


Abstract
This study seeks to test the feasibility of vaccinating injecting drug users for hepatitis B in primary care and to identify predictors of poor immune response. Two hundred and seventy-five injecting drug users were identified from the case notes of a large general practice in an area of high multiple deprivation in northwest Edinburgh and, where appropriate, offered hepatitis B vaccination followed by a post-vaccination serological test. We concluded that hepatitis B vaccination of drug users in primary care is both feasible and effective. This study was unable to identify a group at risk of vaccine failure, however, it found post-vaccination serological testing to be problematic and potentially misleading. Therefore, we would not recommend its routine use in a primary care setting. Significantly, prolonged primary courses were not associated with reduced efficacy. The findings indicate that an appropriate vaccination schedule for primary care should be flexible to maximise compliance.
Introduction
HEPATITIS B infection remains a serious health problem and infection risk for injecting drug users. The sero-prevalence of hepatitis B virus among injecting drug users remains high, ranging from 20–70%, depending on the population surveyed. Hepatitis B outbreaks among drug users are occurring with an increasing incidence, and this is in spite of the availability of effective vaccines for more than 20 years.1 There are few reports or studies of how to effectively engage drug users in vaccination programmes and even less research concerning how well they respond to vaccination. This study addresses these issues from a primary care perspective.
The setting for this study was a general practice in north-west Edinburgh, serving a population of 10 000. It is located in an area of high multiple deprivation, with a high prevalence of drugs misuse and related problems. It is part of a wider study that has gained ethical approval from the Lothian Research Ethics Committee.
Method
An audit was initially carried out in 1998, which confirmed the very low level of vaccination uptake among injecting drug users.2 An attempt was then made to raise awareness concerning hepatitis B and its prevention among injecting drug users, to encourage bloodborne virus screening, and to actively promote hepatitis B vaccination.
Between 1998 and 2002 the case notes of all identified injecting drug users registered with the practice were regularly scrutinised and the following noted: the year of first injecting; HIV, hepatitis B and hepatitis C serological status; hepatitis C virus PCR (polymerase chain reaction) results; and hepatitis B vaccination status. A hepatitis B vaccination course was then offered, when appropriate, following a pro forma inserted in the notes detailing instructions. A recombinant 20 mcg vaccine was used, administered intramuscularly in the deltoid region. An attempt was made to follow the rapid 2-month schedule with a post-vaccination protective antibody to hepatitis B surface antigen (anti-HBs) serological test 1 month after course completion. Those with poor serological responses, defined as anti-HBs <10 mIU/ml using a microparticle enzyme immunoassay, were offered a booster dose.
The post-vaccination serological responses were recorded on a four-point scale based on cut-offs of 0, 10 and 100. Association with potential predictors was tested using χ2 tests for trend or Spearman rank correlation.
Results
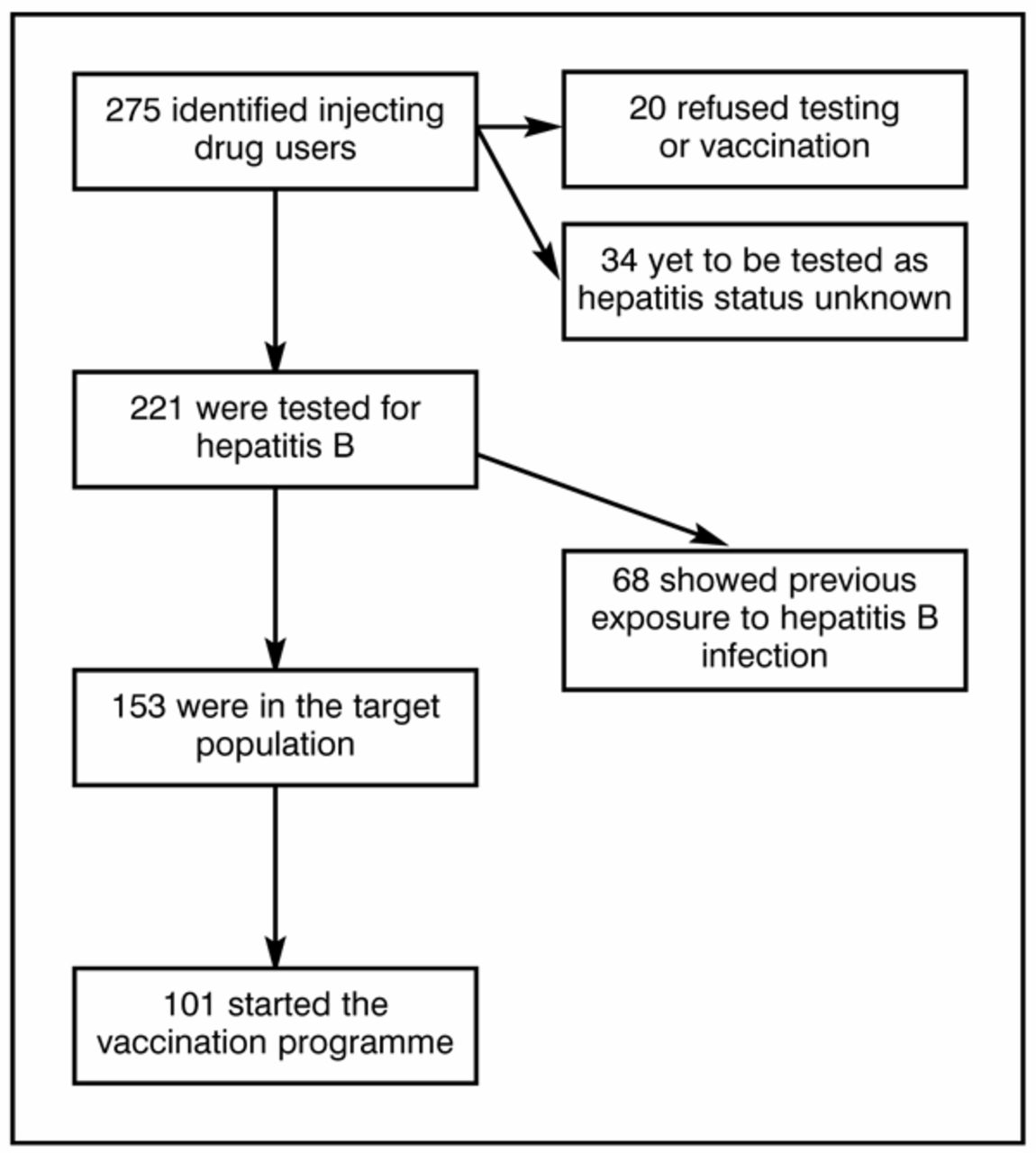
Two hundred and seventy-five injecting drug users were identified. Seven refused bloodborne virus screening and 13 refused any immunisations and were excluded from further analysis.
HOW THIS FITS IN
What do we know?
Injecting drug users are at high risk of hepatitis B infection. Vaccination coverage of this group is very poor and little is known about how to effectively engage drug users in vaccination programmes.
What does this paper add?
Hepatitis B vaccination of drug users in primary care is feasible and effective. Routine post-vaccination serological testing is problematic and not recommended on the basis of this study. Flexible scheduling is required to maximise compliance.
Of the 221 injecting drug users screened for hepatitis B, 68 (31%) showed past exposure, being either positive for core antibody or surface antigen. The sero-prevalence of hepatitis C and HIV antibodies were found to be 58% and 14%, respectively.
By the end of the study, 101 of the target population of 153 had started the vaccination programme (Figure 1). Of these, 74 had completed the primary course and had had a post-vaccination serological test. Seventeen individuals had received at least one booster, having had a poor immune response to the primary course, and, of these, 12 had had a post-booster serological test. Nineteen of the 31 hepatitis C-positive patients who completed the primary course had PCR results. The results of post-vaccination serological tests and association with potential predictors are summarised in Table 1.
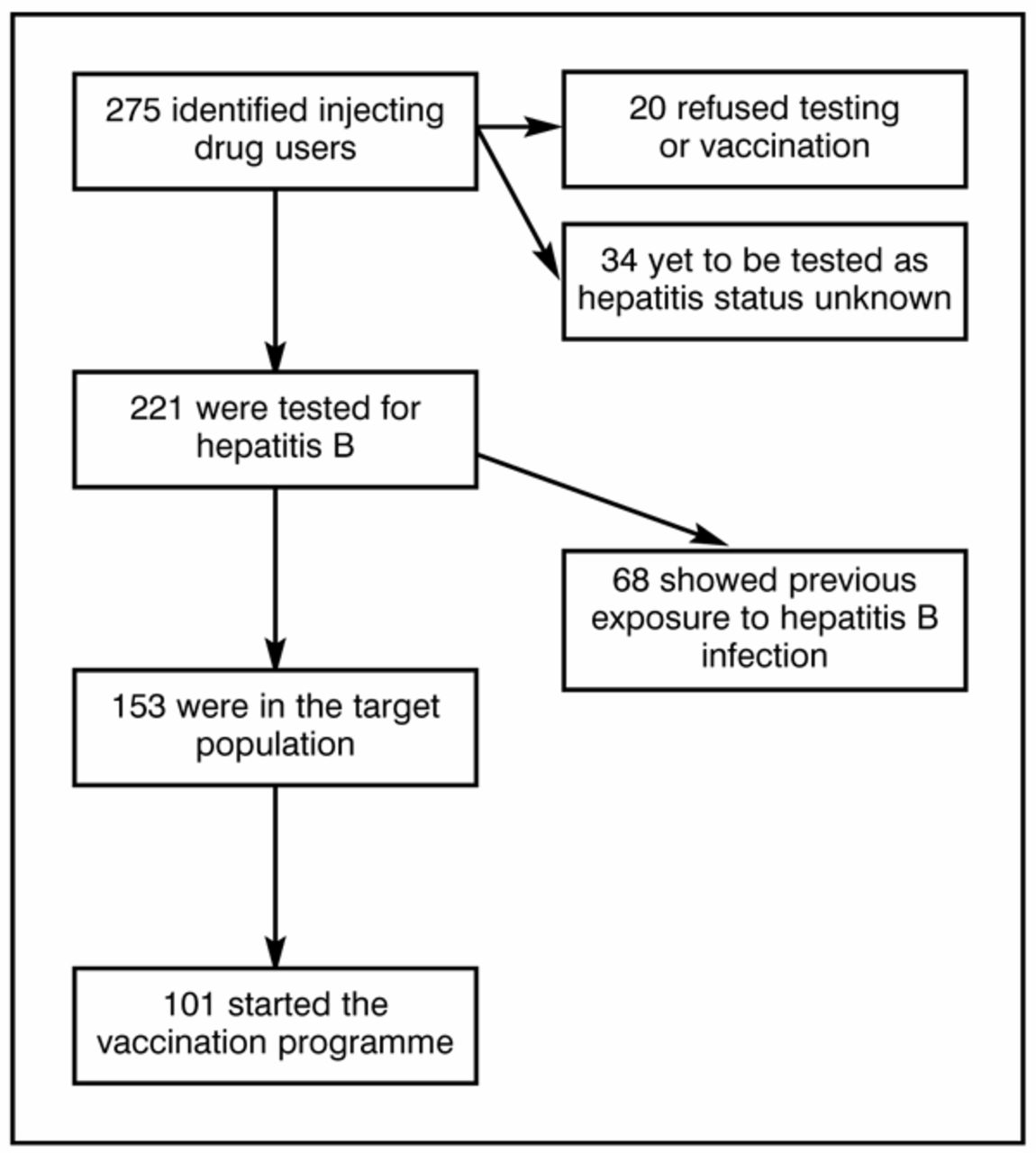
Systematic overview of the study.
Characteristics of patients according to serological response.
Forty-nine (66%) patients mounted a protective immune response of ≥10 mIU/ml to the primary course, although this rose to 55 (74%) patients after the 12 booster results were included.
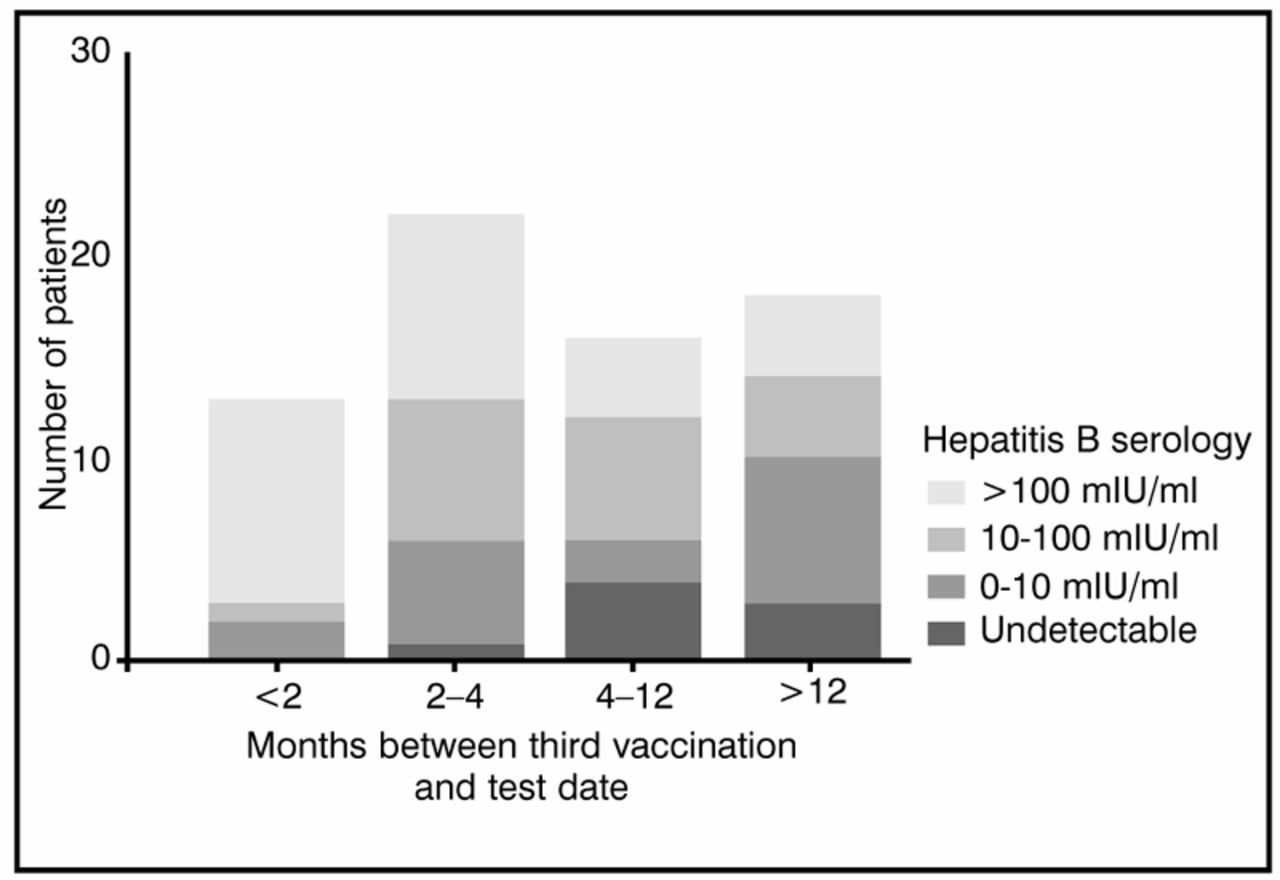
The only statistically significant predictor of poor primary immune response was the length of time between primary course completion and the post-vaccination serological test, with the longer the interval the worse the response (P<0.001) (Figure 2).

{kind=link}
{kind=link}
Immune response to vaccination by length of time from primary course completion to serological test.
Prolonged primary courses were not associated with poor responses, and in fact those lasting more than 1 year were associated with better immune responses (P = 0.024).
Other factors, such as HIV status, hepatitis C status, PCR positivity and sex, were found not to be significant. There were trends for worse response with increasing numbers of years of drug use and older age, but these were not statistically significant.
Of the 12 patients who received a booster and post-booster serology check, six initially had an undetectable antibody response to the primary course. Of these six, four had no detectable response to the booster and two showed a 10–100 mIU/ml antibody level response. Of the other six who received boosters, three showed responses >100 mIU/ml, one responded in the 10–100 mIU/ml range, and two in 0–10 mIU/ml range. Predictors of booster failure were hepatitis C positivity (P<0.01) and HIV positivity (P<0.01).
Discussion
This study shows that vaccinating injecting drug users against hepatitis B in a primary care setting, although not without its difficulties, is both feasible and effective. Much has been written concerning the failure to immunise injecting drug users against hepatitis B and the reluctance of specialist services to offer vaccinations.3,4 If this failure is to be addressed, then primary care, where the bulk of the medical care of drug users is provided, will have to play a significant role.
Over the period of the study the number of identified injecting drug users grew significantly from 145 in the year 2000 to 275 by 2002. Therefore, many of these new cases had not completed their primary courses or had post-vaccination serological tests by the end of the study. Including all patients in the study who had started the primary course gives a coverage of 66% (101/153) and this level compares favourably with other reported programmes among drug users.5 The increase in the number of new injecting drug users is likely to represent, in part, an increased vigilance on the part of the health workers in identifying at-risk individuals, but more significantly and worryingly it reflects the rise in local heroin use and injecting behaviour.
Drug users as a group are recognised as having multiple social, psychological and medical needs. This often leads them to have priorities in their health concerns that do not reflect the medical priorities of their healthcare providers. They are also a very mobile group, dropping in and out of treatment, moving areas, or having enforced periods of absence in prison. Thus, following a set treatment course or vaccination schedule can be problematic. In this context, it is of particular significance that prolonged primary courses were not found to reduce immune response to vaccination. In fact, the results show that when more than 1 year elapsed between the start and completion of the primary course, its efficacy was enhanced.
Box 1. Key messages.
Hepatitis B vaccination of drug users in primary care is both feasible and effective.
Flexible scheduling is required.
Routine post-vaccination serological testing is problematic and potentially misleading.
Prolonged primary courses do not reduce efficacy.
Hepatitis C infection was not found to be associated with poor immune response to vaccination.
The one statistically significant predictor of poor immune response to vaccination was the length of interval between primary course completion and serological testing. The timing of this test is crucial to the interpretation of a low result. Therefore, the late post-vaccination test that is low is potentially misleading, since it may not reflect the peak immune response that determines immune protection.6 Routine post-vaccination serological testing of drug users in primary care is not therefore recommended.
Certain groups who may be at particular risk of severe or chronic hepatitis B infection, such as hepatitis C or HIV infected individuals, could benefit from a timely post-vaccination serology check. Our results show that these groups are also at greater risk of booster failure. Therefore, if these groups show an initial inadequate response to the primary course, then a more immunogenic booster, such as an increased dose of vaccine or the new triple antigen vaccination (when commercially available), could be offered.
If post-vaccination serological responses are elicited, then an antibody level of >10 mIU/ml would be the appropriate target level to indicate protective immunity. The aim of vaccinating drug users is to prevent chronic carrier state or significant infection. Studies that have identified infections among vaccinated individuals have reported that when an immune response of >10 mIU/ml has been achieved, then only mild and transient infections have occurred, with no chronic carrier states.7
Interestingly, hepatitis C antibody positivity was not associated with a poorer response to primary vaccination, but was associated with a poorer response to the booster dose. There is mixed evidence in the literature concerning this, although a large recent study has identified hepatitis C infection as a significant factor in determining immune response.8 One might have thought that PCR positivity, as a marker of active infection, would have been a significant factor in determining immune response; however, our study failed to confirm this.
On the basis of this study we recommend that an appropriate vaccination schedule for primary care should be flexible and include a primary course of three vaccinations, timed to maximise compliance — perhaps to coincide with the issuing of monthly substitute prescriptions, or further apart — with a booster at 1 year or later. This is likely to offer protection rates of over 80%.
Acknowledgments
We would like to thank the partners and all staff at the Muirhead Medical Group for their support and help with this study and in particular Lorraine Copeland for her technical expertise and encouragement.
- Received July 4, 2003.
- Revision received September 23, 2003.
- Accepted December 23, 2003.
- © British Journal of General Practice, 2004.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

