


Abstract
Background In Taiwan, older veterans typically match the characteristics of a high prevalence of inadequate health literacy, which is a major barrier to effective communication in delivering proper health care. A good physician–patient relationship increases patients’ trust and willingness to communicate, so an awareness of the factors that influence this relationship could improve it over time and enhance patients’ health.
Aim To explore factors related to the physician–patient relationship among older veterans with inadequate health literacy in Taiwan.
Design and setting Observational study in veterans’ homes.
Method Data were collected using self-report questionnaires in face-to-face interviews. Patients with a Test of Functional Health Literacy in Adults score <60 (defined as inadequate health literacy) were recruited. Demographic characteristics, the Geriatric Depression Scale–Short Form, Multidimensional Health Locus of Control, and Perceived Involvement in Care Scales were used to identify related factors. Multiple regression and bootstrapping were used for data analyses.
Results A total of 256 older individuals were defined as having inadequate health literacy. Patients’ perceived involvement in health care partially mediated the relationship between Health Locus of Control and the physician–patient relationship. Perceived Involvement in Care, depression score, and Health Locus of Control were predictors of the physician–patient relationship.
Conclusion Older patients with inadequate health literacy had difficulty becoming actively involved in health care. The GP is in an ideal position to become a key person in helping such patients become involved in health care, and appropriately treating their depression may improve the physician–patient relationship.
INTRODUCTION
The physician–patient relationship is integral to patient-centred medical care. A good physician–patient relationship increases adherence to treatment recommendations, enhances continuing care, and promotes patient satisfaction with health care and self-reported health.1–3
The physician–patient relationship is important in healthcare services provided to older individuals with chronic diseases or complex health problems, especially those with inadequate health literacy. Inadequate health literacy is defined as a limited capacity to obtain and understand basic health information and the services needed to make appropriate decisions.4 A national survey of Taiwanese adults, using the Mandarin Health Literacy Scale, revealed that 53.2% of older people had inadequate health literacy.5 Inadequate health literacy is a cause of communication problems, as it embarrasses patients and limits their understanding of information given by healthcare providers, leading to worsening disease control and health status.6–8 Older patients with inadequate health literacy present a great barrier to the delivery of proper health care. They may not disclose their limitations to physicians because of feelings of shame.9 Lacking adequate literacy skills and hiding this inadequacy from physicians creates a vicious circle. The establishment of a good physician–patient relationship, which increases patients’ trust and willingness to communicate, can break the circle.10 Understanding the factors that influence the physician–patient relationship may assist healthcare professionals in identifying patients who have a poor relationship in this regard. However, little is known about the factors influencing the physician–patient relationship among older individuals with inadequate health literacy.
Inadequate health literacy is known to be highly prevalent among males aged >60 years with low educational attainment.11,12 In Taiwan, a special group of older individuals are the war veterans who fought in World War II in mainland China in their youth and followed the government of the Republic of China in its move to Taiwan in 1949; they account for almost 30% of the Taiwanese male older population.13,14 They typically match the above three characteristics and most of them frequently need to contact healthcare professionals about chronic diseases.13 The older veterans in this study were chosen because this population is more likely to have inadequate health literacy.
The aim of this study was to identify the factors affecting the physician–patient relationship among older Taiwanese veterans with inadequate health literacy. An awareness of such factors may help improve this relationship and enhance the health status of older people with inadequate health literacy.
How this fits in
Older patients with low educational attainment have a high prevalence of inadequate health literacy, which is a significant communication barrier to healthcare providers in delivering proper health care. Lacking adequate literacy skills and hiding this fact from physicians through feelings of shame creates a vicious circle that can be broken with the establishment of a good physician–patient relationship. If physicians can help such patients become involved in health care, it will directly improve the physician–patient relationship and also partially mediate the effect of health locus of control on that relationship.
METHOD
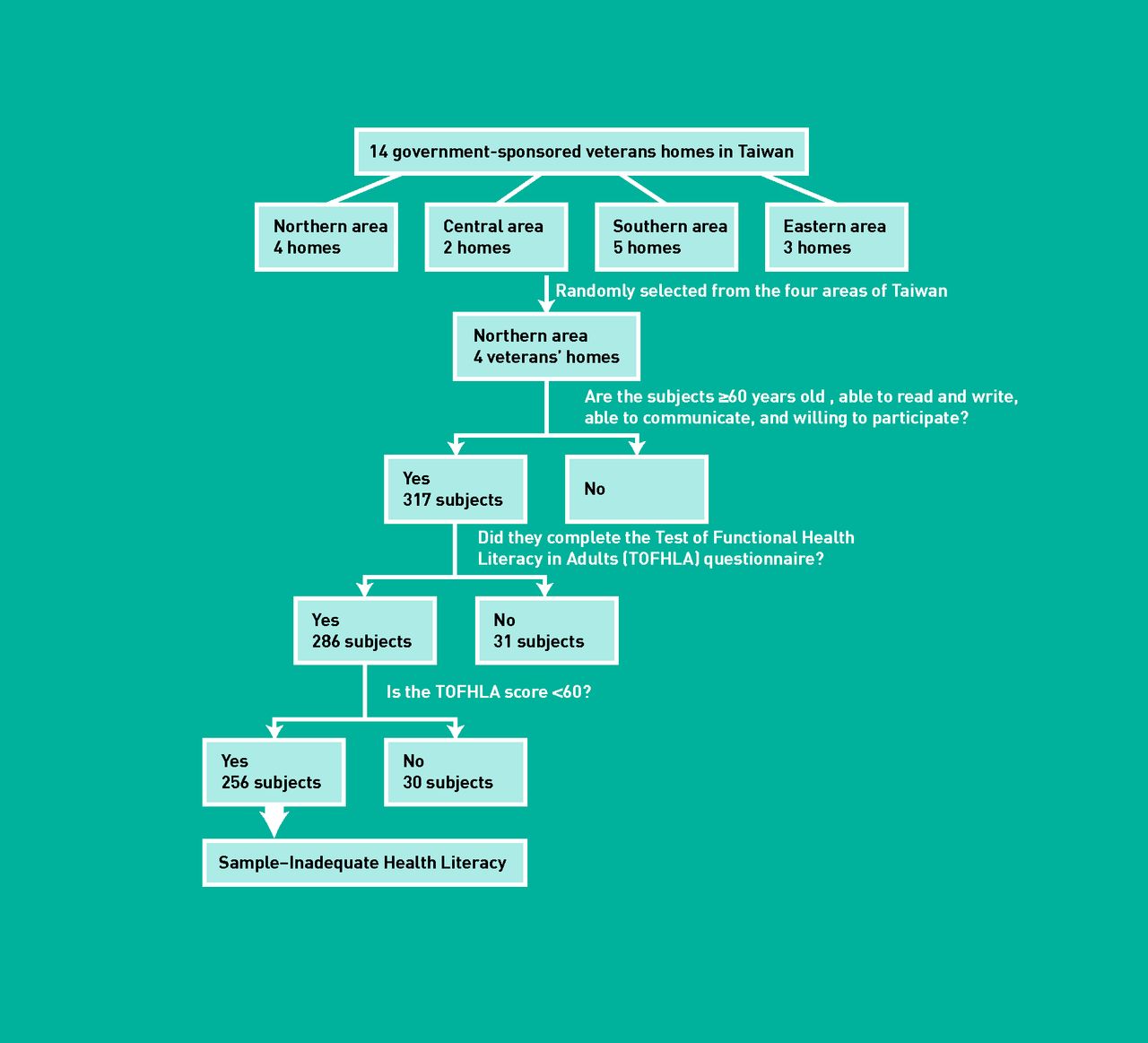
In this observational study, data were collected by face-to-face interviews conducted between January 2010 and March 2011. Participants were recruited from four veterans’ homes in North Taiwan, which was randomly selected from four areas of Taiwan. The scheme of recruiting the study sample is shown in Figure 1. Inclusion criteria were:
having inadequate health literacy, defined as a Test of Functional Health Literacy in Adults (TOFHLA) score <60 (TOFHLA has been translated into Chinese and demonstrated to be a reliable, valid instrument suitable for use in Taiwan);15–17
≥60 years old;
able to communicate with data collectors;
able to read and write; and
willing to participate in the study.
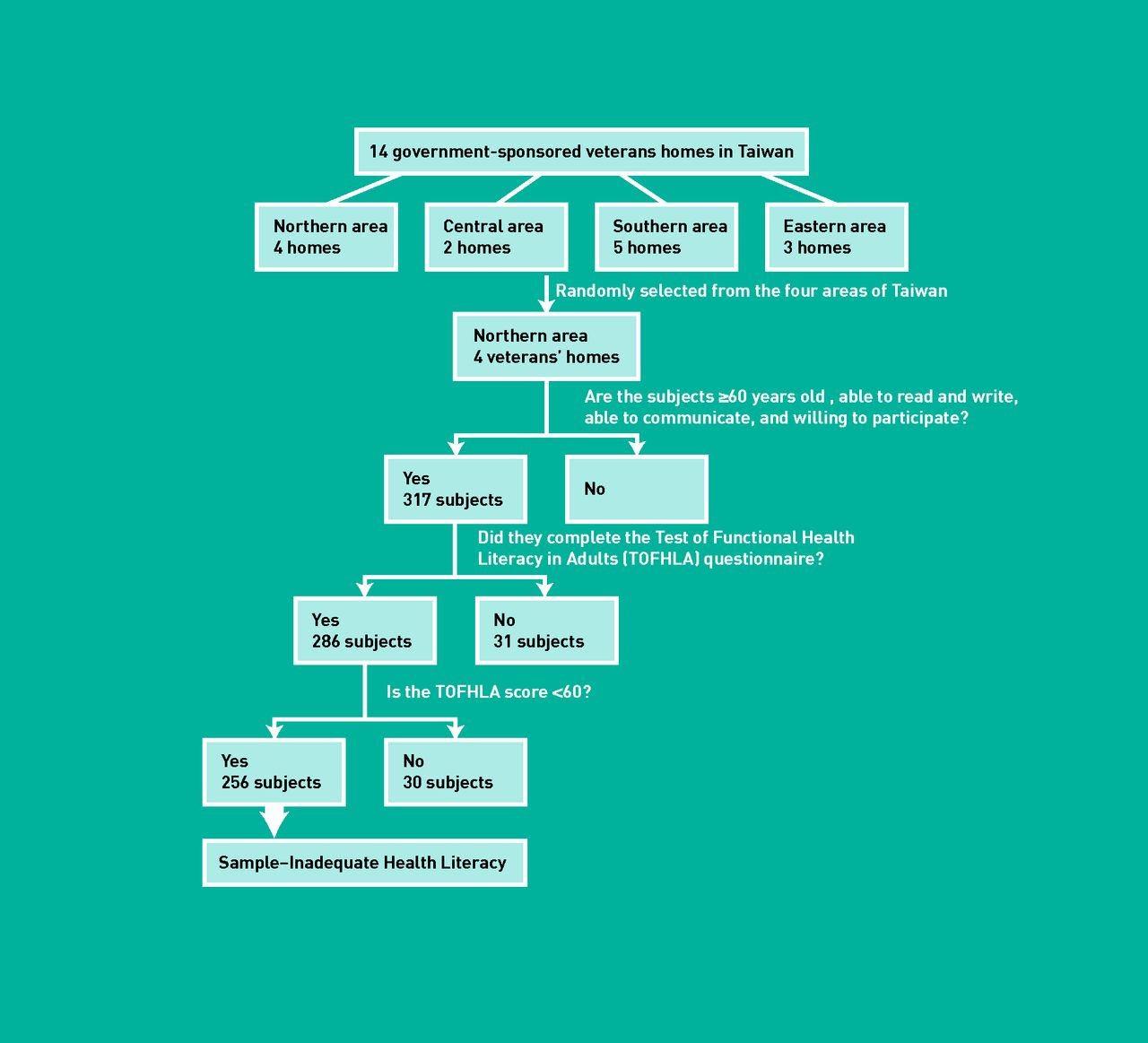
Sampling procedure.
A written explanation was provided to all participants and letters of informed consent to take part in the study were obtained. A total of 256 individuals were identified as the study sample.
Data collection
Data were collected using self-report questionnaires in face-to-face interviews. Information on age, marital status, education level, and economic status was obtained. Comorbidity was measured using the Charlson Comorbidity Index (CCI); a higher score indicates more severe comorbidity.18
A brief, validated instrument, the Patient–Doctor Relationship Questionnaire (PDRQ), was used to assess the physician–patient relationship from the patient’s perspective.19,20 It contains 9 items that assess the physician–patient relationship using a five-point Likert scale. The PDRQ does not have a threshold. Higher scores indicate a more helpful and positive attitude of the physician as perceived by the patient.
The Chinese version of the Geriatric Depression Scale—Short Form (GDS–SF) was used to measure depression status. It has been demonstrated to be a sensitive, reliable, and valid instrument that is suitable for screening depression in Taiwan.21,22 It includes 15 dichotomous questions, with a final score ranging from 0 to 15. Patients with a score ≥6 are considered to be depressed.23
The Multidimensional Health Locus of Control (HLC) scale was used to evaluate patients’ health belief about the location of controlling forces in their lives.24 It contains three subscales that are independent of each other: Internality HLC (IHLC); Powerful others externality HLC (PHLC); and Chance externality HLC (CHLC). Each item is answered on a 6-point Likert scale; a higher score indicates a higher orientation for that dimension.
The 13-item Perceived Involvement in Care Scale (PICS) was used to measure patients’ involvement in health care.25 The PICS has a relatively high level of internal consistency and contains three subscales: perceived doctor facilitation of patient involvement (doctor facilitation [DF]), perceived level of information exchange between doctor and patient (patient–doctor information exchange [PI]), and perceived level of patient participation in medical decision making (patient decision making [PDM]).25,26 The scale is rated on a dichotomous score. Higher scores indicate a greater degree of perceived patient activity and involvement.
Data analysis
Data were analysed using SPSS (version 18.0) for Windows. Statistical analysis determined that the dependent variable of the physician–patient relationship met the assumption of normal distribution. First, univariate analyses were used to identify factors associated with the physician–patient relationship. Then, a multiple regression model was used to study the independent predictors of the physician–patient relationship. At this stage, owing to the various degrees of interrelationships among the demographic characteristics, a propensity score was used to make adjustments;27 the score was obtained from a logistic regression model that examined the impact of potentially confounding variables (for example, age, marital status, educational level, economic status, CCI) on the physician–patient relationship. This method uses a weighted analysis, which directly compares the means marginalised over the confounders to yield unbiased estimates of the physician–patient relationship. Accordingly, in the multiple regression, the propensity score was added as a covariate. Bootstrapping was used as it is the most powerful and appropriate method of testing indirect effects under most conditions;28 it was applied to assess potential mediators of the relationship between predictors and the physician–patient relationship. Results were interpreted with caution, owing to the risk of false positives through multiple testing. All statistical analyses were two tailed, and results were considered significant at P<0.05.
RESULTS
All 256 veterans were male (mean age 83 years). About half had never married, two-thirds had less than 9 years of schooling, less than 10% had expenditures that exceeded their incomes, and nearly half had no comorbidities identified by the CCI (Table 1).
Distribution of veterans’ characteristics, depression score, multidimensional health locus of control, and perceived involvement with care and their association with the physician–patient relationship (n = 256)
The PDRQ score ranged from 9 to 45 (mean = 34.3; standard deviation [SD] ≈5.8). Results showed that lack of sufficient time and communication with the doctor were unsatisfactory aspects of the physician–patient relationship (Table 2). The GDS–SF score ranged from 0 to 14. The mean IHLC score was higher than that for the PHLC; the CHLC score was the lowest. For the three PICS subscales, the mean DF score was the highest and the PDM score the lowest (Table 1).
Mean and standard deviation of items in the Patient–Doctor Relationship Questionnaire (PDRQ) (n = 256)
Demographic variables such as age, marital status, and education level were not associated with the physician–patient relationship (Table 1). Veterans with higher IHLC and PHLC scores had a better physician–patient relationship. Regarding depression, veterans with a GDS–SF score ≥6 had a worse physician–patient relationship. A significant correlation was found between the PICS score and the physician–patient relationship. Furthermore, the PICS score partially mediated the effect of the HLC on the physician–patient relationship (Figure 2).

{kind=link}
{kind=link}
Perceived involvement in care partially mediates the relationship between Health Locus of Control and physician–patient relationship (PPR). Adj = adjusted. β = standardised coefficient.aP<0.05; bP<0.001.
Four variables, the PICS, IHLC, PHLC, and depression scores, accounted for 23.2% of the total variance in the physician–patient relationship (Table 3). Among the three PICS subscales, the DF and PI were significantly and positively correlated with the physician–patient relationship but the PDM was not. Further analysis identified the perceived level of DF as the most important predictor of the physician–patient relationship among study participants.
Multiple regression analysis of factors affecting the physician–patient relationship
DISCUSSION
Summary
Factors affecting the physician–patient relationship were patients’ perceived level of involvement in health care, perceived level of doctor facilitation in health care, depression score, and HLC. Patients’ perceived involvement in care was a mediator between their HLC and the physician–patient relationship. The doctor plays an important role in helping older patients with inadequate health literacy become involved in the healthcare process.
Strengths and limitations
Strengths of the study are that participants had no cognitive deficits, sensory impairment, or communication difficulties. Potential confounders that influence physician–patient interactions were excluded. Data were collected in face-to-face interviews to ensure accuracy. Results were adjusted by a propensity score, to reduce the interrelationship between demographic characteristics and the physician–patient relationship.
However, there are some limitations. Ethically, it was not permissible to collect data from individuals who were unwilling to participate in the study, in order to test the non-response bias. There was no statistically significant difference between the demographic characteristics of the 31 individuals who did not complete the Test of Functional Health Literacy in Adults for various reasons (such as lack of time, patience, and interest) and the 286 individuals who completed it. There may have been potential selection bias in the written study information and obtaining consent to participate. However, this probably did not have a significant effect on the results but simply meant that the study may not have included subjects at the lowest level of health literacy. Participants’ depression status was only evaluated by the GDS–SF, not clinically diagnosed by doctors. Finally, the cross-sectional design, non-probability sampling, and all-male group of participants limit the external generalisability of the findings. To remedy this, future research should recruit older females and individuals living in the community.
Comparison with existing literature
This study’s sample comprised 256 older veterans who were identified from among 286 individuals, almost 90% of whom had inadequate health literacy; a much higher percentage than is reported in previous studies; particular attention should therefore be paid to this population.5,11,15 These individuals have unique characteristics that may explain their high prevalence of inadequate health literacy: school-age experience of war, lack of proper education, and migration from mainland China.14 To meet the healthcare demands of veterans in Taiwan, a specific medical service system (veterans general hospitals, healthcare units in veterans homes, domiciliary centres) has developed over the past 50 years, governed by the Veterans Affairs Commission. It has served hundreds of thousands of veterans and become an important part of the country’s health services.29
It was found in this study that veterans’ demographic characteristics had no effect on the physician–patient relationship, which is in contrast to a previous study that reported that individuals with poor physician–patient relationships have no insurance, low income, or major economic concerns.1 The fact that the veterans in the present study lived in government-sponsored facilities, had national health insurance, and received government financial support for monthly expenses, and fewer than 10% had financial burdens, is a possible explanation for this discrepancy. Noyes et al indicated that the quality of the physician–patient relationship is related to patient dispositional variables not demographic variables.30 The present study found that participants’ IHLC and PHLC directly contributed to a positive perception of the physician–patient relationship. Patients with internal control orientation may be better able to face their health problems, and those with powerful others externality may place greater trust in their doctors.31,32 During the physician–patient interaction, a patient’s active attitude and trust can positively affect a doctor’s behaviour,33 possibly by creating positive feedback in the healthcare process and leading to a good physician–patient relationship. However, the HLC is a type of individual health belief, which may not be easily changed by health professionals’ education or interventions towards improving the physician–patient relationship.
Patient participation in medical care has emerged as an important factor in medical practice. The results of this study show that perceived involvement in care and the perceived level of DF had positive effects on the physician–patient relationship. Brody et al indicated that highly involved patients have a greater sense of control of their illness and a higher degree of satisfaction with their doctors.34 However, inadequate health literacy is a great barrier to the older patient becoming actively involved in health care.6 Patients’ perception that their doctor helped them to participate in the healthcare process has been found to directly increase patients’ level of understanding.25 The GP is in an ideal position to become a key person in helping older patients with inadequate health literacy to become more involved in their health care. The perceived level of involvement in health care can play a mediatory role with respect to the HLC and the physician–patient relationship. The mediating effect of a doctor encouraging patient involvement in health care is potentially a more modifiable factor than health belief. Creating a patient-centred approach and offering continued care, which is the concern of most GPs, promotes a good physician–patient relationship.35 Therefore, if GPs can help older patients with inadequate health literacy to seek health information, and read and follow written instructions (that is, become involved in health care), then this may be beneficial to the development of a good physician–patient relationship. When offering healthcare-related information to patients, GPs should check that patients are able to understand that information.
It was found that 32% of the study sample suffered from depression, as measured by the GDS–SF, which is 1.5–4.0 times the level found in studies of Taiwanese institutionalised male veterans.14,22 Several studies have demonstrated that older subjects with inadequate health literacy have a higher prevalence of depression than those with adequate health literacy.5 Therefore, the higher proportion of patients with depression in this study may be related to their inadequate health literacy. It was found that patients’ perceived depression had a negative effect on the physician–patient relationship. Depression status is a potentially modifiable factor that could be improved by clinical treatment. However, De Marco et al reported that the sensitivity of doctors in detecting patient-perceived depression was only 50%, and the specificity was 59%.36 In other words, there are gaps between doctors’ assessments of patients’ depression status and actual depression as perceived by patients. Therefore, evaluating patients’ depression in a clinical setting, and ensuring appropriate management, represent new challenges for healthcare providers.
Implications for practice and research
This study found a high prevalence of inadequate health literacy among older (>60 years) male veterans with low educational attainment. GPs who meet such individuals for the first time should consider their degree of health literacy. After identifying patients with inadequate health literacy, interventions should be made to improve the physician–patient relationship, paying particular attention to communication, patient understanding, and involving the patients in their own health care.
These findings provide useful information to GPs about what needs to be considered to establish a good relationship with older patients who have inadequate health literacy. As patient depression was found to be a barrier to establishing a good physician–patient relationship, it is suggested that the self-reported depression status of older patients should be integrated into routine history taking and be managed appropriately. An applicable instrument for assessing depression should be selected, otherwise the physician–patient relationship may be threatened.37 Helping patients with depression to become involved in health care can also help improve that depression.38 GPs should be encouraged to actively help older patients with inadequate health literacy become involved in the healthcare process, because patients’ perception of a positive attitude on the part of doctors may have a beneficial effect on the physician–patient relationship. GPs should strive to improve their relationships with patients in a timely manner, which would, in turn, increase their patients’ satisfaction and enhance their health status.
Acknowledgments
The authors thank the staff in the four veterans’ homes for their administrative support.
Notes
Funding
This study was supported by a grant from Taipei Veterans General Hospital, Taiwan (V99C1–046).
Ethical approval
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital (no. 201004023IC).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received March 8, 2012.
- Revision received June 21, 2012.
- Accepted December 4, 2012.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

