


Abstract
The General Medical Services (GMS) contract has focused the attention of United Kingdom (UK) general practitioners (GPs) on the provision of high quality routine care for patients with chronic disease.1 The quality markers defined by the contract endorse the need for objective diagnosis and structured care recommended by the British Thoracic Society/Scottish Intercollegiate Guideline Network (BTS–SIGN) guideline for the management of asthma and the National Institute for Clinical Excellence (NICE) guideline on the management of chronic obstructive pulmonary disease (COPD).2,3 In this paper the key recommendations of these guidelines and their implementation in the pragmatic world of general practice are discussed, with specific focus on diagnosis, monitoring, management, self-management and delivery of care.
Diagnosis of asthma and COPD
Objective diagnosis of asthma
The key diagnostic feature of asthma is the variability of the symptoms, signs, and lung function. Practical hints for diagnosing asthma are shown in Box 1. Diagnosis can be considered and recorded as a three-stage process.
Box 1. Practical hints for ensuring an objective diagnosis of asthma.
Provision of simple written instructions may facilitate teaching during the course of a busy surgery or patients can be referred to an asthma-trained practice nurse
Patients should be asked to record the best of three peak flow readings each morning and evening and at times when they are symptomatic and when they feel well. Patients experiencing regular symptoms should be able to obtain sufficient readings over the course of a week to support or question a diagnosis
Variability of more than 20% is highly suggestive of asthma
Many of the patients with mild asthma in general practice will only demonstrate peak flow variability during times of exacerbations so that lack of 20% variability does not exclude the diagnosis. It should, however, lead to consideration of alternative diagnoses, especially if the patient was symptomatic at the time
Typical history
Variable symptoms of wheeze, shortness of breath, chest tightness and cough suggest a diagnosis of asthma, although some of the patients with mild asthma seen in primary care may have intermittent symptoms occurring only after exposure to an allergen or after a viral infection. Audible wheeze may only be present during exacerbations. A personal or family history of atopy adds weight to the diagnosis.
Objective tests
A peak flow is the most convenient test of lung function for the diagnosis of asthma. The demonstration of variability requires multiple readings recorded over a period of time to demonstrate diurnal variation, deterioration on exposure to a trigger or reversibility after treatment. An isolated normal peak flow carried out in the surgery does not exclude the diagnosis of asthma. Peak flow charting involves the patient in the diagnostic process and has the advantage of capturing objective evidence of variability at the time the patient has symptoms, allowing an assessment of the severity and frequency of symptoms. In addition the best peak flow can be established as a baseline for future management plans. Significant variability is defined as ≥20%, with a minimum change of 60 L/minute. Spirometry may also be used to demonstrate reversibility, but because of the variable nature of asthma, normal spirometry does not exclude the diagnosis.
Response to treatment
Failure to respond to a trial of as-thma treatment, such as inhaled steroids, should prompt reconsideration of the diagnosis.2 The differential diagnosis of adults with symptoms of cough and wheeze includes COPD, heart failure, bronchiectasis and hyperventilation.
Objective diagnosis of asthma in infants
Making a diagnosis in young children is more complex, both because objective tests of lung function are not feasible in routine practice and because of a growing awareness of the different phenotypes of asthma in infancy. Viral-associated wheeze is common in infancy, some will have asthma throughout childhood, a few will have lifelong asthma, and occasional children will have other more serious pathology.4 The three components of the diagnostic process — an appropriate history, objective evidence and a response to treatment — need to be modified for infants:
Persistent symptoms of cough and wheeze, especially in the presence of atopy, suggest asthma.
Wheeze, heard by a healthcare professional, should be noted in the patient's records as objective confirmation of the parent's description.
A documented trial of treatment (either with bronchodilators or a course of inhaled steroids) with relapse on withdrawal may be a useful strategy.5,6 A poor response suggests that asthma is unlikely and should prompt consideration of alternative causes of the child's symptoms.
Objective diagnosis of COPD
COPD is a chronic, slowly progressive disorder in which the airflow obstruction is fixed or only minimally reversible.3 In contrast with asthma, symptoms and signs develop insidiously and lung function deteriorates slowly over years. Other causes of productive cough and breathlessness, such as bronchiectasis, need to be considered in the differential diagnosis of chronic symptoms, while a rapid deterioration should prompt a search for other pathology, such as lung cancer or heart failure. Comorbidity is common, with other smoking-related and age-related diseases occurring in 40% of patients with COPD investigated after an acute exacerb-ation.7 For the primary care clinician the key distinction is often between asthma and COPD; a distinction that is made more complex as some patients with asthma develop irreversible remodelling and patients with COPD may have ‘some reversibility’.3 The diagnosis is suggested by the history and clarified with spirometry.
Typical history
A smoker, presenting with a history of slowly progressive, productive cough, wheeze, and shortness of breath, with an onset of troublesome symptoms after the age of 50 years suggests a diagnosis of COPD.
Spirometry
A consistently low peak flow with no variability in a smoker with typical symptoms may suggest COPD, but the objective diagnosis and assessment of severity requires spirometry.3,8 A FEV1 (forced expiratory volume in 1 second) <80% of predicted and a FEV1/FVC (forced vital capacity) ratio <70% confirms obstruction. Some patients with COPD will show significant reversibility (>15% and 200 ml increase in FEV1), but a substantial increase in FEV1 (more than 400 ml) suggests a diagnosis of asthma. Some key points for the provision of a spirometry service are given in Box 2.
Box 2. Spirometry: some practical points.
A range of reasonably priced spirometers ideal for use in primary care are readily available. They all require regular servicing and manufacturers' instructions for calibration should be followed
Adequate training, whether of respiratory nurses or healthcare assistants, is essential to ensure that satisfactory readings are obtained. Manufacturers of spirometers can provide technical training on the use of specific instruments and a range of suitable courses are available from respiratory training centres
Patients should be prepared for the procedure. They should be clinically stable and should not have used a short-acting bronchodilator for 6 hours, a long-acting bronchodilator for 12 hours or theophyllines for 24 hours
Spirometry takes time, particularly in the elderly with severe COPD who may need to rest for some minutes between blows
The recent NICE guideline recommends classification into mild, moderate and severe COPD as FEV1 falls below 80%, 50% or 30% of predicted, bringing UK practice into line with international guidelines.3,8 Although lung function is a good indicator of prognosis, it does not accurately reflect disab-ility and may underestimate the impact of the disease in some patients while overestimating it in others. In the UK the GMS contract has adopted a 70% threshold for implementing the quality markers for COPD on the basis that symptoms are relatively unlikely at higher levels of lung function.1
There is growing evidence that reversibility testing with bronchodilators and oral steroids do not predict their ther-apeutic value, which should be judged on the basis of clinical benefit.9 Demonstration of poor reversibility, however, is important for diagnostic purposes, principally to exclude the diagnosis of asthma.
Screening for COPD
The accelerated decline in lung function can be prevented if patients can be encouraged to stop smoking.10 It is therefore suggested that identifying patients with mild COPD, combined with intensive smoking cessation advice, could reduce the burden of COPD by preventing progression to severe, disabling disease.3 The practicability, effectiveness, and cost-effectiveness of screening for COPD needs to be evaluated in primary care before widespread adoption of this theoretical benefit can be recommended.11-12 Case finding has been explored as a practical approach to identifying patients at risk of COPD.13,14 The presence of a cough in a smoker has been proven to be the most useful marker, correlating better with the diagnosis of COPD than wheeze or shortness of breath.
An additional problem for detecting mild COPD is that a single reading cannot indicate the rate of decline of lung function.12 A normal FEV1 of 80% of predicted may represent a considerable loss of lung function if that patient's baseline was 120% of predicted.
Monitoring of asthma and COPD in general practice
Regular review of people with asthma
Regular review of people with asthma is associated with a reduced exacerbation rate and improved symptom control15 and is a recommendation of national and international guidelines.2,16
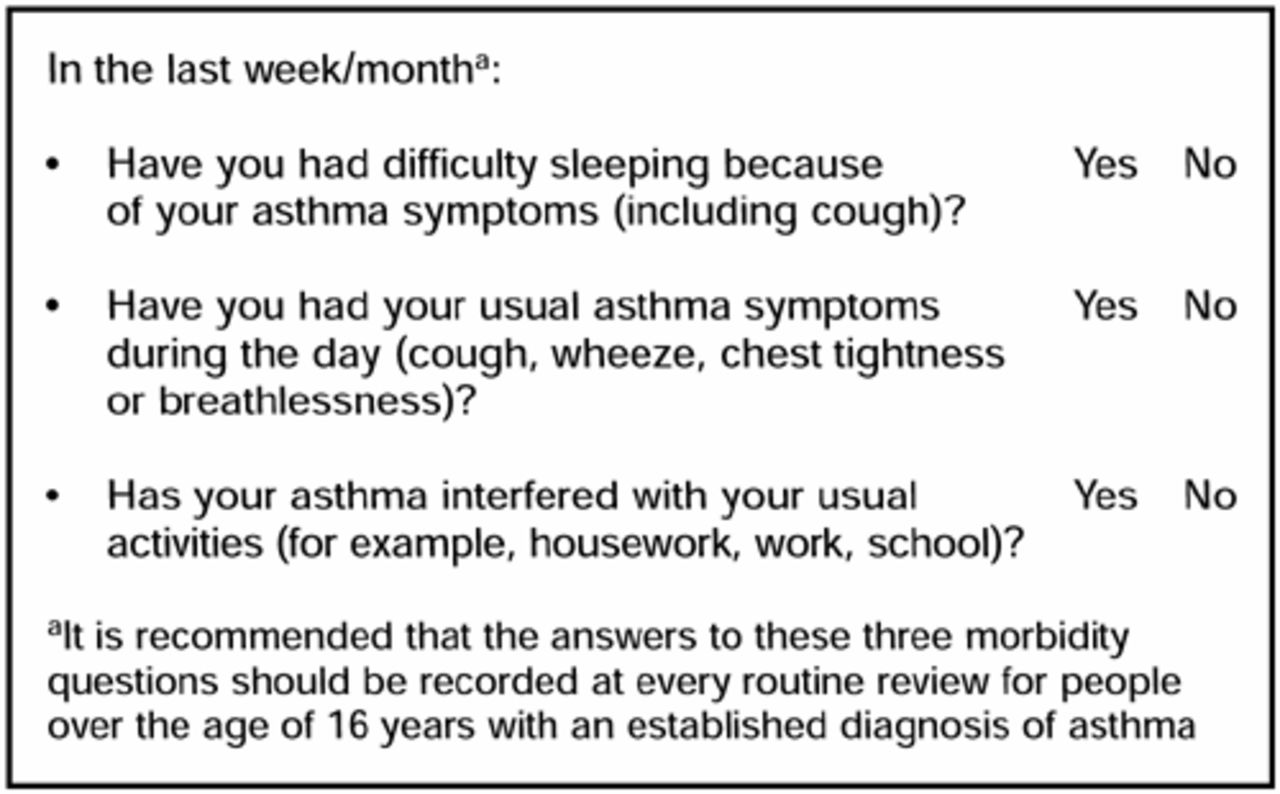
The content of a review will vary according to the needs of the individual patient, but a key component is the standardised recording of asthma control. Because of the var-iable nature of asthma, a peak flow undertaken in the clinic is of limited value in assessing asthma status. The simple morbidity score, promoted by the Royal College of Physicians17 (Figure 1), consists of three questions that could be used at every asthma review to monitor progress. Tools incorporating similar questions have been used successfully to screen for those with more severe problems.18 Refinements to improve sensitivity to change are currently being evaluated and may include replacing the ‘yes/no’ answers with a 0–7 score to reflect the number of days affected in the previous week.

Simple morbidity score promoted by the Royal College of Physicians.17
Despite the emphasis on structured care undertaken in most UK practices by asthma nurses19 as part of the Chronic Disease Management programme,20 only about a third of patients achieve an annual review.21,22 Many reasons have been suggested to account for the reluctance of patients to attend for an asthma review, but a common theme is a perception that their asthma is not serious enough to warrant the time involved in attending an asthma clinic.21,22 Innovative ways of improving access will need to be considered if practices are to improve the proportion of patients currently receiving a regular review. A trial of telephone consultations has shown that this mode of consultation can increase the proportion of patients reviewed with no loss of asthma-related quality of life or patient sat-isfaction.23 The shorter duration of telephone consultations suggests this may be an efficient way of delivering care. Other innovations, such as e-mail consultations, have yet to be evaluated, but may contribute to improving access to regular asthma reviews.
Monitoring of people with COPD
COPD is a condition in which deterioration is inevitable, particularly if the patient continues to smoke, so advice that patients should be reviewed regularly seems reasonable.3,8 There is, however, no evidence to inform decisions about the most appropriate models of care. Issues that still need to be addressed include identifying the frequency of recall app-ropriate for different severities of COPD, the important components of quality care, and who should deliver that care.24 Reviews may include the following key components.
Reassessment of spirometry
Monitoring the rate of decline of lung function detects those patients with accelerated deterioration (>500 ml over 5 years) in whom specialist opinion may be considered,3 and provides a reminder to review care in response to reducing lung function.
Ongoing health promotion
Smoking cessation advice is crucial, but encouragement to maintain an active lifestyle is also important.25
Ongoing assessment and optimisation of therapy
The Medical Research Council (MRC) dyspnoea scale (Box 3) is recommended for grading breathlessness and alerting the clinician to increasing disability and the corresponding need for increased provision of bronchodilators.3,26
Box 3. Medical Research Council dyspnoea scale.26
It is recommended that this dyspnoea scale should be recorded at every routine review for people with COPD
Recognition and management of complications
Depression is recognised as a significant complication of COPD and may need treatment. Severe COPD, the onset of cor pulmonale, or an oxygen saturation of <92% suggests chronic hypoxia and should prompt referral for consideration of long-term oxygen therapy.27
Assessment of disability
Additional social support may be needed as symptoms impact on activities of daily living.
Recent advances in the management of asthma and COPD
All doses of inhaled steroids refer to beclomethasone given via a metered dose inhaler (BDP≡). Adjustment may be necessary for fluticasone, mometasone or other devices.
Asthma management
The BTS–SIGN asthma guidelines reinforce the advice that inhaled steroids are the recommended preventer drug for adults and children,2 although it is now clear that, for many patients, the optimal maintenance dose may be 400 mcg via a metered dose inhaler daily (BDP≡) for adults or 200 mcg for children. Recent advances have extended our understanding of the most appropriate options when low doses of inhaled steroids fail to adequately control symptoms. Much research has been devoted to identifying effective therapeutic regimes, but it is important not to overlook the need for a broad assessment when asthma control deteriorates. Patients may stop taking inhaled steroids, or decide to abandon the spacer device that ensures effective delivery of the drug. Environmental factors may be significant, either at home or work. Importantly, the deterioration may be due to the development of other medical conditions.
The link with rhinitis
The importance of the link between asthma and rhinitis has been highlighted by the Allergic rhinitis and its impact on asthma guidelines.28 A third of people with rhinitis will develop symptoms of asthma and over half of asthma suffers will also have rhinitis. This concept of ‘one airway, one disease’ has a number of implications for the primary care clinician. Enquiry about asthma symptoms should be part of the routine assessment of patients with rhinitis. Conversely, assessment and treatment of rhinitis should be part of routine asthma reviews. Some studies have suggested that treating the rhinitis with nasal steroids may improve asthma control.29
Although interventions designed to reduce house dust mite exposure in patients with perennial rhinitis may be of some benefit in improving rhinitis symptoms,30 reducing allergen levels has not been shown to be an effective measure in adults with asthma.31,32
‘Add-on therapy’ for asthma
Recognition that, for many patients, increasing the dose of inhaled steroids confers little additional benefit while increasing the side effects has led to interest in alternative strategies for improving asthma control. Early suggestions that long-acting b-agonists might be useful add-on therapy have been corroborated by a significant body of evidence.33-35 The addition of a long-acting b-agonist to a modest dose of inhaled steroids can reduce symptoms and the need for rescue medication, improve quality of life, and reduce exacerbations. This supports the recommendation in the BTS–SIGN guideline that adults should not increase their maintenance dose of inhaled steroid above 800 mcg daily (BDP(integral)) via a metered dose inhaler without a trial of other therapy. The equivalent dose in children is 400 mcg daily. The first choice ‘add-on’ therapy for adults and older children is a long-acting b-agonist.2
This statement, however, belies the complexity of tailoring medication to individual circumstances:
Adding formoterol to low doses of budesonide is as effective as quadrupling the dose of budesonide for treating the symptoms due to ‘mild’ loss of control. The number of ‘severe’ exacerbations, however, are controlled better by a high dose of inhaled steroids.34
Leukotriene antagonists can reduce the symptoms of rhinitis,36 raising the possibility that patients whose asthma has slipped out of control during the hay fever season may benefit from a treatment that can help both manifestations of their allergy.
Both long-acting β-agonists and leukotriene antag-onists effectively reduce exercise-induced asthma,2 and a patient's preference for a tablet or an inhaler may be an important factor in selecting treatment.
In pre-school children long-acting β-agonists appear to be less effective, and leukotriene antagonists may be the better option.37
The clear message is the importance of assessing each patient individually and monitoring the effect and side effects of any change in treatment.
Many questions, however, remain to be answered. Pragmatic studies are needed in primary care populations to allow for the influence of patients' preferences, compliance and inhaler technique on outcomes. Combination inhalers containing an inhaled steroid with a long-acting b-agonist, with their potential for convenient dosage schedules but reduced ability to adjust individual drug doses, add yet another dimension to influence the clinician's decision.
Leukotriene receptor antagonists
Leukotriene antagonists are orally active drugs that block the action of the cysteinyl leukotrienes. Recent trials suggest that they can improve asthma control in combination with inhaled steroids, and are currently recommended as first-line add-on therapy for children under 5 years old.2,37,38 They reduce eosinophilic inflammation but they are considerably less potent than inhaled steroids, which remain the preventer treatment of choice in patients of all ages,2 although emerging evidence is exploring the role of leukotriene antagonists as preventer treatment for pre-school children with episodic, viral-induced wheeze.
COPD management
The mainstay of the pharmacological treatment of COPD remains b-agonists and anticholinergics.3 These probably work, at least in patients with severe disease, by reducing hyperinflation rather than by bronchodilation, and their efficacy is not predicted by improvements in lung function. Trials of treatment should therefore be based on sympt-omatic response rather than peak flow or spirometric reversibility. Use of higher doses of bronchodilators, ideally delivered from a metered dose inhaler via a spacer, may be limited in some patients by side effects. Long-acting b2-agonists provide sustained relief from symptoms and improve exercise tolerance, and recent evidence confirms their role in patients continuing to experience symptoms with short-acting bronchodilators.3,8,39
Tiotropium
Tiotropium is an anticholinergic drug with a very long dur-ation of action which improves clinical outcomes, including reducing shortness of breath and the number of exacerb-ations.40 It is administered regularly on a daily basis. The half-life of several days means that it may be a week before maximum benefit is achieved.
Inhaled steroids in COPD
Four major studies, using different inhaled steroids in patients with a range of severity of disease, have demonstrated that inhaled steroids do not reduce the accelerated decline in lung function in COPD.9,41-43 Current guidelines, therefore, do not recommend the routine use of inhaled steroids in patients with COPD.3,8 Response to a short course of oral steroids does not reliably predict benefit from long-term inhaled steroids.3,8,9
A large UK trial, which studied a moderate to severe group of patients, showed a reduction in the exacerbation rate from 1.33 to 0.99 episodes per year, reflected in an improved quality of life.9 This suggests that patients with moderate to severe disease (FEV1 <50% predicted) who have frequent exacerbations (for example, more than two exacerbations per year) would benefit from using inhaled steroids. However, practical questions remain. Which inhaled steroid should be used, at what dose, and via which delivery system? Side effects, particularly easy bruising and local oral symptoms,9,42 may be a concern at the relatively high doses of inhaled steroids (800 mcg to 2000 mcg [BDP(integral)] via a metered dose inhaler daily) used in these studies.
Pulmonary rehabilitation
Patients with moderate to severe COPD will benefit from the multidisciplinary, holistic approach of pulmonary rehabilit-ation. Most programmes are hospital based, although some are carried out in the community and a few are based in primary care.44 Details of each programme vary, but important components include a reassessment of therapy, exercise training, an education programme and psychosocial support.45 Pulmonary rehabilitation can increase exercise tolerance, relieve breathlessness, reduce hospital admissions and improve quality of life46 and should be offered to all patients with more severe disease if a service is available locally.
Palliative care
The prognosis in severe COPD is poor, with only half the patients discharged from hospital after an exacerbation surviving 2 years.47 Regrettably, the palliative care needs of this severely disabled group of patients are rarely met.48 A lack of opportunity to discuss end-of-life decisions denies patients the right to prioritise palliative treatment, such as morphine to reduce dyspnoea,49 and potentially life-sustaining interventions such as mechanical ventilation. The ‘common sense’ approach suggested by Abrahm may be a useful basis for planning care.50 This recognises the unpredictability of the terminal phase of COPD and suggests that, rather than delay until death is imminent, discussion about palliative care should be offered as soon as it is recognised that death could occur at any time due to other ordinary intercurrent illness.
Oxygen therapy
Oxygen therapy is important both acutely, to treat asthma attacks or other respiratory emergencies, but also to relieve the hypoxia that complicates severe COPD. Pulse oximeters are readily available and relatively cheap; oximetry has been shown to be both feasible and useful in primary care.51 The need for long-term oxygen therapy should be considered in patients with severe COPD (FEV1 <30% predicted) and those with peripheral oedema or polycythaemia. Screening in primary care would ensure that all potentially eligible patients (those with an oxygen saturation of <92%) are referred for formal assessment for long-term oxygen therapy.
Drugs on the horizon
Monoclonal anti-immunoglobulin E antibodies
Omalizumab is an anti-immunoglobulin E antibody that lowers free immunoglobulin E levels, reducing responsiveness to antigen challenge. In patients with severe allergic asthma this can reduce symptoms and exacerbation rates. Omalizumab is administered by subcutaneous injection at 2- to 4-weekly intervals. Despite the inconvenience this imposes, patients report an improved quality of life.52
Phosphodiesterase 4 inhibitors
PDE4 inhibitors are highly selective derivatives of theophylline. Early studies suggest they may have an anti-inflammatory effect in COPD and may improve lung function, possibly reducing exacerbation rates without the side-effect profile that limits the usefulness of theophyllines.
Self-management in asthma and COPD
Asthma action plans
The evidence that self-management education, including the provision of written asthma action plans, improves morbidity and reduces acute episodes is not new.15 It is given the highest grade of recommendation by the BTS–SIGN guideline and was one of the key messages promoted after the launch of the guideline. Despite this, only a minority of people with asthma have an asthma action plan,21 possibly because self-management is seen as complex and time consuming to implement.53 Some of the common questions about implementation raised by primary care clinicians are discussed below.
Should plans be based on symptoms or peak flows?
Most trials have included both symptoms and peak flows in their action plans. One primary care study that compared symptom-based plans with peak flow-based plans showed no difference.54 Clinicians may be guided by individual patient preference.
Should we advise patients to double their inhaled steroids at the onset of deterioration?
The studies that have contributed to the evidence base supporting self-management have included a step at which inhaled steroids should be increased. Evidence of limited effect of doubling inhaled steroids from studies of compliant patients poorly controlled on moderate doses has raised doubts about this strategy.33-35 However, in a trial of patients with mild to moderate asthma, Foresi showed that 200 mcg of budesonide daily, with a five-fold increase for 1 week at the onset of an attack, reduced exacerbations as effectively as taking 800 mcg of budesonide throughout, and significantly better than the group maintained on 200 mcg of budesonide.55 Patients with mild asthma, often poorly compliant and on a low maintenance dose, should be encouraged to substantially increase (or recommence) inhaled steroids as soon as control slips.
Should patients have an emergency supply of oral steroids?
Delay is the commonest preventable factor in asthma deaths, and prompt use of oral steroids is critical. Patients at risk of acute attacks may wish to accept responsibility for commencing a course of steroids when symptoms increase and bronchodilators become increasingly ineffective. A fall in peak flow to less than 60% of their best will confirm the need for action.
Doesn't this take time?
There is evidence that written action plans should be provided in the context of self-management education.56 However, education may be seen as an on-going process that can be incorporated into normal care. An initial appointment with a practice asthma nurse should be supported by all healthcare professionals using every opportunity to review, refine and reinforce the advice.2
Will patients follow their action plans?
Patients will vary in the autonomy they wish to accept and plans need to be adapted accordingly. Qualitative data suggest that patients adapt their action plans in the light of experience, reinforcing the concept of self-management education as an ongoing process.57
An example of a suitable personal asthma action plan is available from Asthma UK (www.asthma.org.uk).
Self-management of COPD
Self-management for patients with COPD has been less well studied. In a trial of secondary care patients, implementing self-management plans as part of an intensive education programme reduced acute admissions by 39%.58 A smaller study in primary care patients showed significant changes in self-management behaviour.59 These findings should encourage further research to identify the most appropriate type of action plan for patients with COPD.
Delivery of care for people with respiratory disease
In January 2003 an alliance of UK medical charities, organ-isations and professional bodies with an interest in the prov-ision of respiratory medicine published a report, Bridging the Gap.60 This document defined ‘reasonable patient expectations’ and provided checklists for primary and secondary care professionals working with primary care trusts to deliver high quality, integrated respiratory health care. Current services will need to be developed and new initiatives encouraged if these aims are to be met. (A list of respiratory organisations and useful websites can be found in Supplementary box 2.)
Spirometry services
Recognition of the importance of spirometry and the availability of relatively cheap electronic spirometers has stim-ulated considerable interest in undertaking spirometry within general practices. In 2001 two-thirds of general practices owned a spirometer.61 There are concerns, however, about the quality of spirometry undertaken in primary care,62 particularly as a recent survey observed that in a quarter of general practices spirometers were used by staff with no formal training.61 Strategic planning of spirometry services, either at practice or primary care trust level, will need to address issues of quality as well as capacity in order to meet the demands of the GMS contract1 for objective diagnosis and monitoring of COPD.
Hospital at home
Respiratory disease is responsible for one in eight emergency hospital admissions,63 and is a major contributory factor in the winter bed crisis.64 There is considerable interest in the concept of hospital at home, and recent trials have suggested that about a third of admissions can be prevented,65 and lengths of stay halved66 with supported discharge and nurse-led home care. Patient satisfaction with these schemes is high.67
Allergy services
The increasing incidence of allergic disease, including asthma and rhinitis, has exposed the inadequate provision of allergy services in the UK. In their report Containing the allergy epidemic the Royal College of Physicians recommend that allergy services should be coordinated in a regional allergy centre, but recognises the ‘front-line’ role of primary care and advocates improved training of GPs and practices to meet the increased demand.68
Supplementary information
A list of relevant guides and useful resources accompany this paper at: http://www.rcgp.org.uk/journal/index.asp
Box 4. Key messages.
Diagnosis
Objective diagnosis and assessment of patients with asthma or COPD is a prerequisite of appropriate management.
Monitoring
Structured care involving regular review improves asthma morbidity and may enable the provision of holistic care for COPD.
Management
Guidelines define strategies for the management of asthma and COPD: their application will be influenced by the individual clinical circumstances and the patient's preference.
Self-management
Written, personalised asthma action plans improve health outcomes and should be offered to all people with asthma. The role of self-management for people with COPD has not yet been clarified.
Delivery of care
Current provision for respiratory health care and allergy services does not meet reasonable patient expectations.
Acknowledgments
Thanks are due to Professor David Price for his helpful comments on an earlier draft.
Footnotes
This text is based on a chapter in the forthcoming RCGP book due to be published in 2004: Charlton R and Lakhani M (eds). Recent advances in primary care.
- © British Journal of General Practice, 2004.
References
In this issue









{kind=link}
Jump to section
More in this TOC Section
Related Articles
Cited By...

