


Abstract
Background Kidney function reduces with age, increasing the risk of harm from increased blood levels of many medicines. Although estimated glomerular filtration rate (eGFR) is reported for prescribing decisions in those aged ≥65 years, creatinine clearance (Cockcroft–Gault) gives a more accurate estimate of kidney function.
Aim To explore the extent of prescribing outside recommendations for people aged ≥65 years with reduced kidney function in primary care and to assess the impact of using eGFR instead of creatinine clearance to calculate kidney function.
Design and setting A cross-sectional survey of anonymised prescribing data in people aged ≥65 years from all 80 general practices (70 900 patients) in a north of England former primary care trust.
Method The prevalence of prescribing outside recommendations was analysed for eight exemplar drugs. Data were collected for age, sex, actual weight, serum creatinine, and eGFR. Kidney function as creatinine clearance (Cockcroft–Gault) was calculated using actual body weight and estimated ideal body weight.
Results Kidney function was too low for recommended prescribing in 4–40% of people aged ≥65 years, and in 24–80% of people aged ≥85 years despite more than 90% of patients having recent recorded kidney function results. Using eGFR overestimated kidney function for 3–28% of those aged ≥65 years, and for 13–58% of those aged ≥85 years. Increased age predicted higher odds of having a kidney function estimate too low for recommended prescribing of the study drugs.
Conclusion Prescribing recommendations when kidney function is reduced are not applied for many people aged ≥65 years in primary care. Using eGFR considerably overestimates kidney function for prescribing and, therefore, creatinine clearance (Cockcroft–Gault) should be assessed when prescribing for these people. Interventions are needed to aid prescribers when kidney function is reduced.
- Cockcroft–Gault
- creatinine
- drug prescriptions
- kidney function
- older people
- prescribing recommendations
- renal insufficiency
INTRODUCTION
Prescribing when a patient’s kidney function is reduced should include consideration of the risk from increased blood levels when drugs excreted renally are eliminated more slowly.1 With ageing, a progressive loss of functional capabilities in most body organs, changed responses to receptor stimulation, and decreased homeostatic mechanisms have implications for drug handling. Of these changes, excretion is the most significant and important age-related pharmacokinetic change, and is both predictable and measurable. Two-thirds of people aged 70–80 years have approximately half the kidney function of a ‘young adult’,2,3 with an average decline of approximately 1 ml/minute annually after 30 years old, decreasing more rapidly after 65 years of age.4
Harm and hospitalisation are potential outcomes when recommendations for altering prescribing are not applied. In other European countries, a large primary care study found drug use not recommended when kidney function was reduced in people aged ≥65 years caused a 40% increase in all-cause mortality;5 one-third of hospital admissions related to adverse drug reactions were judged to be caused by renal impairment in those aged ≥65 years;6 and one-third of adverse drug reactions in people aged ≥65 years during their hospital stay were associated with reduced kidney function.7
The National Institute for Health and Care Excellence (NICE) guidance on chronic kidney disease (CKD)8 recommends ‘review of medications’, and now the NICE acute kidney injury guidelines9 and alerts require GPs to review medicines after an acute kidney injury episode. These include drugs that are a direct risk to the kidney, such as non-steroidal anti-inflammatory drugs (NSAIDs), angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II receptor blockers (ARBs); and drugs that are more likely to cause adverse drug reactions when blood levels are increased as a result of slower elimination, such as metformin, gabapentin, and pregabalin. Reduced kidney function can also reduce the effectiveness of some drugs, such as thiazides and nitrofurantoin.
Estimated glomerular filtration rate (eGFR) has been reported with pathology results since the introduction of the CKD guidelines in 2003, and is calculated using the ‘Modification of Diet in Renal Disease’ equation,10 and more recently, the CKD Epidemiology Collaboration (CKD-EPI) formula.11 eGFR was developed to provide staging for CKD and does not have a weight component, therefore, making it straightforward for pathology to report. Drug-dosing studies, however, have used the Cockcroft–Gault equation12 to estimate kidney function as ‘creatinine clearance’ (CrCl). Cockcroft–Gault includes a weight component: ideal body weight to factor muscle mass, not body fat, as creatinine is produced from muscle turnover.13 The equations give progressively different results with increasing age, and studies focused on prescribing for older people have concluded that Cockcroft–Gault should continue to be used for prescribing decisions.14,15 Studies using gentamicin have shown that blood levels are more closely estimated by creatinine clearance: while Cockcroft–Gault underestimates kidney function and effect on drug blood levels by 10% across all older ages, eGFR overestimates kidney function increasingly as age increases by 29% up to 69%,16 meaning the safer estimate to use is Cockcroft–Gault.17,18 Using eGFR for prescribing decisions, rather than Cockcroft–Gault, has been shown to lead to more frequent major bleeding events with glycoprotein-IIb-IIa-inhibitors,19 and increases the likelihood of adverse drug reactions,20 hospitalisation,6 or ineffectiveness.21
How this fits in
Internationally, studies have found that recommendations for prescribing in patients with reduced kidney function are often not applied, with increased risk of patient harm and hospital admissions. How medicines affected by renal impairment are prescribed to those aged ≥65 years in primary care was previously unknown. This survey found many people aged ≥65 years in UK general practice had a recorded estimate of kidney function but their prescribed drugs had not been adjusted. Data were available to calculate creatinine clearance (Cockcroft–Gault); when creatinine clearance estimates were applied even more patients were identified as at a risk. The findings from this study have informed an update to the British National Formulary to recommend the Cockcroft–Gault formula as the preferred method for estimating renal function in older people.
International studies have found prescribing outside recommendations for older people with reduced kidney function,5,22 but, while a similar problem has been shown in a UK hospital,23 to the authors’ knowledge, no studies have been conducted in UK general practice. The aim of this study was to assess whether drugs are prescribed according to the British National Formulary (BNF)13 and the Electronic Medicines Compendium (eMC), summary of product characteristics (www.medicines.org.uk/emc/) when kidney function is reduced, for people aged ≥65 years across a healthcare population. The study also set out to determine the impact of using eGFR instead of creatinine clearance (Cockcroft–Gault) on drug and dosage decisions.
METHOD
A cross-sectional survey was conducted on prescribing data from all 80 general practices in a north of England former primary care trust (PCT).
Two drugs, or drug classes, were identified in each of four categories in reduced kidney function:
drugs that should be avoided;
drugs that should have a dose reduction;
drugs that are ineffective; and
drugs that require caution as they are known to frequently cause adverse drug reactions in renal impairment.
The eight choices of drugs were based on findings in a previous case-note review of five practices in the PCT.24 Drugs were selected on the strength of the BNF/SPC (summaries of product characteristics) recommendations and the literature5,21–22,25–32 impact on patients,28,33–40 and independent expert advice from a renal physician, geriatrician, hospital renal pharmacist, and an antibiotics expert pharmacist (Table 1).
Choices of drugs and drug classes investigated in the study
Data collection
Data collected were age, sex, actual weight and date last recorded, serum creatinine and date last recorded, eGFR and date last recorded, or no eGFR ever recorded. These data were used to calculate creatinine clearance using actual body weight (CrCl-AW) and creatinine clearance using estimated ideal body weight (CrCl-IBW).
Searches were run for all patients prescribed each drug by a PCT data analyst at the end of October 2011 to extract data from general practice systems. All practices used the TPP SystmOne clinical information system.
Data analysis
Data quality and missing data analyses were performed, and a descriptive analysis to give:
the numbers of people aged ≥65 years with eGFR <60 ml/minute/1.73 m2 (NICE CKD level);8 and
the numbers of people aged ≥65 years taking each of the study drugs.
For each of the eight drugs the number of patients in age bands ≥65, 65–74, 75–84, and ≥85 years were assessed; for seven drugs on the repeat medication list, and for nitrofurantoin, at least one prescription in the previous 12 months, described as ‘patient drug events’. For each drug the following data were collected and/or calculated:
the number of ’patient drug events’ where a serum creatinine level had been recorded in the previous 15 months, and the estimated kidney function was too low for the recommended use, calculated using eGFR, CrCl-AW and CrCl-IBW;
the number of ‘patient drug events’ that would be missed if eGFR, or actual weight in Cockcroft–Gault, were used;
the number of ‘patient drug events’ for each drug where there was no kidney function estimate on the record;
Spearman correlation between age and level of kidney function (using SPSS version 21); and
Logistic regression analysis to explore the effect of people aged ≥65 years on the likelihood of having a kidney function too low for appropriate prescribing of the drug (using SPSS version 21).
Data oversight was provided by the supervisory research team.
RESULTS
Thirteen per cent of the PCT population were aged ≥65 years (70 900/549 533), and 1.8% (9723) were aged ≥85 years; 26% of those aged ≥65 years, and 50% of those aged ≥85 years, had a documented eGFR ≥60 ml/minute/1.73 m2.
A recent kidney function test in the previous 15 months was found in the patient record for 83% of patients prescribed NSAIDs and for 97% of patients prescribed metformin. Only 0.2–9.7% of the patient drug events had no eGFR, and 0–5.7% did not include the parameters to be able to calculate CrCl-IBW.
Figure 1 shows the numbers of patients prescribed each of the drugs studied; an ACEI or ARB was found to be prescribed for 40% of the 70 900 patients ≥65 years.

Number of people aged ≥65 years prescribed each of the study drugs. ACEI = angiotensin-converting enzyme inhibitor. ARB = angiotensin II receptor blocker. NSAID = non-steroidal anti-inflammatory drug.
Prevalence of low kidney function
The number of patient drug events where a recent kidney function was available but was too low for the recommended drug use ranged from 39.6% (95% confidence interval [CI] = 35.8 to 43.4%) for nitrofurantoin, to 3.5% (95% CI = 0 to 11.2.0%) for NSAIDs in those aged ≥65 years, and 79.5% (95% CI = 75.1 to 83.9%) (nitrofurantoin), to 29.2% (95% CI = 0.5 to 57.9%) (NSAIDs) for the patients aged ≥85 years (Table 2).
Number of drugs prescribed for people aged ≥65 years with a kidney function estimate (CrCl-CG IBW) in the previous 15 months below that for recommended use
Figure 2 shows an example line plot charting the range of kidney function (CrCl-IBW in the previous 15 months) for nitrofurantoin at each age level for those aged ≥65 years. All cases below the line at CrCl-IBW 45 ml/minute had a kidney function likely to be too low for the drug to be effective, and more likely to cause adverse drug reactions.28
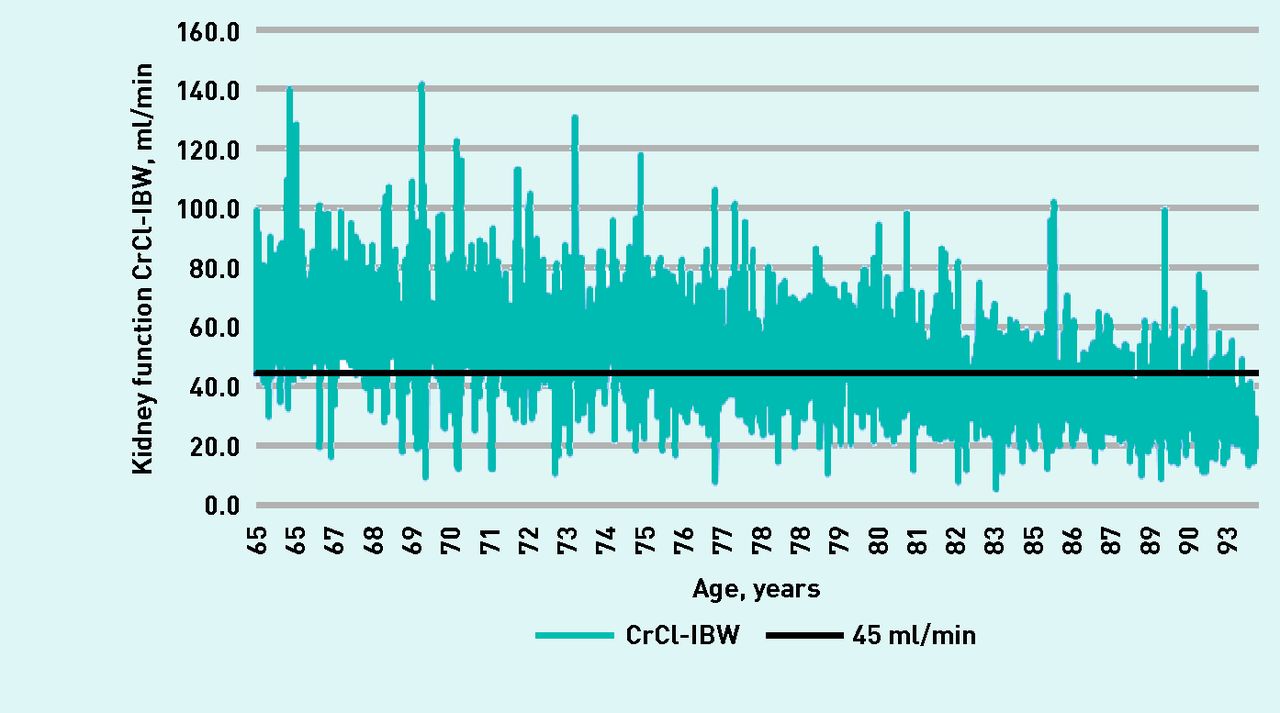
Range of kidney function using creatinine clearance (Cockcroft–Gault) calculated using estimated ideal body weight (CrCl-IBW) in the previous 15 months, for nitrofurantoin prescribed at each age level ≥65 years.
Different ways to estimate kidney function
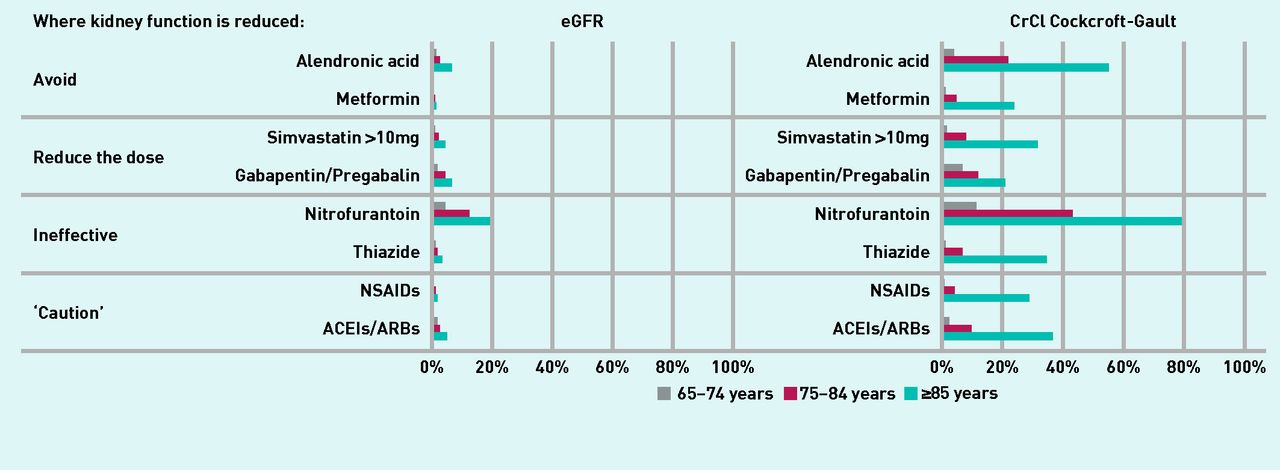
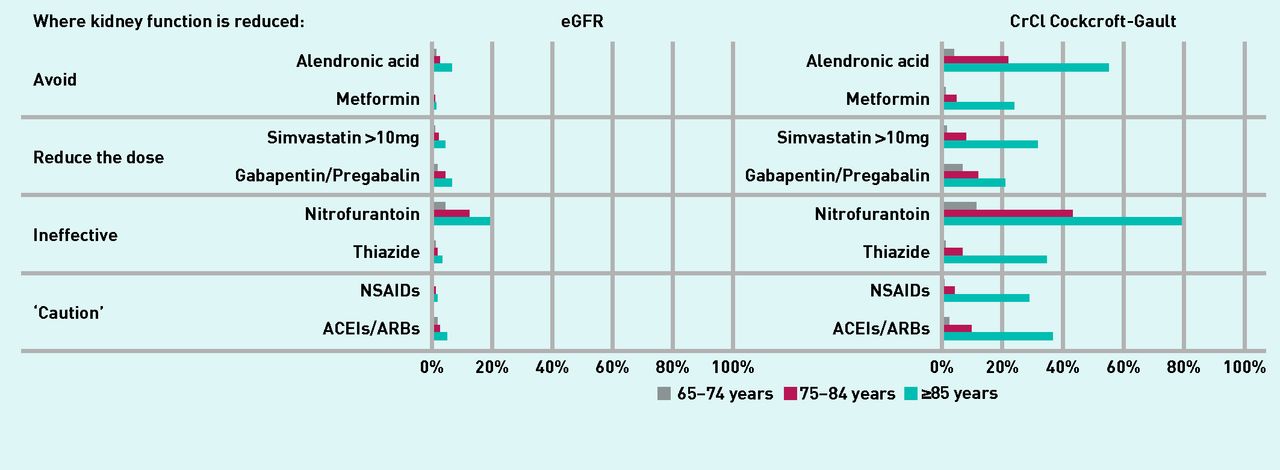
Using eGFR to estimate the level of kidney function suggested that a much lower number of alterations were required for drug or dose choice than would be the case using CrCl-IBW (Figure 3). Use of eGFR, rather than CrCl-IBW, would mean that the suggested alteration or stopping of the study drugs would be missed for 3–28% of those aged ≥65 years, and for 13–58% for those aged ≥85 years.
{kind=link}
{kind=link}
{kind=link}
Percentage of patients found with a kidney function too low for recommended use of the drug using estimated glomerular filtration rate compared with creatinine clearance (Cockcroft–Gault) in the three older age bands. ACEIs = angiotensin-converting enzyme inhibitor. ARBs = angiotensin II receptor blockers. CrCI = creatinine clearance. eGFR = estimated glomerular filtration rate. NSAIDs = non-steroidal anti-inflammatory drugs.
Using actual weight in the Cockcroft–Gault equation also found fewer patients who might need prescribing alteration, but to a lesser extent than using eGFR: the suggested alteration or stopping of the study drugs would be missed for 1–10% of patients aged ≥65 years.
Effect of increased age
Kidney function reduced with age for all groups studied using Spearman correlation, for example, for nitrofurantoin (r = −0.608, n = 3185, P<0.001). Logistic regression analysis found that, compared with age band 65–74 years, patient drug events for those aged 75–84 years had higher odds of being prescribed drugs where the kidney function was too low, and even higher odds for those ≥85 years (Table 3). For example, for nitrofurantoin, using CrCl-IBW the patient drug events for people aged 75–84 years had 5.64 (95% CI = 4.58 to 6.95) times greater odds of being prescribed drugs where the kidney function was too low for recommended use, and 29.23 (95% CI = 22.75 to 37.56) times greater odds for those aged ≥85 years.
The odds of having a kidney function too low for the drug with increased age compared with those aged 65–74 years, using eGFR, creatinine clearance (Cockcroft–Gault) calculated using actual body weight, and using ideal body weight
DISCUSSION
Summary
Prescribing of drugs outside recommendations for use in reduced kidney function was widespread for the eight representative drugs in the study population. Using eGFR, rather than CrCl- IBW, considerably underestimated the potential risk to patients, particularly for those aged ≥85 years.
Prescribing recommendations in reduced kidney function were not applied for a large number of people aged ≥65 years, in this first UK general practice study. Assessment of Cockcroft-Gault creatinine clearance to estimate kidney function level when making prescribing decisions for people aged ≥65 years will find more at risk of higher drug blood levels than eGFR, and reduce the risk of harm.
Strengths and limitations
The study population was from a large PCT with a broad range of prescribers. A deprivation score higher than the England average, a lower life expectancy, and a slightly younger population,40 suggests that the study findings might be an underestimation of the problem in the UK. Only a small number of data were excluded, where no kidney function data were available, giving confidence in the findings being representative.
Anonymised ‘patient drug events’ were collected, but it is likely that many patients were prescribed more than one drug. Inferences cannot be made on the group of drugs as a whole in this study, or the prevalence of a patient having more than one drug affected by level of kidney function. A case-note review in five GP practices found that 25% of patients aged ≥65 years were prescribed an average of two drugs when their kidney function was too low for recommended use, and 70 different drugs were involved.24
Comparison with existing literature
International prevalence studies in primary and secondary care have reported large numbers of drug use and dosing outside recommendations.5,22,25–32 A French multicentre prospective primary care study found 13.3% of patients aged ≥65 years with a kidney function too low for recommended use, 52.5% in those with eGFR 30–59, and 96% with eGFR <30 ml/minute/1.73 m2.5 A retrospective case record analysis of patients aged >70 years in a UK hospital found 13% had ‘potentially inappropriate prescribing’.23
A recent kidney function level was recorded in the patient record for most (90%) people aged ≥65 years prescribed the included drugs in the current study. The UK Quality Outcomes Framework48 targets may have helped because kidney function testing has been incentivised, for example, in diabetes. However, renal impairment did not seem to lead to altered prescribing in all four categories of drugs studied, which may impact on patient safety from increased blood drug levels, sensitivity, or ineffectiveness. For all drugs studied, the dose could have been reduced or an alternative treatment chosen (such as atorvastatin, which is not affected by level of kidney function) instead of simvastatin, or another antihypertensive or antidiabetic medication.
Increased age predicted higher odds of having a kidney function estimate too low for recommended prescribing. This analysis did not address the possibility of confounders, but there is broad evidence of progressive loss of kidney function with ageing.2,3 Those aged ≥65 years are more likely to have a lower kidney function, and so a lower reserve to react to assaults such as dehydration or nephrotoxicity of drugs. Renal impairment, polypharmacy, and identified drugs such as NSAIDs are included as ‘deficits’ that can occur with ageing and combine to increase ‘frailty’ which, in turn, increases the risk of adverse outcomes.49
The equation used to estimate kidney function for prescribing decisions made a substantial difference to whether prescribing might be reviewed because of renal impairment in people aged ≥65 years. Many other studies report variance in estimating of kidney function when different equations are used, ranging from an Italian hospital study that found 9.8% dosing outside recommendations if eGFR was used,50 to a Spanish hospital study of nephrotoxic drugs, which found 65% dosing outside recommendations.51 A US primary care study found that 40% of patients should have been recommended different doses, and 22% of those reviewed would have had different recommendations based on the equation chosen.52 The current study found that using eGFR would mean that many people needing a review of prescribing would be missed. It also showed that using actual weight in the Cockcroft–Gault equation would miss drugs that might need review; an ideal body weight, or actual body weight if lower, should therefore be used in the Cockcroft–Gault calculation to give an indication of muscle mass.13,14
Implications for research and practice
Treatment of multimorbidity has resulted in increasing numbers of people aged ≥65 years being prescribed more long-term medicines, the mean being seven for people aged ≥80 years,53 and 60% of the billion items dispensed in the community in England are for people aged ≥65 years.54 As many people aged ≥65 years are prescribed multiple medications, there is the likelihood that they will be taking more than one drug eliminated via the kidneys, increasing the complexity of the impact. Applying BNF recommendations for prescribing (or avoidance of prescribing) in renal impairment could reduce the risk of adverse drug reactions, particularly for the oldest and most frail patients.
In 2017 the BNF reviewed the evidence from this study and updated its recommendation in the ‘Prescribing in Renal Impairment’ section to state that ‘... the Cockcroft and Gault formula is the preferred method for estimating renal function in elderly patients aged 75 years and over’.13,55 Electronic patient record systems, such as SystmOne and EMIS, have a ‘renal calculator’ to enable prescribers to calculate, and code, creatinine clearance Cockcroft–Gault; smartphone apps are also available and easy to use. Pharmacists have been shown to significantly reduce prescribing outside recommendations in reduced kidney function;56 they can audit, highlight for review, and do medication reviews for high-risk populations.
The data required to calculate creatinine clearance and identify affected drugs are already available in the prescribing and consultation systems; it would be possible to develop patient- and drug-specific decision support to suggest safer doses or alternative drugs, both at initiation and at medication review. Further research has been undertaken to understand why GPs often do not apply renal impairment recommendations when prescribing, and to inform an intervention to aid prescribing in reduced kidney function.57
Guidelines should consider recommendations for drug use and level of kidney function.58 CKD and acute kidney injury guidelines could include guidance on prescribing (and avoiding prescribing) to reduce risk to the kidney and reduce adverse drug reactions from renally excreted drugs. The NHS England Think Kidneys resources include an acute kidney injury medicines optimisation toolkit (www.thinkkidneys.nhs.uk) aimed at prescribers in hospitals, which could be usefully extended to primary care. Non-prescription medicines could be important for future research, for example NSAIDs bought from pharmacies or retail outlets.
Acknowledgments
The authors thank the PCT research coordinator Paul Carder, data analyst Simon Falkner, and the statistics advice received from Professor Robert West.
Notes
Funding
This research was carried out as part of a self-funded PhD at the University of Leeds.
Ethical approval
Not required for this study.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received July 11, 2017.
- Revision requested August 15, 2017.
- Accepted December 21, 2017.
- © British Journal of General Practice 2018
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

