Article Text

Abstract
Background: Failure to attend appointments compromises health service efficiency. Despite considerable interest in using novel technologies to improve attendance, evidence from rigorously conducted controlled studies is lacking.
Aim: To evaluate the effectiveness of texting appointment reminders to patients who persistently fail to attend appointments.
Design: Randomised controlled study.
Setting: Inner city general practice in Lothian, Scotland.
Method: We included 415 appointments made by patients (n = 173) who had failed to attend two or more routine appointments in the preceding year. Patients whose appointments were randomised to the intervention group received a text message reminder of the appointment. Patients whose appointments were in the control group received no reminder. Our primary outcome measure was non-attendance rates. We undertook an intention-to-treat analysis and multi-level analysis to take account of the lack of independence of the outcomes of repeated appointments for the same patient.
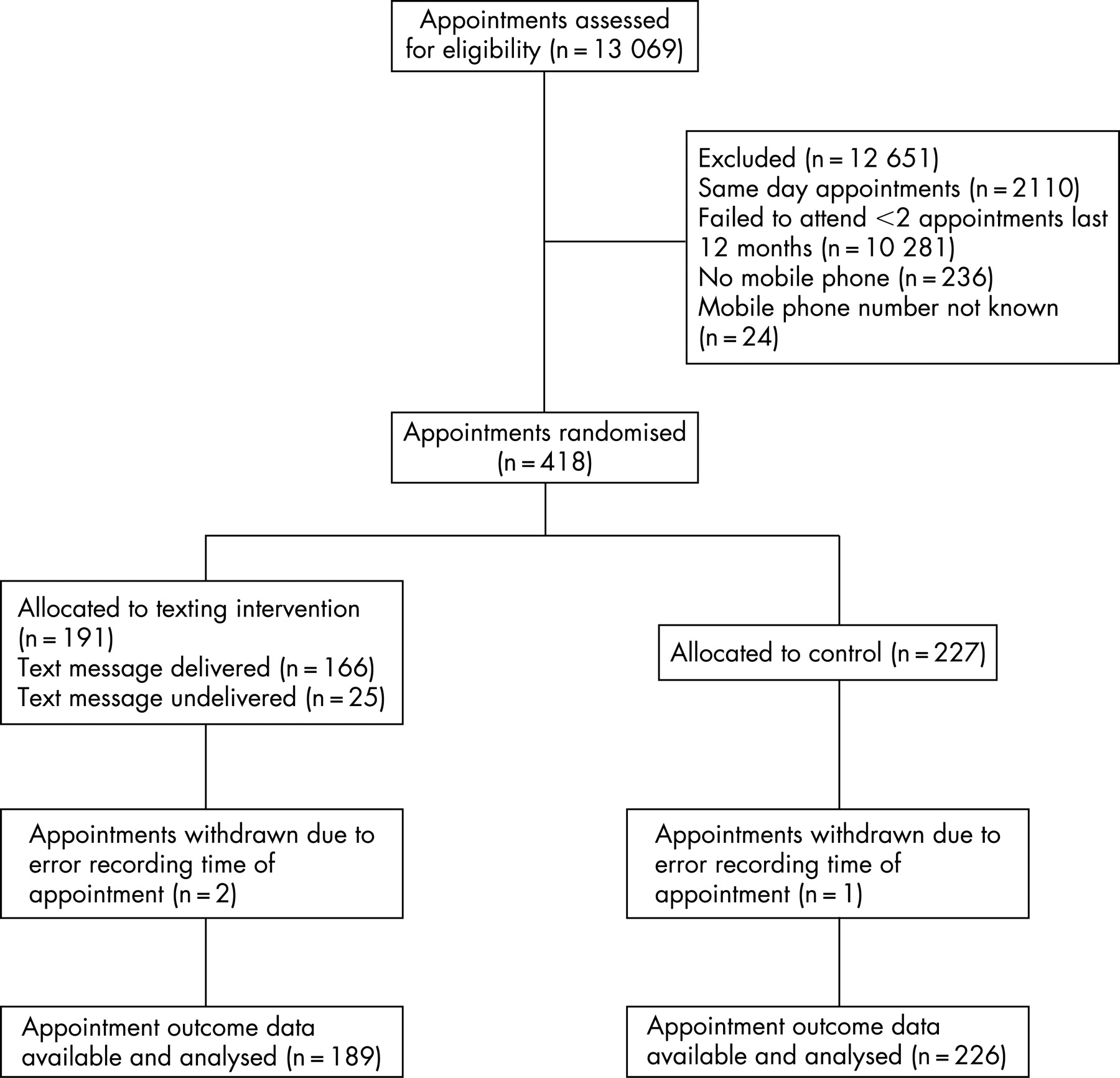
Results: Of the 418 appointments originally included in the study, three were excluded due to clerical error; 189 were randomised to the intervention group and 226 to the control group. Twenty-two appointments (12%) were not attended in the intervention group compared with 39 (17%) in the control group. A chi-square analysis, considering the outcome of appointments as independent from one another, gave a non-significant difference of 5% (95% CI of difference −1.1 to 12.3%, p = 0.13). Multilevel analysis applied to the binary outcome data on non-attendance gave an odds ratio for non-attendance in the intervention group compared with the control group of 0.63 (95% CI 0.36 to 1.1, p = 0.11).
Conclusion: Although the intervention showed promise, we failed to demonstrate significant reduction in non-attendance rates, as a result of texting appointment reminders to patients who persistently fail to attend their general practice appointments.
Statistics from Altmetric.com
Non-attendance rates for general practice and hospital outpatient appointments in Britain range from 5% to 34% across different specialties and between regions.12 This not only costs an estimated £185 million per annum in wasted appointments3 but also introduces significant inefficiency into a healthcare system that is under increasing pressure to achieve strict access targets.
Reasons for and patterns of non-attendance have not been well described. We do however know that patients who miss appointments tend to be young, have more psychological problems and be more socio-economically disadvantaged.4–6 Reasons for non-attendance appear to be complex and multi-factorial ranging from simple memory lapses—cited by patients in one study as the main reason for missing appointments7—to disillusionment with the way in which care is structured and delivered.89 Reminding patients of appointments by letter or telephone has previously proved effective in improving attendance,10 and patients have suggested that texting appointment reminders might similarly reduce those missed appointments associated with memory lapses.8
Despite interest in the use of novel technologies to improve attendance, evidence from rigorously conducted controlled studies is lacking.11 We report the results of a randomised controlled study assessing the effectiveness of texting appointment reminders to patients who repeatedly fail to attend their appointments in one inner-city general practice, with a practice population of 5200, in Lothian, Scotland.
METHODS
Participants
The computer records of all patients who failed to attend two or more routine doctor or nurse appointments in the preceding 12 months were flagged. These patients were considered to be the most likely to fail to attend subsequent appointments. All appointments made by these patients between August 2004 and February 2005 other than those made on the day of the appointment were eligible to be included in the study. Appointments made by patients with no mobile phone or who were unable to provide a mobile telephone number were subsequently excluded.
Intervention
The intervention comprised a text message reminder of the appointment sent between 08:00 and 09:00 on the morning preceding afternoon appointments and between 16:00 and 17:00 on the afternoon preceding morning appointments. Reminders for Monday morning appointments were sent on Friday afternoon. The text stated: “You have an appointment at (name of practice) (today/tomorrow) at (time). Please call (number) if you can’t make it.” Patients whose appointments were in the control group received no reminder.
Procedures
When an eligible patient made an appointment, the receptionist booking the appointment recorded it onto a prepiloted study diary sheet. Enquiry was also made as to whether the patient had a mobile phone, and if so, the mobile telephone number was recorded next to the appointment on the diary sheet. Randomisation of appointments took place between 08:00 and 09:00 on the morning preceding afternoon appointments and between 16:00 and 17:00 on the afternoon preceding morning appointments. Text-message reminders were sent immediately after randomisation to patients whose appointments were in the intervention group. Texts were sent from a PC via http://www.vodafone.net. Non-delivery of texts was reported via this system.
Randomisation
Appointments with associated mobile phone numbers were randomly allocated to one of the two groups by means of a random sequence of labels contained in sealed opaque numbered envelopes. One of two trained designated receptionists randomised each appointment by sequentially opening the sealed envelopes and allocating the appointment to the intervention group or the control group as indicated. The randomisation sequence was based on a table of random numbers.
Outcome
We defined the primary outcome measure as rates of non-attendance. We examined the appointment histories of participating patients within the practice computer record to determine whether each appointment was attended, not attended or cancelled. The data were extracted by KF and independently verified by the practice computer manager. Appointments were considered cancelled if patients notified the practice that they were unable to attend at any point up to the time of their appointment.
Sample size
We assumed a non-attendance rate of 15% in the control group.1 We considered that a 10% absolute reduction in non-attendance rates was organisationally important. With equal numbers of appointments in the intervention and control groups, we estimated using EpiInfo that a sample size of 414 appointments for the intervention and control groups combined would give 90% power to detect this, at the 5% significance level (two-tailed test).
Statistical analysis
We undertook a straightforward chi-square analysis to test the null hypothesis that there was no difference between the number of appointments not attended in the intervention and control groups.
To take account of the lack of independence of outcomes of repeated appointments for the same patient, we also undertook a multi-level analysis using the logistic model in MLwiN, with each non-attendance derived from a binomial probability which depended on both the randomised intervention and a random effect for patient.
RESULTS
A total of 418 appointments were eligible for inclusion in the study. There were 191 appointments in the intervention group and 227 appointments in the control group. However, three appointments (two in the intervention group and one in the control group) had to be excluded due to incorrect recording of the date of the appointment on the study diary sheet leaving 189 in the intervention group and 226 in the control group. These 415 appointments were made by 172 individual patients. Figure 1 shows the flow of appointments through the study. Table 1 shows the characteristics of the patients whose appointments were included in the study. Table 2 shows the frequency distribution of numbers of appointments per patient.
{kind=link}
Main findings
Table 3 shows the results for appointment outcomes in the intention-to-treat analysis. The non-attendance rate was higher in the control group (17.0%) than in the intervention group (11.7%), giving a risk difference of 5.3% (95% CI −1.1 to 12.3%), but this difference did not reach statistical significance (p = 0.13).
A multilevel analysis applied to the binary outcome data on non-attendance gave an odds ratio for non-attendance in the intervention group compared with the control group of 0.63 (95% CI 0.36 to 1.11). Again, this did not reach statistical significance (p = 0.11).
Of the 80 appointments cancelled by patients (41 in the intervention group and 39 in the control group), 55 (69%) were re-used (29 in the intervention group and 26 in the control group, respectively)
Adverse events
There were no adverse events during the study period.
DISCUSSION
Summary of main findings
To our knowledge, this is the first randomised controlled evaluation of the effectiveness of texting appointment reminders to patients. The results of this study failed to demonstrate that texting appointment reminders to patients who repeatedly do not attend their general practice appointments significantly reduces non-attendance rates. However, the intervention did show some promise: the point estimate for the effect of texting was a 5% absolute reduction in non-attendance; and the upper limit of the 95% confidence interval suggests that receiving a text message appointment reminder has the potential to reduce non-attendance rates among patients in this group by up to two-thirds.
Strengths and limitations of the study
The study was conducted in an everyday practice setting. The study procedures were pragmatic and easily incorporated into the routine reception and administrative duties of practice staff confirming the feasibility of the intervention. The costs of the study were small, less than £0.10 per text and around 10 min of receptionist time per day.
However, this was a single-centre study, which limits the generalisability of our findings to other settings. Furthermore, although 415 appointments were included in the study, these were made by only 172 patients, 103 of whom had more than one appointment included in the study. This clustering of data within patients was not accounted for in our original parallel group study design. We therefore undertook a multi-level analysis of the data to take account of the possibility that the outcomes of patients’ second and subsequent appointments were not entirely independent of their earlier experiences in the study. This will have resulted in some loss of power, increasing the risk of Type II errors.
A further limitation of the pragmatic study design was that the timing of the intervention was not the same for all appointments; reminders for Monday morning appointments were sent the previous Friday afternoon. It is conceivable that the timing of the reminder influenced its effect, but the study was underpowered to investigate this issue further.
Our work has other important limitations. Conceptually, it regards non-attendance as problematic. This perspective is predicated on the perception that non-attendance at appointments is responsible for avoidable inefficiencies in the healthcare system and is reflected in professionals’ negative views of and attitudes towards patients who fail to attend. However, missed appointments, if not the patients who miss them, are not always seen negatively by doctors, as they provide the opportunity for them to “catch up” and run to time or spend more time with other patients.12 This raises the prospect that, even if found to be effective, implementation of strategies to reduce non-attendance rates may founder because of professional ambivalence about missed appointments.
This study also regards non-attendance in isolation rather than as one element of a complex system that determines access to healthcare and which interacts with other elements of that system. Change in one element of the system such as texting appointment reminders is likely to impact upon other elements including the subsequent behaviour of patients and professionals. For example, we do not know whether an intervention such as this one which potentially shifts part of the responsibility for ensuring attendance at appointments from the patient to the healthcare system might lead to decreased patient self-efficacy in other aspects of their health-related behaviour. Potential effects such as this were unevaluated in this study.
Comparison with other studies and interpretation of our findings
The negative findings in this study are not consistent with the positive results of other intervention studies in which patients were prompted to attend appointments through the use of letter or telephone reminders.101314 However, we believe that texting appointment reminders shows promise, and there is scope for the intervention to be refined, which could possibly increase its effectiveness. We adopted a low and absolute criterion of failure to attend two appointments in the preceding 12 months for inclusion of a patient’s appointment in the study. This meant that patients whose appointments were included in the study included many who frequently attended and for whom the two non-attended appointments in the preceding 12 months represented a small proportion of appointments made. Additionally, we included patients of all ages who had mobile telephones despite the possible text messaging naïvety of many older patients. Also, we powered the study to detect a 10% reduction in non-attendance rates which we considered would be organisationally significant for the practice. In retrospect, we think a smaller reduction, for example 5%, might have been important to detect and of interest to policy makers and the NHS as a whole.
Implications for future research or practice
Despite the negative statistical outcome of this study, texting appointment reminders to patients who repeatedly fail to attend their general practice appointments may still have the potential to reduce non-attendance rates within particular patient groups, and can be incorporated relatively easily and safely into routine care. A larger multi-centre study is needed to provide a better estimate of the effect of the texting intervention and of its cost-effectiveness. Future research also needs to focus on who might benefit most from the intervention and, if found to be effective, the best time for the intervention relative to the appointment and whether any positive effect is sustained over time; it is also important to investigate other potential indirect and perhaps unanticipated consequences on consulting behaviour of incorporating such a strategy into routine practice.
How this fits in
Many patients fail to attend scheduled appointments in primary care, compromising the efficiency of the health service.
Despite considerable interest in the use of new technologies to facilitate access to care, rigorous evidence on their effectiveness in improving attendance is lacking.
Texting appointment reminders to patients who repeatedly fail to attend their primary care appointments may not significantly reduce non-attendance rates.
Acknowledgments
We are greatly indebted to the practice receptionists and administrative staff who incorporated the study procedures into their daily work and without whom the study would not have been possible. We wish to thank Rob Elton, Consultant Statistician, for his statistical advice and assistance with analysis, and referees of earlier versions of this paper for their constructive comments.
REFERENCES
Footnotes
Funding: Lothian and Borders Primary Care Research Network.
Competing interests: None.
Ethics approval: Lothian Local Research Ethics Committee granted approval for the study. The committee agreed that informed consent from patients to include their appointments in the study was not necessary. REC reference number 04/S1101/7.