


Abstract
Background Gynaecological cancers are the second most common female cancer type, with survival rates in the UK lower than in many comparable countries. A potentially important factor in the UK’s poorer cancer outcomes is diagnostic delay; gynaecological cancers are the cancer type most likely to be affected by less timely diagnosis.
Aim To examine current evidence for factors that contribute to patient and primary care delays in the diagnostic pathway of gynaecological cancer.
Design and setting A systematic review of the available literature.
Method PRISMA guidelines were followed. MEDLINE and Embase databases and the Cochrane Library were searched using three terms: primary care; gynaecological cancer; and delay. Citation lists of all identified articles were searched. Two authors independently screened the titles, abstracts, and full texts of publications. Data extraction was performed by one author and quality assured by a second reviewer in a 20% sample of selected articles. Synthesis was narrative.
Results A total of 1253 references was identified, of which 37 met the inclusion criteria. Factors associated with delayed diagnosis were categorised as either patient factors (patient demographics, symptoms or knowledge, and presentation to the GP) or primary care factors (doctor factors: patient demographics, symptoms or knowledge, and referral process); and system factors (such as limited access to investigations).
Conclusion Delayed diagnosis in the patient and primary care intervals of the diagnostic journey of gynaecological cancer is complex and multifactorial. This review identifies areas of future research that could lead to interventions to enable prompter diagnosis of gynaecological cancers.
INTRODUCTION
Despite improvement, UK survival for the five most common gynaecological cancers (ovarian, cervical, endometrial, vagina, and vulval) lags behind that in comparable countries such as France and Germany.1 The relatively low survival in the UK may reflect later diagnosis, with delayed referral from primary care contributing.2 Gynaecological cancer is more likely than other cancer types to be affected by less timely diagnosis.3 Several primary care-based initiatives have been introduced to try to improve survival through earlier diagnosis, including patient education, urgent suspected cancer referral (USCR) guidelines, risk assessment tools, and improved access to diagnostic testing, but it is unknown if these initiatives have improved morbidity and mortality.4 USCR guidelines for suspected gynaecological cancer recommend the use of pelvic examination (abdominal palpation and bimanual examination with or without visualisation of the cervix), although its effect is yet to be determined.5,6
Research into early diagnosis of cancer is complex. The diagnostic pathway of cancer consists of several discrete stages, from when a patient notices a worrying symptom to the pathological confirmation. These stages are described in the Aarhus statement (Figure 1).7 Fully understanding each stage could inform effective interventions to reduce overall diagnostic delay. However, there is a paucity of coherent evidence to inform interventions. Therefore, this systematic review aimed to address the research question: what factors influence patient and primary care delay in the diagnostic pathway of gynaecological cancer?

The stages of cancer diagnosis according to the Aarhus statement.7
METHOD
A systematic narrative review was conducted. A computerised database search was performed in September 2014 and updated on 17 March 2017. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria were followed.
Search strategy
The search strategy included three terms, their synonyms, and MeSH terms: primary care, gynaecological cancer, and diagnosis. The full strategy is available from the authors on request. The Cochrane Library and MEDLINE and Embase databases were searched and citation lists of identified articles were searched manually by one of the authors. All study types from January 2000 to March 2017 were included: controlled and uncontrolled quantitative studies, and qualitative studies.
Inclusion and exclusion criteria
Included studies:
were based in primary care;
involved patients aged >18 years with gynaecological cancer or symptoms potentially indicative of gynaecological cancer, and primary care practitioners who were GPs; and
described referrals from primary to secondary care and/or stages of the diagnostic pathways as described in the Aarhus statement.7
Excluded studies involved:
non-English articles;
articles from low- and medium-income countries; and
editorials, unpublished work, and academic theses.
How this fits in
Despite its prevalence and evidence that it is associated with diagnostic delay, it is not clear which factors are important in the diagnostic pathway of gynaecological cancer. This study shows that diagnostic delay is multifactorial, with a complex interplay of mutually interdependent relationships between patient and primary care factors. Identifying areas of further research, the study also identifies areas where the introduction of a complex intervention has the potential to improve patient outcomes.
Study selection
Titles, abstracts, and full articles were sequentially screened by one author against the inclusion and exclusion criteria. The same author obtained full-text articles for all eligible abstracts. Any disagreements were resolved by discussion between two researchers.
Quality appraisal
Each included article was assessed using the relevant Critical Appraisal Skills Programme (CASP) tool. Well-established CASP tools are validated for the study methodologies included in the review.
Data extraction and analysis
Data were extracted from eligible articles to a data collection form. The full data collection form is available from the authors on request. Data extraction was performed by one author. Twenty per cent of the articles were independently reviewed by one of two authors. Synthesis was narrative.8 Overarching themes were identified after initial reading. Three main themes emerged inductively after detailed reading. Re-reading of the included articles allowed cross-referencing of data to these themes and development of subthemes.
RESULTS
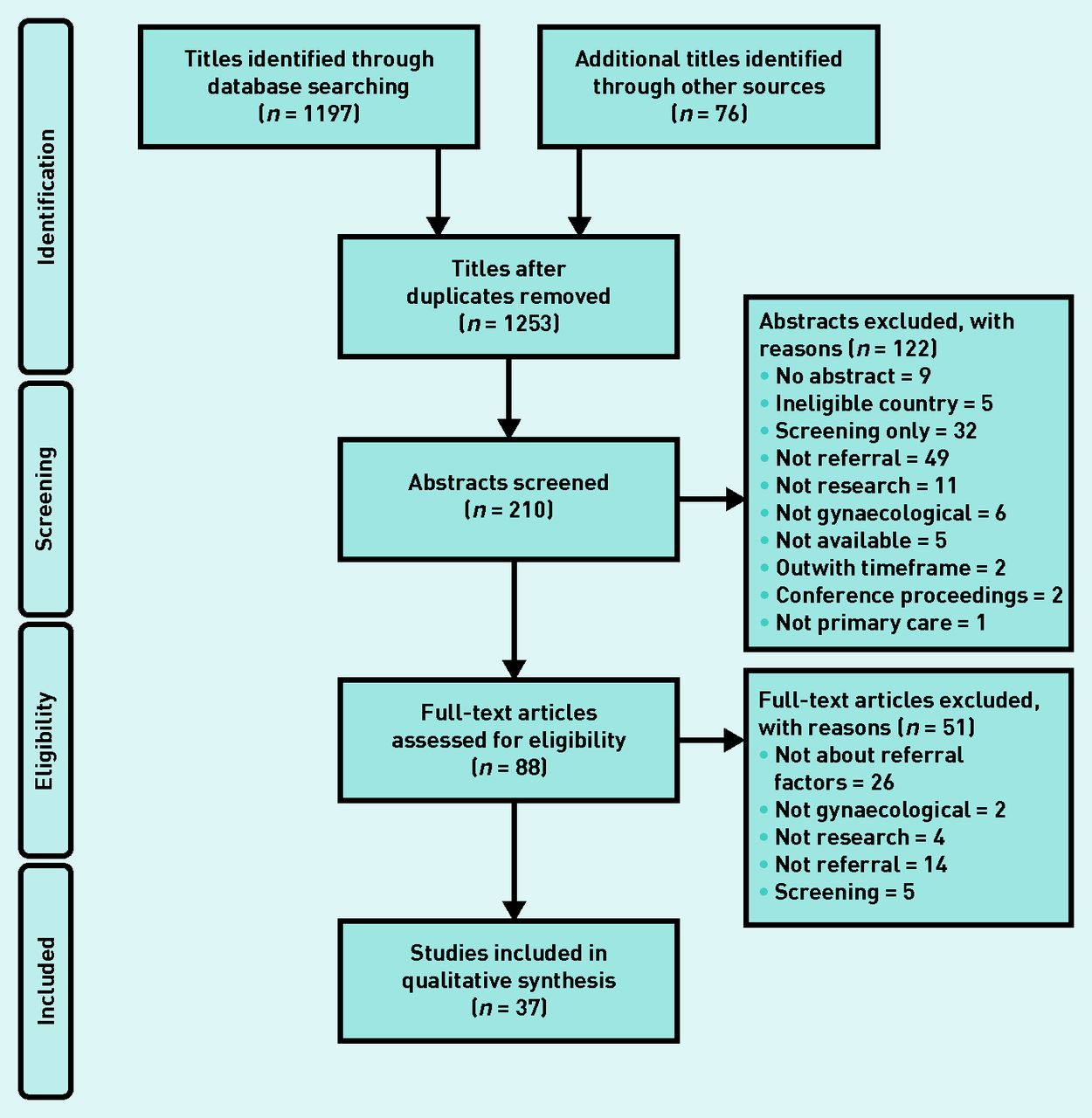
A PRISMA diagram for the systematic review is shown in Figure 2. The search identified 1253 titles; 210 abstracts were screened with 122 being excluded; 88 full text articles were assessed with 37 meeting the inclusion criteria. Full details of the studies are available from the authors on request.9–45 The reasons for abstract and full article exclusions are given in Figure 2.
{kind=link}
{kind=link}
PRISMA diagram.
Various methodologies were employed: 15 cohort studies, five retrospective note reviews, four questionnaire studies, three qualitative studies, two mixed methods studies using both qualitative and data analysis, three telephone surveys, one cross-sectional analysis, three secondary data analysis studies, and one review.
Poor study quality did not affect inclusion of articles. A detailed cohort quality checklist is available from the authors on request.
Initial reading of the data identified three themes that mapped on to the diagnostic intervals described in the Aarhus statement (patient factors, doctor factors, and system factors).7 Further analysis identified subthemes as outlined below.
Patient factors
Patient demographics
Four articles demonstrated the lack of influence of socioeconomic status (SES) on the diagnostic journey,9–12 although one demonstrated diagnostic delay in patients of lower SES diagnosed with endometrial cancer.10 In countries where health care is based on insurance and payment, low income was linked to diagnostic delay and delays in treatment.13,14 In Denmark, women of higher SES appeared more capable of ‘seeking and sustaining treatment’,15 reinforcing work that showed women of higher SES were more likely to speed up health-seeking behaviour.11 Further work in Denmark demonstrated a link between SES and survival: endometrial and ovarian cancer mortality was highest in women with low educational attainment, whereas survival from cervical cancer was highest in those of higher SES.16 Macleod et al 12 demonstrated no effect of educational status on delay; however, Hansen et al 17 demonstrated decreased delay in those with higher educational attainment. Ashing-Giwa et al 13 found an association between lower survival and lower attainment. Women of higher educational status are more likely to be referred in primary care to specialists.18 A pooled analysis of 18 studies identified an association between lower educational attainment and an increased risk of advanced stage at diagnosis of ovarian cancer.14
The effect of ethnicity was mixed. Although one author demonstrated black or ethnic minority women in the UK were more likely to require three or more visits to their GPs before referral,19 two demonstrated no link with ethnicity and delay.9,12 Poorer survival rates were observed in black and Latino women in the US,13 and Pacific and Maori women in New Zealand,20 suggesting that other factors, such as cultural attitudes, might influence survival.
Six studies conducted in the UK, Sweden, and Denmark identified age as a factor. Three found that females aged ≥75 years and those who were housebound were more likely to present earlier, along with those patients who were retired.21–23 Females of working age were more likely to delay presentation,16 although a review found that age was not a factor.12 Patients diagnosed with ovarian cancer aged ≤55 years were found to be more likely to have had more than three consultations before referral.19 Of those patients who were referred urgently, older patients were more likely to be diagnosed earlier than younger patients.23 However, when looking at endometrial cancer in isolation, older patients were more likely to be diagnosed with late-stage disease.15
Three studies demonstrated that rurality and distance from health care increased delay.14,20,24
Symptoms and symptom knowledge
Patients were shown to lack knowledge of the symptoms of ovarian, cervical, and endometrial cancer.25–27
Abnormal vaginal bleeding is considered differently at different stages in life. Two authors demonstrated that vaginal bleeding symptoms led to less delay than vague or gastrointestinal symptoms.12,28 Patient delay was greater in cervical cancer than in endometrial cancer because bleeding was less likely to be considered as a symptom of illness in premenopausal women.29
Seibaek et al 15 suggested that, although patients experience ‘bodily sensations’ such as abdominal distension or pain, it is organisational, cultural, and social factors that determine whether these ‘sensations’ are then interpreted as symptoms that lead to health-seeking behaviour. Many women will put these ‘sensations’ down to menopause or a non-gynaecological cause.
Presentation to primary care
Less delay was seen in women who undergo regular screening.12,20 Consulting with more than one GP before diagnosis has been linked to later disease stage.14
The International Cancer Benchmarking Partnership examined the effect of cancer awareness and beliefs on cancer survival in different countries. It found that the UK had the ‘highest mean barriers to symptomatic presentation’, for example, embarrassment and worry about what the doctor might find, when compared with other high-income countries.30
Doctor factors
Patient demographics
GPs in Denmark were less likely to delay referring women with higher SES.17 In a systematic review, Macleod et al 12 found that lower educational status was associated with referral delay. Three articles found that increasing patient age increased delay,15,29,31 although Robinson et al 16 found delay was greater if the patient was younger; this was related to menstrual status. Marital status was found not to affect referral delay.7 Rurality was associated with delay in one article.16
Symptoms
Non-specific, atypical, and gastrointestinal symptoms are more likely to be associated with delay.12,14,19,25,28,32 Doctor failure to appreciate the significance of symptoms, especially postcoital bleeding, led to longer delays in women diagnosed with cervical cancer, whereas older women with postmenopausal bleeding had shorter delay.33 Jensen et al 34 explored the effect of ‘suboptimal clinical decisions’ and found that endometrial cancer was least likely to have involved suboptimal clinical decisions, whereas cases involving ovarian cancer and non-alarm symptoms were most likely to involve this deviation in quality. Non-investigation of symptoms, including postmenopausal bleeding, is associated with increased delay in diagnosis.26,35 Failing to consider cancer as a possible diagnosis leads to diagnostic delay.33,36
Misdiagnosis, either through treating patients symptomatically or by relating symptoms to other conditions, can also lead to referral and diagnostic delay,12,32,35 as can comorbidities.14,36
Referral process
Not being referred to gynaecology,35,37 non-urgent referral,26,35 and referring without notifying a suspicion of cancer on the referral12 were all associated with diagnostic delay.
In patients with multiple consultations before referral, a lack of follow-up led to delay.27,35 Poor communication can lead to patients not re-presenting with persistent symptoms or follow-up.35,38
Poor communication can affect a GP’s ability to make a differential diagnosis, which can cause delay.34,35 For patients referred for investigations by their GP, false-negative results led to delayed diagnosis.34
The effect of pelvic examination was investigated. One article demonstrated no association between pelvic examination and diagnostic delay, whereas three authors demonstrated diagnostic delay when no pelvic examination was performed.12,29,33 The effects of misinterpreting abnormal findings as normal was also highlighted.27
A study of the use of USCR guidelines demonstrated no survival difference in women with ovarian cancer.39 Jiwa et al 36 found that those who were referred urgently were diagnosed most quickly, although failure to satisfy all the criteria for urgent referral can lead to delay. In patients diagnosed with cervical cancer, there was evidence that guidelines were not being used.33
Further study of USCR guidelines has demonstrated that, when used, the median diagnostic interval for cervical and endometrial cancers was increased, although in referrals using National Institute for Health and Care Excellence symptoms for referral, diagnostic intervals decreased.40 However, this study excluded patients aged ≤40 years. Vandborg et al 29 found some association between lack of alarm symptoms and long delays of >90 days, with 39% of those diagnosed with gynaecological cancer consulting with non-alarm symptoms, although the study only involved small numbers. Ovarian cancer diagnosis was quicker if referrals were USCR referrals (regardless of specialty referred to) compared with those referred routinely.41
The primary–secondary care interface was highlighted by two authors who commented on the need for senior clinicians to screen referrals and the resulting delay from slow communication of test results.38,42 Waits between secondary care appointments lead to delay.19
System factors
Shorter system delays were seen in wealthy females and patients referred by GPs who did not see them routinely. Patients described as ‘less compliant’ and those who had a high alcohol intake had greater system delays, as did patients referred by a female GP.17
It has been suggested that the gatekeeper role performed by GPs delays diagnosis.30,37 Poor access to investigations, both actual and perceived, can lead to delay.12,21,36,37
DISCUSSION
Summary
Diagnostic delay in gynaecological cancer is multifaceted and complicated. However, this inductive narrative review has identified symptom type, symptom knowledge, symptom investigation, and primary–secondary care interface as the factors most associated with differences in diagnostic delay for patient, doctor, and system intervals as described by Aarhus.7
Analysis by themes can be limiting and there are some difficulties categorising patient, doctor, and system factors because of their interdependency: some subthemes are embedded in all three major themes. Patient age appears to be an important factor influencing patient and practitioner behaviour. The symptom type is important and an absence of alarm symptoms can lead to delay. Patients and GPs can lack symptom knowledge, which affects patients’ decisions to present and clinicians’ decision to investigate or refer. Non-investigation of symptoms or misdiagnosis can lead to non-urgent referral or referral to specialties other than gynaecology. Communication between GPs and patients and GPs and secondary care also has impact.
There was little evidence describing the effect of UK and Danish USCR guidelines. Of the 21 UK studies included in the review, 15 were conducted after the introduction of the guidelines. Misattribution of symptoms by GPs and suboptimal referral were identified before and after guideline introduction.27,33,41 All eight Danish studies were conducted after guidelines were introduced.
Strengths and limitations
This review is the first to examine the factors influencing patient and primary care intervals in the diagnostic pathway of gynaecological cancers. It has been conducted rigorously and provides a summary of the available evidence to inform complex interventions to reduce diagnostic delay.
There are some limitations. Despite a comprehensive systematic search strategy, a paucity of evidence was identified. Almost all studies were observational and of variable quality. The studies were heterogeneous, varying in terms of cancer type, research methods, and outcomes, with a focus on descriptive work rather than interventions. Variance in the definition of delay and in the healthcare systems investigated led to heterogeneity of patients and practitioners. The lack of common methodology does not permit definitive conclusions.
Comparison with existing literature
The general diagnostic delay themes identified, such as patient socioeconomic and educational status, symptom knowledge, and misdiagnosis, confirm those described previously by other authors,12,30,46,47 but this review is the first to examine factors specific to gynaecological cancer.
Implications for research and practice
This review has identified specific factors that influence patient and primary care diagnostic delay.
GPs can be misled by presenting symptoms; they should be alert to gastrointestinal symptoms and abnormal bleeding in premenopausal women, which can lead to misdiagnosis, lack of examination, and suboptimal referral. Another important factor in reducing delay is for GPs to have suspicion that the patient may have cancer. However, because GPs do not see cases of gynaecological cancer often, it is important to work out how they can differentiate between suspicious and non-suspicious vaginal bleeding or recognise the significance of gastrointestinal symptoms while minimising delay.
There is a need to understand why patients delay presenting and identify effective education. Pelvic examination appears to be an important factor in reducing delayed diagnosis; therefore, research might be useful to find out how to make it an acceptable procedure to patients in terms of physical and emotional comfort and to GPs in terms of time, chaperone availability, and skills. Communication is key; patients must be reassured that they are not wasting GPs’ time and to come back if symptoms persist or worsen.
Notes
Funding
This work was funded by an NHS Education for Scotland Clinical Academic Fellowship.
Ethical approval
Not applicable.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article: bjgp.org/letters
- Received June 14, 2018.
- Revision requested July 13, 2018.
- Accepted September 24, 2018.
- © British Journal of General Practice 2019
This article is Open Access: CC BY-NC 4.0 licence (http://creativecommons.org/licenses/by-nc/4.0/).
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

