


Abstract
Background: Although children are frequently referred to specialists, detailed information on referral patterns of them is scarce. Even less information is available on how referral patterns evolve over time.
Aims: To examine current referral patterns for children aged 0–17 years and compare these with referral patterns reported for 1987.
Design of study: Data were analysed from two national cross-sectional surveys, performed in 2001 (91 general practices) and in 1987 (103 general practices).
Setting: Dutch general practice.
Method: All new referrals to specialists were assessed by age, sex, International Classification of Primary Care (ICPC) category, specialty referred to, and specific episodes of disease. Referral measures were quantified as new referrals per 1000 person–years and per 100 new episodes, a measure of likelihood of a young person with a specific diagnosis to be referred. Rates in 2001 were compared with those from 1987.
Results: Referral rates decreased from 138 per 1000 person–years in 1987, to 84 per 1000 person–years in 2001. Age differences in referral rates were similar in both surveys. Compared with 1987, more boys than girls were referred to specialists. The overall likelihood of a condition being referred decreased from 8.0 per 100 episodes in 1987 to 6.5 per 100 episodes in 2001. Reasons for referral had also changed by 2001, particularly for the ear, nose, and throat (ENT) specialist and ophthalmologist. Moreover, referral rates for acute otitis media, refractive disorders, and vision problems decreased two- to fourfold in 2001.
Conclusion: Presently, Dutch general practitioners tend to manage more health problems themselves and refer less young people to specialists.
Introduction
ALTHOUGH the vast majority of health problems in children presented in general practice are managed by the general practitioners (GPs) themselves, a part of GPs' treatment of children involves referrals. In the Netherlands, as in the United Kingdom (UK), the GP acts as a gatekeeper for specialist care, so that access to specialist care is limited to those patients who are referred by their GP. Moreover, because every Dutch inhabitant is listed in a general practice, referrals by GPs provide valid insight into the use of specialist care.
Only a few studies have examined referrals in children to specialists by GPs in more detail. Studies have either small numbers,1 or are restricted to referrals to a single outpatient clinic.2 Even less information is available on how referral patterns evolve over time within a particular country. In the first Dutch national survey, performed in 1987, referral rates for children in general practice showed varying referral rates by age, sex, and specialty referred to.3 Since this first national survey, several changes have been made in health care for children in the Netherlands. For example, several evidence-based guidelines for childhood diseases have been implemented to help decision making for referral to specialist care. These guidelines are generally accepted and widely used by Dutch GPs.4
It is of interest, not only for GPs but also for specialists, to have insight in up-to-date and nationwide representative information on GPs' referral rates. It is also of interest to know which conditions are frequently referred and which childhood problems are managed predominantly by GPs and therefore seldomly referred. Moreover, valuable insight may be gained in the demand for outpatient specialty care.
The objective of our study was to examine current referral patterns of GPs to specialists for health problems in children aged 0–17 years, and to compare these data with the first Dutch national survey of 1987.
Method
Data were analysed from the second Dutch national survey of general practice, which was performed by the Netherlands Institute for Health Services Research (NIVEL) in 2001. In addition, secondary analyses on data from the first Dutch national survey (1987) were performed. Details on the design of both national surveys have been described elsewhere.5,6
For the current study, data on children aged 0–17 years were analysed from both surveys.
HOW THIS FITS IN
What do we know?
Children are sometimes referred to secondary care, but detailed information on general practitioners' (GPs') referral patterns is scarce. Very few studies have examined referral patterns of children over time.
What does this paper add?
Dutch GPs increasingly handle childhood conditions themselves, parallel to the introduction of evidence-based guidelines. Referral patterns have changed over the past decades and specialists nowadays see a different range of childhood morbidity, in particular ear, nose, and throat specialists and ophthalmologists.
First Dutch national survey
The first national survey was performed in 1987. A non- proportionally stratified sample of 161 GPs (103 practices) was randomly selected to participate in the study. The GPs were divided into four groups and each group registered all contacts between patient and doctor on registration forms during one of four consecutive 3-month periods during 1987. Data recorded of each consultation included patient characteristics (age, sex), reason for encounter, diagnosis, and new referrals to specialists. Diagnoses made by the GP were coded afterwards by specially trained clerks using the International Classification of Primary Care (ICPC-1).7 The first national survey was episode-orientated, meaning that different consultations concerning the same health problem were clustered into one disease episode. The last diagnosis made by the GP was considered the diagnosis of the episode. If a referral was made during a consultation, the specialty referred to was registered and the referral was linked to the diagnosis made by the GP and to the relevant episode. Because of an underrepresentation of the population in deprived areas, the population was weighted according to their proportion in the total population of the Netherlands at the time.
Second national survey
The second national survey was performed in 2001; 195 GPs in 104 practices were initially recruited to the study. The participating GPs and practices were representative for Dutch GPs and practices. The total study population consisted of 394 192 patients, a 2.5% representative sample of the Dutch population.
During a 1-year period all patient contacts and all new referrals were registered. All health problems presented within one consultation were recorded separately using the ICPC and the diagnosis was coded immediately by the GP using ICPC. This survey was also episode orientated. Patient characteristics such as age and sex were derived from the GPs' computerised patient records.
For this analysis data from 13 practices were excluded for the following reasons: in eight practices the quality of registered data was poor, and five other practices failed to register referrals.
Measures of referral and analysis
For this study all new referrals to secondary care were evaluated by referring diagnosis and specialty referred to. Referring diagnosis was considered the diagnosis at the time the referral was made. A referral was considered new when a child was referred to a specialist for the first time for a certain health problem. If, later on in the study period, he/she was referred to the same specialist but for a new and different health problem, this was also considered as a new referral. The referral rate was calculated as the number of referrals per 1000 person–years. The referral rate by episode of illness, a measure of likelihood of a certain health problem being referred, was calculated as the number of referrals for a certain condition per 100 new episodes presented to general practice.3 For analysis SPSS version 11.0 was used.
Results
Overall referral rates
The study population of the 2001 survey consisted of 78 648 children aged 0–17 years. A total of 101 398 new episodes were presented in general practice and 6608 new referrals were made to specialists. A total of 6130 children were referred (7.8% of all children [95% confidence interval [CI] = 7.6 to 8.0]). The overall referral rate to specialists was 84 per 1000 person–years (95% CI = 82.0 to 86.0) as shown in Table 1. The study population of 1987 consisted of 86 577 children, who presented 37 715 new episodes, and 2997 new referrals were made during the 3-month study period. This resulted in an overall referral rate of 138 per 1000 person–years (95% CI = 134 to 143).
Referral rates for the population and referral rates per episode of illness by ICPC category in 1987 and 2001.
Referral by age and sex
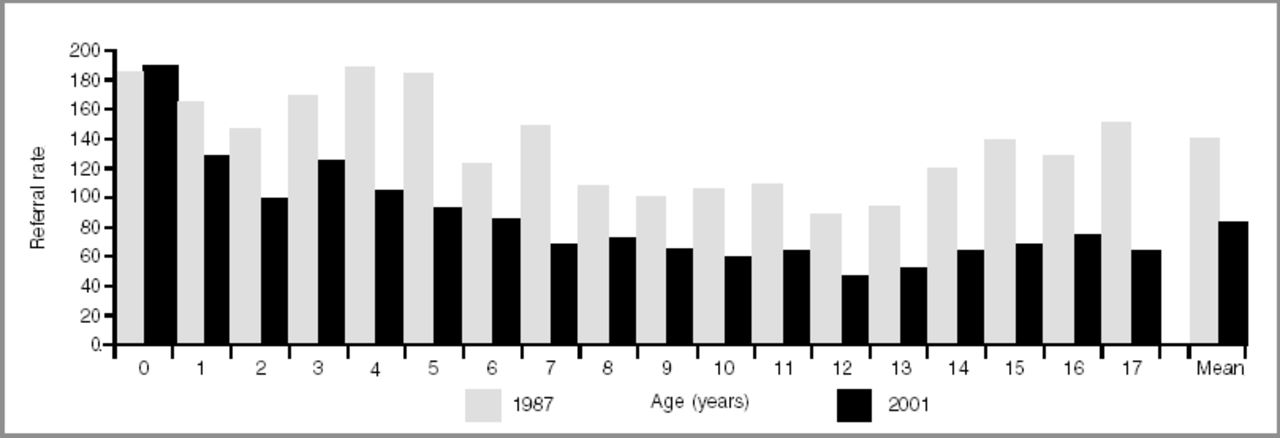
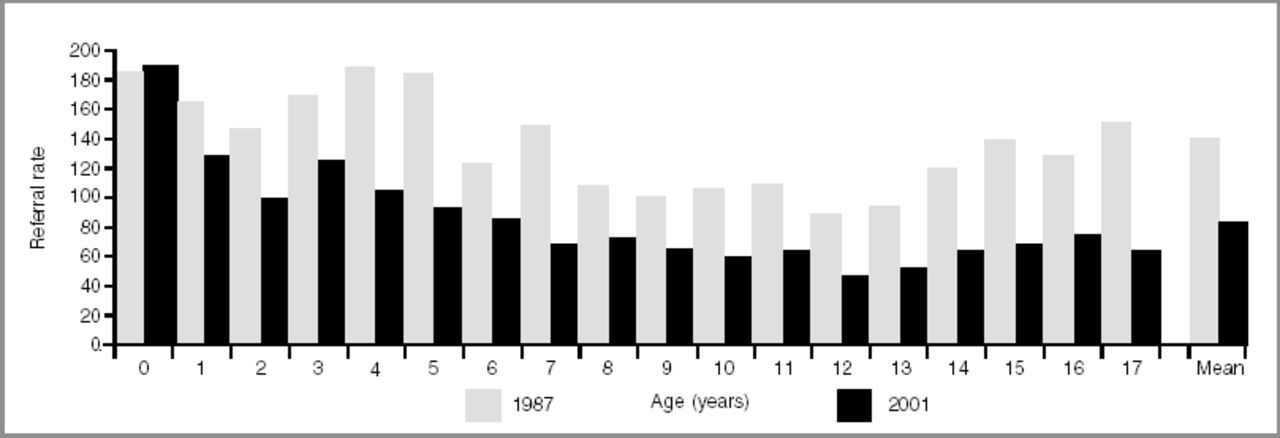
Figure 1 shows the distribution of the referrals by age for 1987 and 2001. Both surveys show similar referral patterns for age: most referrals in the first years of life (mainly to paediatricians and ear, nose, and throat [ENT] specialists), fewest referrals at ages 10–14 years, and an increasing number of referral at ages 15–17 years.
{kind=link}
Referral rates for the population by age in 1987 and 2001 per 1000 children per year.
In 2001, boys were referred more often to specialists than girls (boys: 89/1000 person–years; girls 79/1000 person–years, P<0.001). In 1987, girls were referred to specialists as often as boys (girls: 138/1000 person–years; boys 140/1000 person–years, P = 0.69).
Referral rates by diagnosis
Table 1 gives an overview of the referral rates for the population and referral rates per episode of illness for both surveys by ICPC category. The likelihood of being referred, quantified in the referral rate per 100 episodes of illness, decreased from an overall rate of 8.0 in 1987 to 6.5 in 2001. Both population-based and episode-based referral rates for musculoskeletal problems decreased by 65% and 55% respectively, indicating that considerably more musculoskeletal problems were managed by GPs themselves in 2001, and were less frequently referred to secondary care. It is also shown that population-based referral rates for respiratory and skin problems are high, but the likelihood for these conditions to be referred is relatively low. In 2001, GPs referred more children with psychological or psych-iatric problems than in 1987. This increase is mainly accounted for by a substantial increase in referrals for learning problems.
Table 2 gives the top five diagnoses leading to referral within each of the specialties most frequently referred to in 2001 (covering 41% of all referrals). Referral rates for the population and referral rates per episode of illness from both surveys are shown. This table illustrates that the reasons for referral have changed considerably, especially for referrals to the ENT specialist: in 2001, the population-based referral rate for acute otitis media was 72% lower than in 1987 and is no longer the main reason for referral to the ENT specialist, as it was in 1987. Among dermatological diseases, in 2001 warts were treated more often by GPs themselves than in 1987.
Top five diagnoses of the specialists most frequently referred to.
Discussion
Referral patterns of children have changed considerably over the past 15 years in the Netherlands. Our results show that Dutch GPs presently refer fewer children and are less likely to refer children to specialist care.
Not only has the overall number of referrals decreased, reflected in a lower population-based referral rate of 40%, but also the overall likelihood of a certain condition being referred, reflected in the referral rate per 100 episodes of illness, has decreased by almost 20% — the mean referral rate per episode changed from 8.0 to 6.5. In part, the decrease in population-based referral rate can be explained by an approximate 25% decrease in childhood consultation rate from 1987 to 2001 (unpublished data). However, the episode-based referral rate reflects GPs' referral decision and is independent of differences in consultation rates (when assuming that severity of childhood morbidity presented in general practice has not changed). That these episode-based referral rates have declined as well, demonstrates clearly that GPs tend to manage more health problems themselves in 2001 than they did before.
The healthcare systems in the UK and the Netherlands share many similarities. In 2001, 7.8% of the children in the Netherlands were referred to specialists, only slightly less than the 8.7% reported recently in the UK.8
To our knowledge no studies have examined GPs' referrals of children over time. Moreover, only a few studies have explored referral patterns for patients of all ages over time. A Dutch study examining new referrals from 1971 to 1994 in four general practices showed a decrease of new referrals after 1971, but from 1981 onwards the referral rates remained more or less stable.9 Statistics Netherlands collects secondary care-based data on referrals to specialists, and they found a decreasing number of childhood referrals between 1991 and 2000.10 A study of referral patterns in the UK showed a steady increase of referrals from 1990 through 1994, not only to all specialties but also to paediatrics.11
Referral rates for children vary greatly by age at referral, which is illustrated for both surveys in Figure 1. Both surveys show highest referral rates in the first years of life, lowest rates at ages 10–14 years, and a gradual increase in the later-teen age groups. This is consistent with results of other studies.12 Although not fully understood, boys are referred to specialists more often presently, a finding also reported by others.13,14
Parallel to the overall decreased referral rate, the likelihood for a condition being referred, quantified in the referral rate per 100 episodes of illness, also decreased, although to a lesser extent. One explanation is that, during the past 15 years, a considerable amount of research has been performed in primary care rationalising a watchful–waiting policy or non-invasive treatment for several childhood conditions, showing that referral to secondary care is often not necessary.
Furthermore, based on this research, several new guidelines for childhood diseases were developed including criteria for referral — these may have attributed to the decrease in episode-based referral rates. In particular, this may be the case for referrals to the ENT specialist and ophthalmologist. For example, the otitis media guideline (the first guideline concerning children) appeared in 1990 and gives clear advice as to when referral is appropriate.15 Although our study design does not allow statements about causal associations between lower referral rates and guideline adherence, our results do suggest that these guidelines are helpful in deciding when to refer and thus leading to fewer referrals to secondary care. This may also be the case for referrals to the ophthalmologist; a guideline on refractive disorders and vision problems was implemented in 1990, with well-defined recommendations as to when a child should be referred.16
In 2001, the likelihood of referral for respiratory problems had not decreased, but referral rates for these conditions decreased from 20.5 in 1987 to 13 in 2001. This implies that fewer children consult their GP for respiratory tract problems. In contrast to the trend of overall declining referral rates for children, we found that children were referred more often for learning problems. We hypothesise that these are related to attention deficit hyperactivity disorder (ADHD), for example that parents or teachers question whether learning problems of a child are caused by ADHD and request referral for further testing.
In 2001, referral and referability rates of conditions, such as fracture of the arm and appendicitis (diagnoses that generally need treatment in secondary care setting), decreased two- to threefold compared with 1987. An explanation for this unexpected finding could be that patients were treated directly in the emergency department, but registration of the referral was not made in the GPs' records.17
Limitations
Although both surveys were similar in design and were performed by the same research group, comparing referral rates of both surveys has limitations. For example, presently GPs may refer health problems to the physiotherapist that in 1987 may have been referred to the orthopaedic surgeon (a subanalysis, however, did not reveal any significant changes in referrals to physiotherapists). Furthermore, in 1987 each diagnosis was coded later by trained NIVEL clerks, whereas in 2001 the GPs coded the diagnoses themselves; this could lead to coding differences in diagnoses between the two surveys.
Implications for future research
This study gives a broad, up-to-date and representative picture of referral patterns in children. The results show that referral patterns have changed considerably over time, with an overall decreasing referral rate and an overall decreasing likelihood of diseases being referred. Changes in referral patterns may be due to improved primary care, but this study has not addressed the question whether the decrease in referrals implies a decrease in inappropriate referrals; this needs further research.
Acknowledgments
We thank all practice staff members who participated in the surveys, all field workers and all those involved in data management.
- Received October 13, 2003.
- Revision received March 2, 2004.
- Accepted April 30, 2004.
- © British Journal of General Practice, 2004.
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

