


Abstract
Background Antibiotics are overprescribed for non-severe acute infections in children in primary care.
Aim To explore two different interventions that may reduce inappropriate antibiotic prescribing for non-severe acute infections.
Design and setting A cluster randomised, factorial controlled trial in primary care, in Flanders, Belgium.
Method Family physicians (FPs) enrolled children with non-severe acute infections into this study. The participants were allocated to one of four intervention groups according to whether the FPs performed: (1) a point-of-care C-reactive protein test (POC CRP); (2) a brief intervention to elicit parental concern combined with safety net advice (BISNA); (3) both POC CRP and BISNA; or (4) usual care (UC). Guidance on the interpretation of CRP was not provided. The main outcome was the immediate antibiotic prescribing rate. A mixed logistic regression was performed to analyse the data.
Results In this study 2227 non-severe acute infections in children were registered by 131 FPs. In comparison with UC, POC CRP did not influence antibiotic prescribing, (adjusted odds ratio [AOR] 1.01, 95% confidence interval [CI] = 0.57 to 1.79). BISNA increased antibiotic prescribing (AOR 2.04, 95% CI = 1.19 to 3.50). In combination with POC CRP, this increase disappeared.
Conclusion Systematic POC CRP testing without guidance is not an effective strategy to reduce antibiotic prescribing for non-severe acute infections in children in primary care. Eliciting parental concern and providing a safety net without POC CRP testing conversely increased antibiotic prescribing. FPs possibly need more training in handling parental concern without inappropriately prescribing antibiotics.
- children
- cluster randomised controlled trial
- inappropriate prescribing
- physician–patient communication
- point-of-care testing
- primary care
INTRODUCTION
Acute infection in children is a common reason for encounter in family practice. Most children suffer from non-severe conditions, though many of them are unnecessarily treated with antibiotics. This might lead to avoidable adverse effects and costs, and to the emergence of antibiotic resistance. Despite a recent decline, 38% of all Belgian children were given at least one antibiotic prescription in outpatient care during 2014.1 This number is more than twice as high as in the Netherlands (18%) and comparable with the annual antibiotic prescription rate in the UK (36%).2
Overprescribing can be caused by physicians’ diagnostic uncertainty, as distinguishing between viral and bacterial infections is clinically challenging and denying antibiotics to a child with a possible bacterial infection might feel inappropriate.3–6 More diagnostic certainty can be attained by applying clinical prediction rules intending to rule out serious infection in children.7–9 Moreover, new diagnostic tools, such as point-of-care C-reactive protein (POC CRP) tests, could further reduce uncertainty. Studies suggest that CRP levels <20 mg/L can rule out serious infection in febrile children in a hospital setting, but safe cut-off levels in the primary care setting, in which serious infections are rare, remain unknown.10 By reducing uncertainty, POC CRP could also reduce antibiotic prescribing, as shown in adults with respiratory tract infections.11,12 Also, having an observable test result to share might reassure patients that clinicians are making appropriate treatment decisions.13
Overprescribing can also be attributed to physicians’ failure to cope with parental concern. When physicians engage in reassuring worried parents too promptly, parents can feel misunderstood and restate their worries to get the physician’s attention. Physicians can misinterpret this as parental insistence for antibiotics, which may lead to inappropriate prescribing.14,15
In the present study, the effect of two interventions on antibiotic prescribing for acute non-severe infections in children were explored: reducing clinicians’ uncertainty with an objective inflammatory parameter (POC CRP test) or improving mutual understanding by both actively giving parents the opportunity to express their underlying concerns and providing safety net advice.
METHOD
Study design
A cluster randomised, factorial controlled trial (CRCT) was performed in children with an acute non-severe infection presenting to a family physician (FP). There were four intervention groups: (1) performing a POC CRP test; (2) applying a brief intervention to elicit parental concern combined with safety net advice (BISNA); (3) performing a POC CRP test plus applying BISNA; and (4) usual care (UC). Allocation was performed at practice level to avoid contamination. The allocation ratio was 1:1:1:1. Every cluster consisted of infectious episodes in children included by one physician.
How this fits in
It is known that antibiotics are prescribed too often for non-severe acute infections in children in primary care. Point-of-care CRP (POC CRP) testing and promoting shared decision-making reduce antibiotic prescribing for acute respiratory tract infections in adults, but the effect of such interventions in children remains unclear. This study found that systematic POC CRP testing without guidance is not an effective strategy to reduce antibiotic prescribing for non-severe acute infections in children in primary care. Eliciting parental concern and providing a safety net without POC CRP testing conversely increased antibiotic prescribing. Family physicians possibly need more training in handling parental concern without inappropriately prescribing antibiotics.
Study population
Participating family physicians
All FPs in Flanders, Belgium, stating that they were able and prepared to consecutively recruit at least five ill children during the inclusion period, were eligible to participate. Practices were assigned to the four intervention groups using stratified (by practice type) block randomisation (block size four).
Participating children
Children aged 1 month to 16 years presenting with an acute infection lasting a maximum of 5 days at the initial contact were consecutively included. Episodes at a high risk for serious infection were excluded post hoc, as antibiotic prescribing should not be restricted in these cases. These children were identified using a clinical decision rule (CDR) consisting of four clinical criteria: the gut feeling of the physician, presence of dyspnoea, temperature ≥40°C and diarrhoea in children aged between 1 year and 2.5 years.7 Children who were referred to a paediatrician were excluded. Other exclusion criteria were episodes caused by merely traumatic or neurological conditions, intoxication, psychiatric or behavioural problems, or an exacerbation of a known chronic condition. Written informed consent was solicited from the child’s accompanying parent or legal guardian.
Intervention
For the POC CRP test using an Afinion AS100 Analyzer, Alere, US, a finger prick test was performed and the result was available within 4 minutes.16 Guidance on the interpretation of CRP results was not provided because safe cut-off levels in primary care are unknown.17 The brief intervention consisted of the following three questions for parents at the start of the consultation: ‘Are you concerned [about the illness of your child]?’, ‘What exactly concerns you?’, and ‘Why does this concern you?’ Apart from these questions, a parent information leaflet containing information about supportive treatment (for example, what to do in case of fever, how to use antipyretics) and when to re-consult was provided as safety net advice. To avoid contamination between the intervention groups, only FPs in the BISNA intervention groups (allocation group 2 and 3) were informed about the specific content of the brief intervention.
Data collection
FPs registered child characteristics, clinical parameters, preliminary diagnosis, and treatment actions (or referral) on a registration form. Parents completed a diary until they assessed their child as recovered.
Endpoints
The main outcome measure was the immediate antibiotic prescribing rate. An immediate prescription is meant to be delivered and administered immediately after the consultation. Second, the total antibiotic prescribing rate was observed, by adding delayed prescriptions meant to be administered by the parent in certain circumstances, for example, in case of persistent or worsening complaints such as fever, cough, and pain, or in case of a prolonged or worsening general feeling of illness.
Sample size calculation
To detect an absolute reduction in antibiotic prescribing of 15% (from 40% to 25%), with 80% power at a 5% significance level, an individually randomised study would need 600 patients (150 patients per group and four groups). Assuming an intra-cluster correlation coefficient (ICC) of 0.15 (worst case) and a cluster size of 21, the design effect of the study is 4. Twenty-nine FPs per group (116 FPs in total) are thus needed.18
Statistical analysis
The analyses were performed with SPSS version 24. A crude and adjusted mixed logistic regression analysis was performed, considering the hierarchical structure of the data (practice level, FP level, patient level).
At practice level, region (urban/rural) and practice type (solo/duo/group) were considered.
At FP level, the role of personal characteristics (sex, age [mean]), years of experience [mean]), annual antibiotic prescription rate, and the FP’s risk-avoiding attitude were investigated. The annual antibiotic prescription rate during 2011 (children and adults, most recent Belgian data available) was used as a proxy for baseline antibiotic prescribing. National prescribing data only for children were not available. FPs were categorised as high or low prescribers (with the mean rate as cut-off point). As data from early-career FPs and residents were not yet available, they were considered as a separate group. All FPs completed a validated questionnaire measuring their risk-avoiding behaviour. Physicians with higher scores ‘prefer the certain to the uncertain’.19
At child level, considerations included: age (infant, preschool child, child/adolescent), fever (no fever, elevation, high fever [≥39°C]), and the presence of an appropriate indication for antibiotics according to the Belgian guidelines20 (further details may be obtained from authors). The Belgian guidelines follow international guidelines, but the antibiotic choice and dosages are adapted to the Belgian bacterial resistance patterns. The perceived parental expectation regarding antibiotics, which was registered by the FPs at the end of the consultation by answering ‘yes or no’ to the question ‘Do you think this parent expects a prescription for antibiotics?’, was also considered. The option ‘I don’t know’ or missing values were categorised as ‘unknown’.
First, the researchers explored which of these covariates, at the univariate level, influenced immediate antibiotic prescribing. Second, a multivariate analysis was performed. With exception for practice type, which was added because stratification was carried out at this level, only covariates with P-values lower than 0.1 were entered. When comparing intervention groups, limited imbalances for a child’s age and temperature were found. These were added as covariates to the final adjusted analysis. Episodes with missing data about antibiotic prescribing were discarded from the analysis. For more detailed information about the methodology of this trial, the authors refer to the published protocol.18
RESULTS
Participant flow, recruitment, and numbers analysed
Initially 169 FPs started recruitment and 3288 acute infectious episodes were included between 15 February 2013 and 28 February 2014. After applying exclusion criteria (Figure 1), 2227 acute infectious episodes registered by 131 FPs (78 practices) were analysed. Because of the CDR indicating a higher risk for serious infection, 761 episodes (23%) were excluded. Thirty-one physicians were excluded because they included fewer than five children. Their baseline characteristics were equal to those of included FPs (further details of excluded FPs are available from the authors). Due to missing data on antibiotic prescribing, 177 episodes were discarded. These children were of similar age, but had less fever (P<0.001) and fewer indications for antibiotics following the Belgian guidelines (P<0.001) in comparison with children with outcome data on antibiotic prescribing (further information on outcome data is available from the authors).
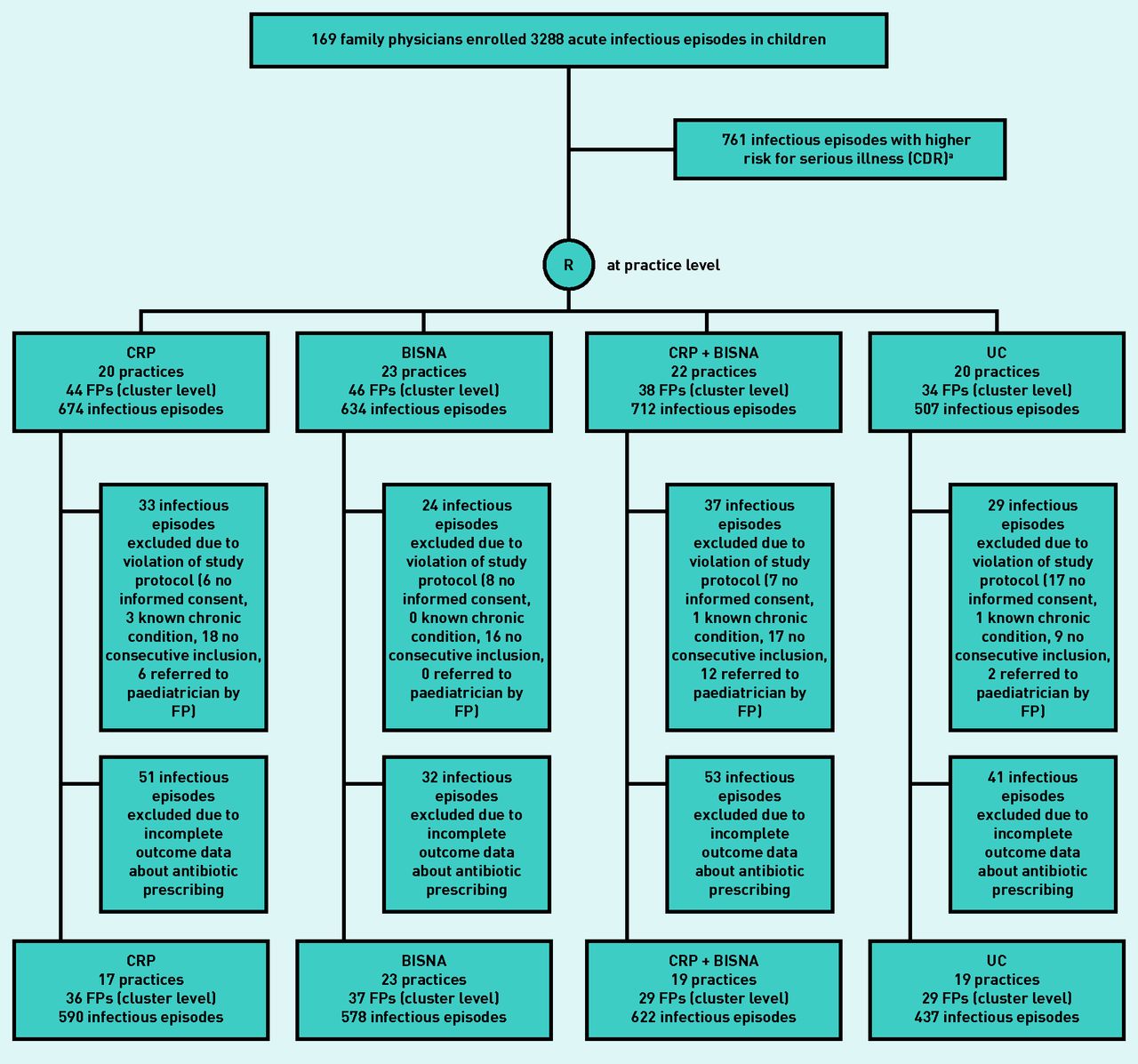
Flow chart representing the number of acute infectious episodes included in the study.
a Scoring positive at one of the following clinical criteria: gut feeling of the physician, presence of dyspnoea, temperature ≥40°C, and diarrhoea in children aged between 1 and 2.5 years. BISNA = brief intervention with safety net. CDR = clinical decision rule. CRP = C-reactive protein. FP = family physician. R = randomisation. UC = usual care.
Baseline characteristics
Family physicians
Forty-one percent of FPs were male. Their mean age was 39.8 years (standard deviation [SD] 10.7 years) and 17.6% were residents. Fifty-seven per cent were practising in a rural region. The mean risk-avoiding behaviour was 17.3 (SD 2.9), and the mean annual antibiotic prescription rate was 41.9% (SD 9.5%). There were no differences between the FPs of different intervention arms regarding personal characteristics, risk-avoiding attitude, and annual antibiotic prescription rate (further details are available from the authors). The median number of included infectious episodes per FP was 11 (interquartile range [IQR] 6 to 17, total range 2 to 304).
Children
Fifty-one per cent of infectious episodes concerned males. Their mean age was 5 years (SD 4.0, IQR 1.6 to 7.6; 30.6% were infants, 37.5% were preschool children, 31.9% were child/teenager) and their mean temperature was 38.2°C (SD 1.1; 25.5% no fever, 43.5% elevation, 29.4% high fever [≥39°C]). The top three preliminary diagnoses were: upper respiratory tract infection (34.4%), acute otitis media (15.5%), and other viral disease (11.8%). There were small imbalances in age and temperature across the intervention groups, but there was no difference in appropriate indications for antibiotics (further details are available from the authors).
Parents returned the diary in 1017 episodes (45.7%). There were no differences in baseline characteristics of children whose parents did or did not return the diary, except a minor difference in the child’s temperature: 4% more parents of children with high fever returned the diary in comparison with those who did not.
Outcomes and estimates
In 593 infectious episodes (26.6%), FPs delivered an antibiotic prescription. In 334 episodes (56.3%), this was an immediate prescription. An appropriate indication to prescribe antibiotics immediately could be found in 13.1% (291 episodes) of all episodes. The FPs prescribed an immediate antibiotic course only in half of these cases. Conversely, there was no appropriate indication in 73.6% (1638 episodes) of all infectious episodes, but antibiotics were prescribed immediately in 125 episodes (7.6%) and a delayed prescription was given in 140 (8.6%) episodes. A judgement of whether there was an appropriate indication for antibiotics could not be made in 298 (13.4%) infectious episodes because information about clinical parameters or preliminary diagnosis was missing (Table 1).
Observed antibiotic prescribing rate in comparison with the presence of a rational indication to prescribe
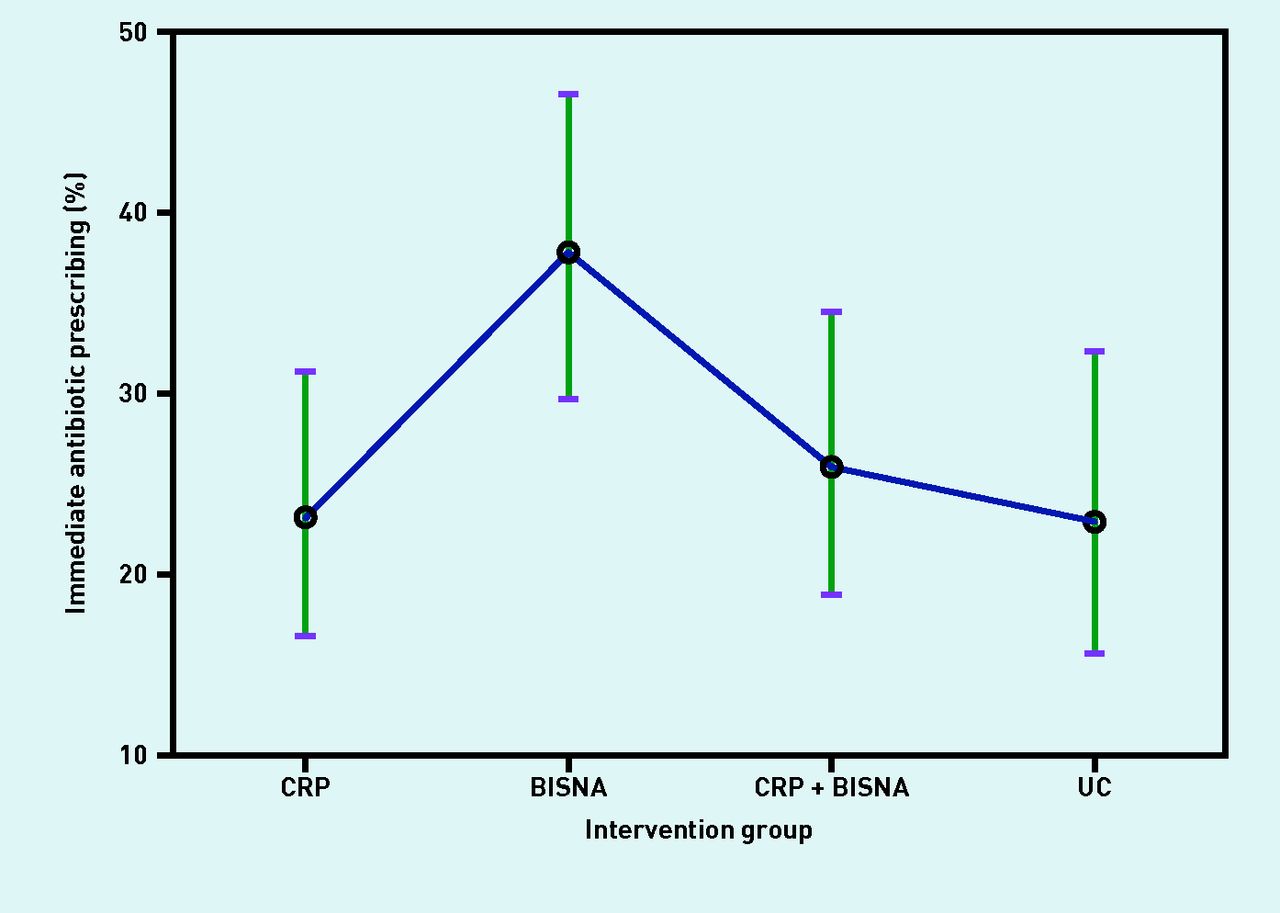
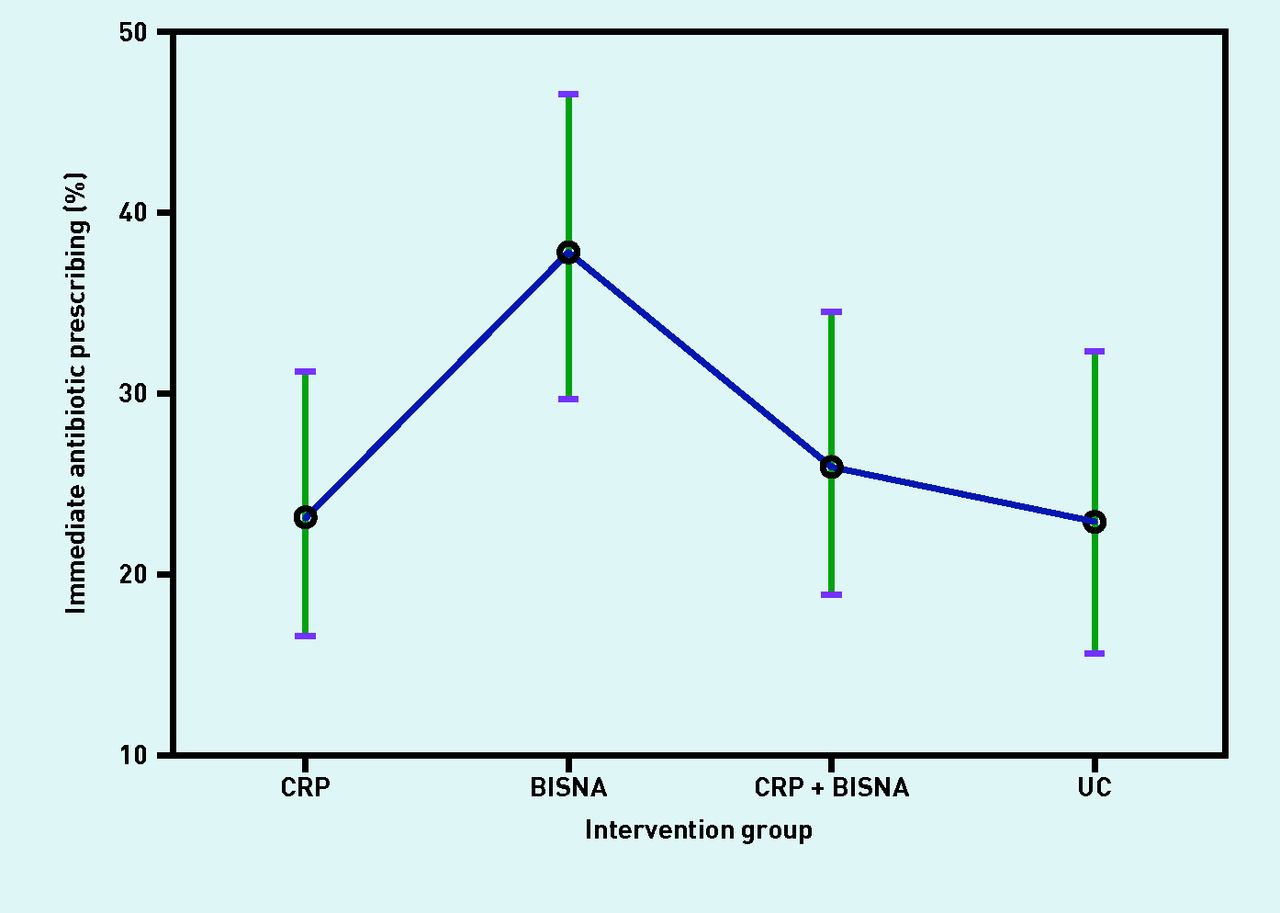
The ICC was low (0.09 at practice level and 0.03 at FP level). The crude mixed logistic regression analysis showed no significant effect of the interventions on antibiotic prescribing. After adjusting for covariates, BISNA increased immediate antibiotic prescribing (adjusted odds ratio [AOR] 2.04, 95% confidence interval [CI] = 1.19 to 3.50) and total antibiotic prescribing (AOR 1.95, 95% CI = 1.11 to 3.42) in comparison with usual care. This increase disappeared when BISNA was combined with POC CRP. Performing a POC CRP test as sole intervention did not influence antibiotic prescribing in comparison with usual care (Table 2, Figure 2) (a complete model is available from authors).
{kind=link}
{kind=link}
Estimated marginal means of the immediate antibiotic prescribing rate (with 95% confidence interval) for the different intervention groups (adjusted analysis). BISNA = brief intervention with safety net. CRP = C-reactive protein. UC = usual care.
Mixed logistic regression analysis (crude and adjusted analysis) to compare intervention effects on immediate antibiotic prescribing
Harms
All children recovered. No child was hospitalised for a serious infection. Based on data from the diaries, children recovered on average 4 days (SD 3.8 days) after the consultation. There were no differences in time to recovery across the intervention groups, nor across children with or without antibiotics, whether appropriate or not.
DISCUSSION
Summary
For non-severe infections in children in which inappropriate prescribing could be reduced safely, performing a POC CRP test did not reduce antibiotic prescribing. Improving mutual understanding by eliciting parental concerns and providing safety net advice without POC CRP testing conversely increased antibiotic prescribing.
Strengths and limitations
A cluster randomisation trial was chosen because its design mimics daily practice, where certain tools are either available in the surgery or not. Furthermore, once the content of the communicative intervention is known it would be difficult (and uncontrollable) for individual physicians to switch randomly between the interventions. Preliminary diagnoses registered by the FP were classified independently by two investigators to avoid imprecision bias in coding, using the International Classification of Primary Care (ICPC).
The antibiotic prescribing rate was lower than expected. Based on data from a Belgian continuous and integrated computerised morbidity registration network (INTEGO),21 a prescribing rate of 40% was expected. In these data, however, no distinction can be made between severe and non-severe infections. Furthermore, FPs may have been more willing to avoid prescribing antibiotics during the trial because they were eager to perform well.22 The low prescribing rate in the current study cannot be explained by the selection of participating FPs, as their mean annual antibiotic prescription rate was comparable to the national mean. Moreover, 37.4% of the immediate prescriptions could still be considered inappropriate, thus highlighting room for improvement.
Results from this study could be generalisable to similar children in other Western countries. Results, however, may be different among countries with less accessible health care. The results here are not applicable for children at high risk for serious infection.
Comparison with existing literature
A recent Cochrane review identified six randomised trials that evaluated the use of POC CRP tests in acute respiratory tract infections in primary care.12 The pooled result for all trials showed a reduction in antibiotic use (risk ratio [RR] 0.90, 95% CI = 0.80 to 1.02; I2 = 5% for RCTs and RR 0.68, 95% CI = 0.61 to 0.75; I2 = 0% for cluster RCTs). The most pronounced effect occurred in studies with a restrictive CRP algorithm. Its effect in children was only investigated in a small group of children (Diederichsen et al :23 139 children with a respiratory infection, RR 1.09, 95% CI = 0.70 to 1.71; Van den Bruel et al:17 54 children with temperature of ≥38°C, P-value = 0.627). Both studies found no reduction in antibiotic prescribing; however, no conclusions can be drawn because they were clearly underpowered. Nevertheless, their findings are in line with the findings of the present study, which collected a much larger data sample. Contrary to the current study, Diederichsen et al 23 and Van den Bruel et al 17 provided some guidance about CRP and antibiotic prescribing. In the trial of Diederichsen et al,23 strict cut-off values were not given, but information was provided that a normal CRP level was <10 mg/L and that CRP levels <50 mg/L were seldom the result of bacterial infection. These values were based on an article by Thompson et al with an unclear methodology.24 In the trial by Van den Bruel et al,17 FPs were informed that a serious infection was less likely when the CRP level was <20 mg/L and more likely when the level was >80 mg/L. The cut-off level of 20 mg/L was adopted from trials in high-prevalence settings such as emergency units and paediatric assessment clinics. As the authors also conclude, this strategy should be assessed before widespread implementation, as studies suggest that serious infections can be present in children with CRP levels as low as 5 mg/L.25,26 As reliable cut-offs are not available, the authors opted not to provide guidance in this study. Obviously, FPs are aware of normal values of CRP.
A recent Cochrane review,15 identifying 10 trials assessing a variety of interventions to promote shared decision-making to reduce antibiotic prescribing in acute respiratory infections in primary care, found a reduction of 32–45% in antibiotic prescribing compared with usual care in the short term. These trials provided support such as communication skills training, interactive workshops, seminars, and web-based platforms. Five studies recruited children, but no separate analysis assessed the effect of the interventions in this subgroup. The brief intervention used in this study had the advantage of being cheap, reproducible, and immediately applicable in practice without extensive training, but, unfortunately, failed and even doubled prescribing rates, except when POC CRP testing was at their disposal. It appears that extensive, multifaceted training is needed to reduce antibiotic prescribing.
Implications for research and practice
Systematic POC CRP testing without proper guidance was not found to be an effective strategy to tackle antibiotic overprescribing and should not be recommended for this purpose. So far, CRP testing has only shown to be useful to avoid unnecessary hospital admissions in children at higher risk for serious infection.26 Reliable cut- off levels for CRP to distinguish children with self-limiting infections from those who benefit from antibiotic treatment may be needed to make POC CRP a more useful tool to improve antibiotic prescribing.
Eliciting parental concern and providing a safety net surprisingly increased antibiotic prescribing — the reasons for this can only be presumed. Apparently, parental concern can settle in the FPs’ mind and, instead of reassuring the parent verbally, they felt the need to prescribe antibiotics, except when an objective marker (CRP) is measured. A qualitative analysis of the answers to the questions about concerns and in-depth interviews with participating FPs will further help understand why FPs prescribed antibiotics more often when discussing parental worries.
Acknowledgments
This article was written on behalf of the ERNIE2 study collaboration. The authors wish to acknowledge the other principal ERNIE2 investigators: Dominique Bullens, Karin Decaestecker, Katrien De Schynkel, Jasmine Leus, Karl Logghe, Luc Pattyn, Marc Raes, Lut Van den Berghe and Christel Van Geet. The authors would like to thank all participating FPs and paediatricians at participating hospitals; Annelien Poppe, Frederick Albert, and Greet Delvou for daily follow-up during the study; Kaatje Van Roy for her support in the processing of the data; and IKEA, Belgium, for providing finger puppets that were handed out to participating children as a token of appreciation. And, finally, the authors wish to thank all children and parents who took part in this study.
Notes
Funding
This study was funded by the National Institute for Health and Disability Insurance (RIZIV, Belgium) (reference: CGV 2012/235) and the Research Foundation Flanders (FWO) (reference: G067509N).
Ethical approval
The protocol of this study was approved by the Ethical Review Board of the University Hospitals/KU Leuven (reference: ML8601).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
All authors declare that support was exclusively provided by the funding organisations mentioned above; that there are no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; and that no other relationships or activities could appear to have influenced the submitted work.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 15, 2017.
- Revision requested July 31, 2017.
- Accepted October 2, 2017.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

