ||
| GMS and private | 100 | 96.0a |
| GMS list size | ||
| ≤500 | 14.3 | 29.8b |
| 501–1500 | 23.8 | 59.6b |
| 1501–2500 | 61.9 | 10.6b |
| Practice staff | ||
| Single-handed GP | 14.3 | 35.0a |
| ≥2 GPs | 85.7 | 65.0a |
| Practice manager | 71.4 | 30.0a |
| Practice location | ||
| Urban | 76.2 | 43.0a |
| Mixed | 23.8 | 36.0a |
| Teaching activity | 100 | 42.0a |
| Patients | ||
| Total population | ||
| Male | 105 (53.6) | 157 016 (43.4)c |
| Age category, years | ||
| 70–75 | 95 (48.5) | 154 286 (42.6)c |
| 76–80 | 58 (29.6) | 95 894 (26.5)c |
| 81–85 | 35 (17.9) | 63 406 (17.5)c |
| 86–90 | 6 (3.1) | 34 358 (9.5)c |
| ≥91 | 2 (1.0) | 13 811 (3.8)c |
| Marital status | ||
| Married/cohabiting | 108 (55.1) | 170 560 (47.1)c |
| Widowed | 58 (29.6) | 125 551(34.7)c |
| Single | 24 (12.2) | 55 371 (15.3)c |
| Divorced | 3 (1.6) | 3767 (1.0)c |
| Separated | 2 (1.0) | 6506 (1.8)c |
| Unknown | 1 (0.5) | – |
| GMS card holder | 183 (93.4) | 360 000 (96.0)b |
Appendix 3. Topic guide
Broad medication-related interview questions
Could you tell me a little about your medications?
Prompts: What do you take? How many medicines? Are your medicines important/necessary? Why do you take them? Are there any side effects?
Could you tell me how you feel about taking these medications?
Prompts: How does having to take your medicines impact on you?
Could you tell me a little about your interactions with your GP?
Prompts: How often do you see them? What do you discuss about your medications? What type of information about your medications do you get?
The intervention — you met with your GP to discuss some of your medications in a medicines review
Can you tell me how you found that experience?
○ Informative, beneficial, helpful/unhelpful, negative
Can you tell me more about why you feel that?
○ How did it differ from your general GP visits?
Get anything extra from it (PIL)?
— Yes — Was it useful/informative?
— No — Would you like something like this?
○ What was the outcome if you don’t mind discussing?
Did anything change (for example, stopped med, reduced dose)?
YES How do you feel about those changes — were they positive, what impact have they had on you/health/life?
Are you happy?
NO What was the reason for that? Your preference, hospital, no alternative?
Are you happy with the outcome generally?
Do you think having a review like this, maybe once or twice a year, would be useful?
○ To you, to others, etc.
Elements that may benefit from change
○ Was there anything you disliked/a process you would like to change?
How would you describe the experience of taking part in this study?
○ Positive, negative, useful, neutral, etc.
Effects of intervention overall?
○ In summary, given your experience of the review, is it something you would be happy to do again (hypothetically) if your GP asked? Would you like to see it become a routine thing?
Appendix 4.

Prescribed medication categories
Notes
Funding
This study was funded by the Health Research Board (HRB) PhD Scholars Programme in Health Services Research under Grant No. PHD/2007/16 and the HRB Centre for Primary Care Research under Grant No. HRC/2007/1, Royal College of Surgeons in Ireland (RCSI), Dublin, Ireland. The sponsors of the study had no role in the study design, data collection, data analysis, data interpretation, writing of the report, or in the decision to submit the paper.
Ethical approval
The Research Ethics Committee of the Irish College of General Practitioners (ICGP) approved this study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received January 12, 2017.
- Revision requested February 15, 2017.
- Accepted February 23, 2017.
- © British Journal of General Practice 2017
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

