


Abstract
Background For the diagnosis of asthma in young children, GPs have to rely on history taking and physical examination, as spirometry is not possible. The additional diagnostic value of specific immunoglobulin E (IgE) to inhalent allergens remains unclear.
Aim To assess the predictive accuracy of specific IgE to cat, dog, and/or house dust mites in young children for the subsequent development of asthma at the age of 6 years.
Design of study Prospective follow-up study.
Setting Seventy-two general practices.
Method A total of 654 children, aged 1–4 years, visiting their GPs for persistent coughing (≥5 days), were tested for IgE antibodies by radio allergosorbent testing (RAST). Parents completed a questionnaire on potential risk indicators. Those children who showed an IgE-positive status (12.7%) and a random sample of those with an IgE-negative status (<0.5 U/ml) were followed up to the age of 6 years when the asthma status was established. The main outcome measure was asthma at the age of 6 years (combination of both symptoms and/or use of asthma medication, and impaired lung function).
Results Addition of RAST results to a prediction model based on age, wheeze, and family history of pollen allergy increased the area under the receiver operating characteristic (ROC) curve from 0.76 to 0.87. Furthermore, RAST improved patient differentiation as indicated by a change in the range of asthma probabilities from 6-75% before the IgE test, to 1-95% after the IgE-test.
Conclusion Sensitisation to inhalant allergens in 1-4-year-olds, as shown by RAST, is a useful diagnostic indicator for the presence of asthma at the age of 6 years, even after a clinical history has been obtained. This model should preferably be validated in a new population before it can be applied in practice.
INTRODUCTION
In general practice, cough is the main complaint in some 13% of all consultations for children aged 0–4 years.1 For GPs it is difficult to identify the subgroup of children for whom the risk of developing asthma is high enough to justify treatment. After all, the majority of children with isolated cough will not develop asthma.2
According to international consensus,3,4 asthma in children younger than 6 years of age is predominantly a clinical diagnosis, based on the presence of recurrent coughing and wheezing. In these children, the equipment for assessing lung function is neither easily nor routinely used.5 In the majority of children aged over 2 years who have asthma, allergies play an important role.6,7 Therefore, in these young children GPs may be able to decrease their diagnostic uncertainty by establishing whether an allergy is present, in addition to obtaining information from clinical history. If an allergy is present, this may have consequences for clinical management.3,8 We therefore assessed the extent to which the determination of specific immunoglobulin E (IgE) to cat, dog, and house dust mites — in addition to the easier obtainable information from the clinical history — may help GPs to predict asthma.
How this fits in
For the diagnosis of asthma in young children, GPs have to rely on history taking and physical examination, as spirometry is not possible. The additional diagnostic value of specific immunoglobulin E to inhalant allergens remains unclear. Sensitisation to inhalant allergens in 1–4-year olds, as shown by radio allergosorbent testing, is a useful diagnostic indicator for the presence of asthma at the age of 6 years, even after a clinical history has been obtained.
METHOD
The study design is outlined in Figure 1.
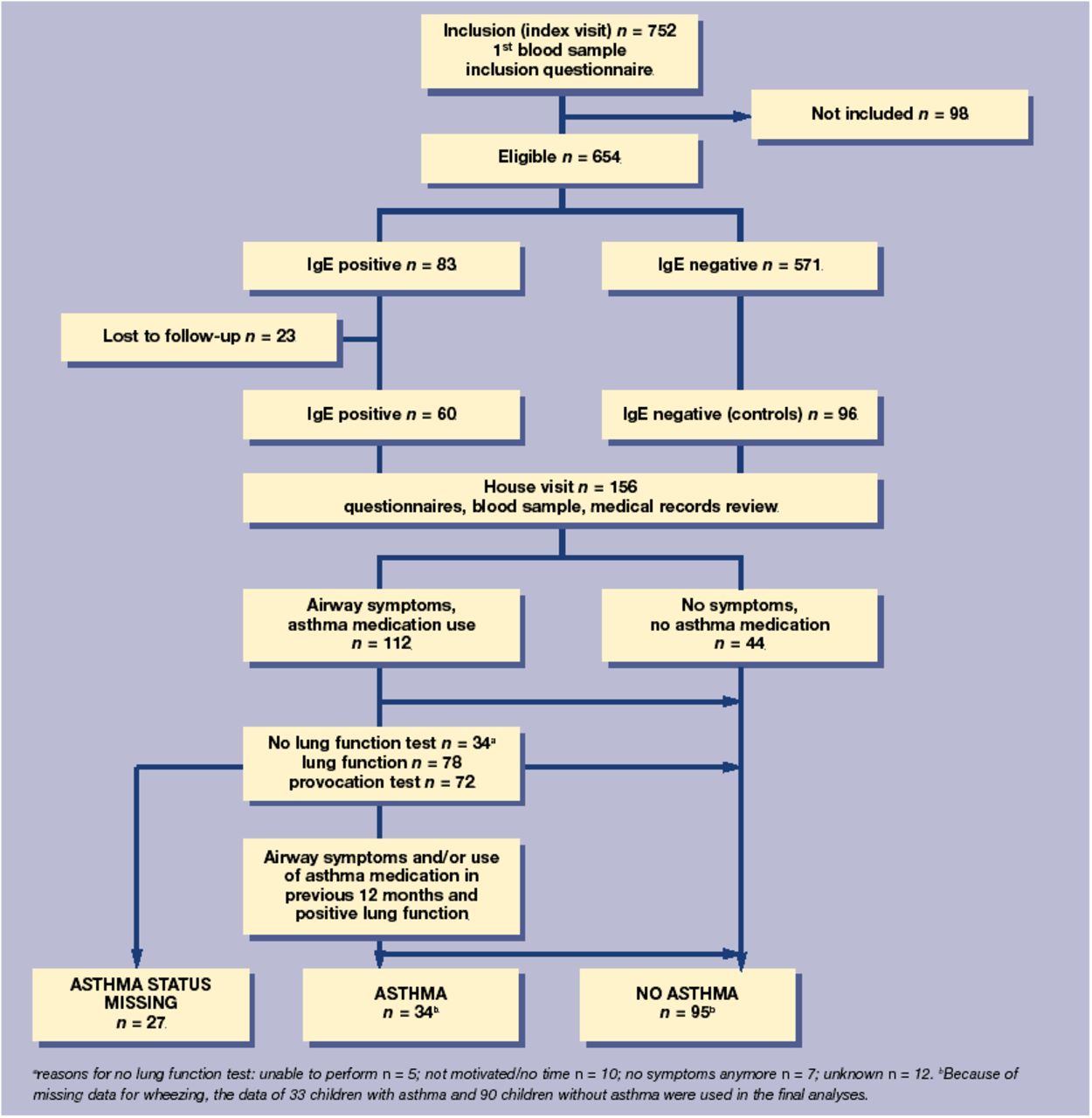
Flow chart of the study design.
Study sample
Between February 1995 and February 1997, 72 GPs in the northwestern part of the Netherlands, recruited 752 children aged 1–4 years to a study on the development of inhalation allergy and asthma in preschool children. Children who had complained of cough for at least the previous 5 days and who had visited their GP with their parent were invited to participate. Informed consent was obtained from the parents.
At baseline, data on age, sex, and geographical region were collected. Furthermore, the parents completed a structured questionnaire with 11 questions on duration of coughing, presence of atopy in the family, breastfeeding, infantile eczema, smoking by parents, and contact with pets. A blood sample was obtained from the children and total immunoglobulin E (IgE) and specific IgE for cat, dog, and house dust mites were determined. The children with an IgE-positive status were matched to those with a negative status in each of the 16 strata defined by age (four categories of 1 year), sex, and region (urban versus rural). In cases where a control patient with an IgE-negative status could not be traced (n = 12), was not willing to participate (n = 15), or was lost to follow-up (n = 16), a new matched control was selected among those with an IgE-negative status from the original cohort.
At the age of 6 years, the parents of the children with an IgE-positive status and a selection of those with an IgE-negative status were contacted again. Their written consent was asked for in order to review the child's medical records at the GP's office together with a lung function measurement at the clinic, and to determine the child's asthma status. At that time, parents completed two questionnaires on their child's asthma and allergic symptoms.9,10
Laboratory methods
Total IgE and allergen-specific IgE were determined as described earlier.11 In brief, blood obtained by a finger prick was absorbed on filter paper and eluted. Total IgE was expressed in international units per millilitre (IU/ml); radio allergosorbent testing (RAST) results were expressed in RAST units per millilitre (U/ml) with one RAST unit representing approximately 2.4 ng of specific IgE.12 All test results were corrected for actual amounts of plasma used in the tests, using serum albumin as a reference protein.
Medical records review
The GP or research assistant completed a case record form, which consisted of items regarding the child's asthma and allergy-related symptoms, and medication used during follow-up. These data were used to establish the definitive asthma diagnosis in combination with the results from the lung function tests.
Lung function measurements and histamine challenge
Children were required to withhold all bronchodilators 48 hours before the test. In case of shortness of breath the child was allowed to use salbutamol up to 8 hours before the test. The forced expiratory volume (FEV1) was measured until three reproducible recordings were obtained; the two best (within 5% or 100 ml of each other) were used for analysis. Measurements were performed with a Pulmoassist 2 spirometer (Jaeger, Wurzburg, Germany). Values for the FEV1 are those of Zapletal et al13 and were obtained on the day the histamine challenge test was performed.
Bronchial histamine challenge tests were performed with a gauged DeVilbiss 646 nebuliser (DeVilbiss, Somerset, MA, US) with an output of 0.13 ml/min according to the modified method of Cockroft et al.14 A 0.9% phosphate-buffered saline solution and doubling histamine concentrations from 0.03–16 mg/ml were inhaled for 2 minutes during tidal breathing with the child's nose clipped. FEV1 was measured 30 and 90 seconds after each inhalation until FEV1 had fallen by at least 20% from the initial value. The provocation concentration of histamine that induced a 20% fall in FEV1 (PC20) was calculated from a log-dose response curve.
Data analysis
Independent variables
The results of the RAST were dichotomised as IgE negative or IgE positive. IgE positivity to cat, dog, and/or house dust mites was defined as > = 0.5 kU/l. The information collected at baseline was used to derive predictor variables for the presence of asthma at the age of 6 years. As the questionnaire did not include questions on wheezing, we reconstructed the wheezing status at baseline of each child using their medical records.
Dependent variables
Asthma was defined as a combination of both symptoms and/or use of asthma medication and impaired lung function. Symptoms were defined as current complaints or complaints during the previous 12 months of wheezing and/or shortness of breath and/or recurrent coughing. In addition, use of asthma medication was defined as use of 2 agonists or inhaled corticosteroids currently or during the previous 12 months. Impaired lung function was defined as a positive histamine test, which, in turn, was defined as PC20 <8mg/ml.
All children who had not experienced any symptoms during the previous year and had not used asthma medication were not invited for lung function measurement and were considered as not having asthma.
Multivariable model
Combinations of demographic characteristics and clinical variables were selected using a forward stepwise logistic regression analysis with asthma as the dependent variable. Likelihood ratio statistics were used as a criterion for selection in the model. Variables with a P-value for entry of <0.05 and a P-value for removal of <0.10 were selected in the model. The regression coefficients from the best model were used to derive the probabilities of asthma for each child. Two models were constructed: the first was based on demographic characteristics and clinical history at baseline; in the second model the RAST results were added. All variables were coded as indicator variables using 0–1 coding.
For each child a score was calculated by multiplying the values of the regression coefficients by zero (if the child's test result belonged to the reference category) or by one (in any other case). In each model the probabilities of developing asthma were then calculated for each child using the formula ‘probability = 1/(1 + e-(score + constant))’, where the constant is the intercept from the regression model. The scores associated with each covariate pattern were plotted against the probabilities of having asthma at the age of 6 years. We accounted for the clustering of an average of three children per GP practice using robust variance estimators.15 The matching procedure was accounted for by a special regression analysis that weights observations by their sampling probability in each of the 16 strata.15
Finally, we compared the differences between the areas under the curve corresponding to the model without and with the RAST results. The final versions of the two logistic regression models were fitted 10 000 times using bootstrap methodology and the 10 000 corresponding differences between the areas under the curve were used to construct a more robust confidence interval around this area-under-curve difference.
Data analysis was performed with SPSS 10.0 for Windows, except for the standard errors of the predicted probabilities and the bootstrapping procedure, which were calculated using STATA 7.0.
RESULTS
During the inclusion period, 654 children were eligible; 83 of them (12.7%) had an IgE positive status for cat, dog, and/or house dust mites. A total of 96 children were selected from the remaining 571 children who had an IgE negative status, matching those with a positive IgE result. At age 6 years, 23 children who had an IgE positive status had been lost to follow-up. These children did not differ significantly in terms of variables/tests that were collected at inclusion from the children included in the final analysis. Thus, 60 children with an IgE positive status and 96 with an IgE negative status were available for descriptive analysis. A total of 112 children who had symptoms and/or used asthma medication were invited for the lung function test; the remaining 44 children who displayed no symptoms and used no medication were not invited to perform the lung function test. Complete results for lung function were available for 72 of the group of 112 children. No children showed airway obstruction as assessed by FEV1 (FEV1 <75% FEV1 predicted). Challenge testing showed that 56 children had a low PC20 (Table 1: a low PC20 corresponds with mild, moderate and severe responsiveness)
Clinical and lung function characteristics of the children in the study (n = 123).a
Twenty-seven children did not attend the lung function test or had an insufficient technique, so there were 27 missing values on the dependent variable. In this group of children, both those with and without symptoms dropped out. No significant differences were found in the distributions of other test results. For six children we could not reconstruct a value for wheezing from the records or questionnaires, and so regression analyses were performed on 123 children. The median number of days of coughing before the index visit to the GP was 14 days (interquartile range [IQR] = 7–25 days). Their general characteristics are shown in Supplementary Table 1. Thirty-three (26.8%) children were identified as having asthma: 23 (54.8%) had an IgE-positive status, and 10 (12.3%) an IgE-negative status.
Probability of developing asthma at the age of 6 years
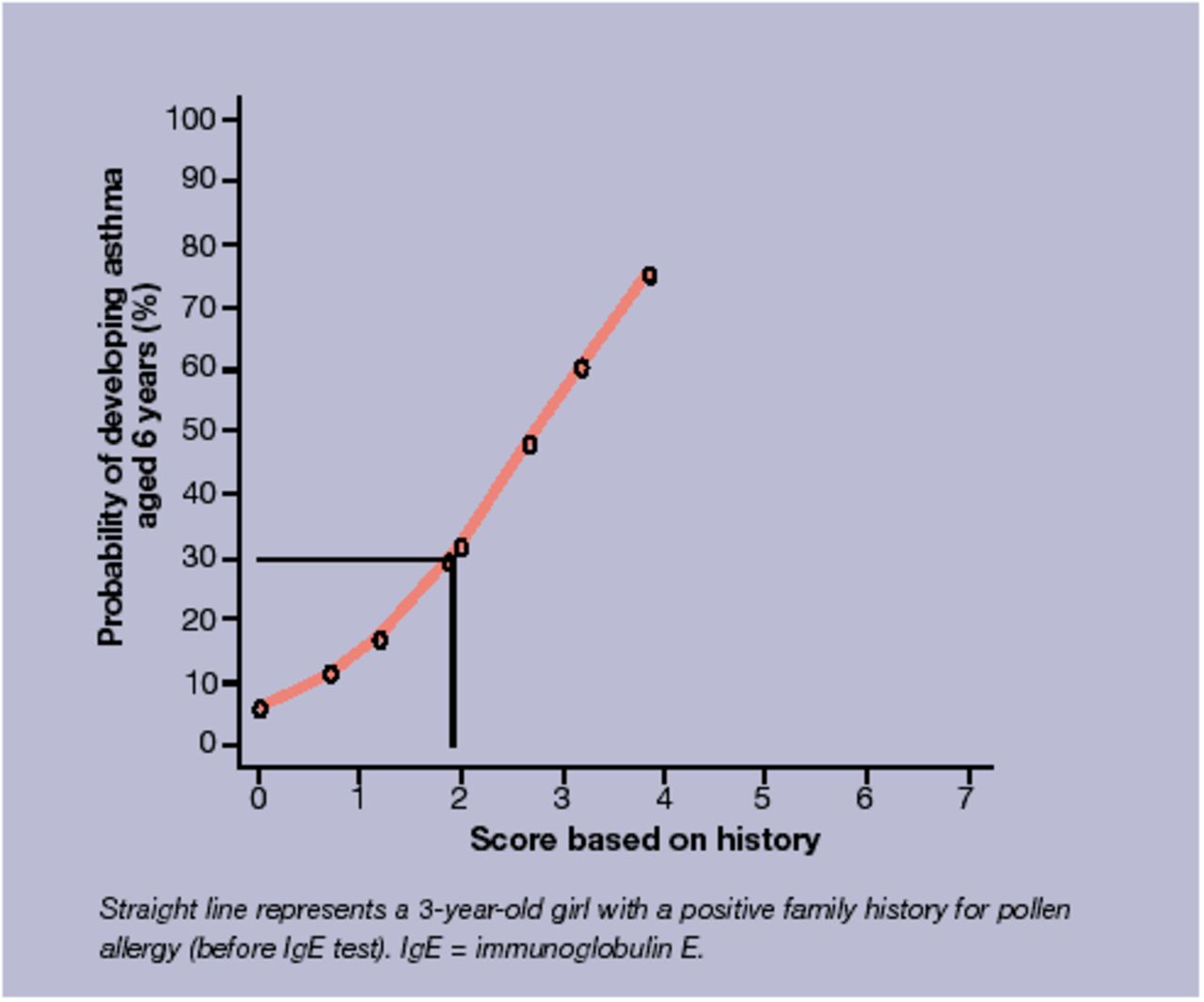
The prediction models included age at inclusion, wheezing, and family history of pollen allergy (Table 2). Adjustment for the matching procedure yielded similar results as the unadjusted analysis (data not shown). Therefore, the latter was used. The summed scores ranged from 0 to 3.9 for the model without specific IgE (model 1), and from 0 to 7.2 for the model containing specific IgE (model 2), with corresponding predictive values ranging from 6.1% to 75.2% for model 1 (Figure 2) and from 1.3% to 94.5% for model 2 (Figure 3). After the IgE test, the number of children in the extremes of the distribution increased at the expense of the middle range, indicating increased differentiation between those likely and unlikely to develop asthma at age 6 years.

Relation of scores (derived from 3–4 year olds, wheezing, familial allergy for pollen) to probability of developing asthma.
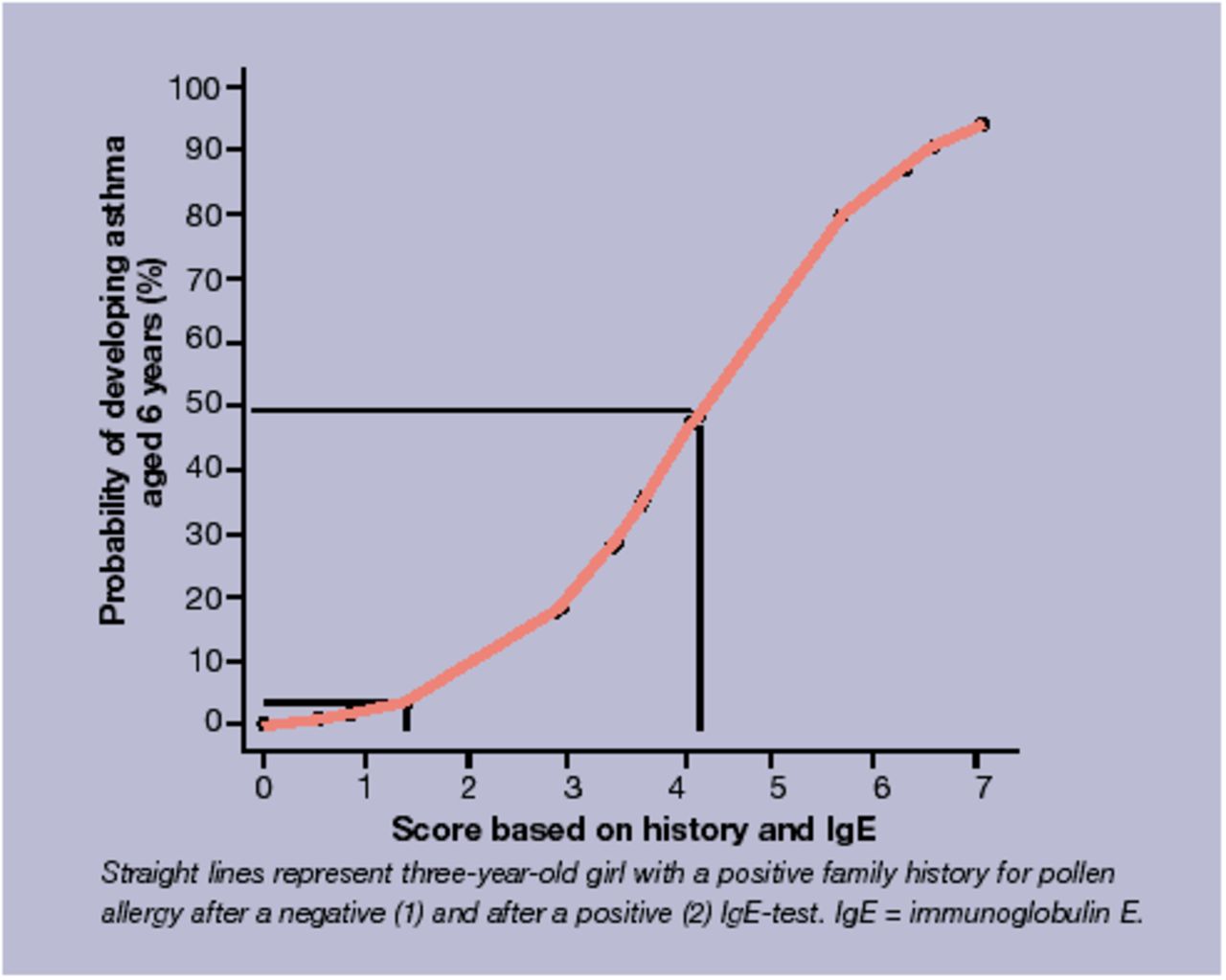
Relation of scores (derived from 3–4 year olds, wheezing, familial allergy for pollen, and specific IgE) to probability of developing asthma.
Results from logistic regression analyses (odds ratios [with 95% CI] and regression coefficients) for two models with demographic variables, variables with respect to clinical history and specific IgE.
For each covariate pattern the probability of developing asthma can be calculated before and after a RAST result (Supplementary Table 2). For example, a 3-year-old child that wheezed and had a negative family history of pollen allergy had a probability of developing asthma of 48.1%. After a negative or a positive RAST, his/her probability changed to 28.3% and 88.1%, respectively. Consider a GP who is willing to start treatment if the probability of developing asthma is greater than 50%. Since the covariate patterns without wheeze all yield probabilities of less than 50%, the GP is likely to refrain from treatment. Not even a positive RAST will change this and can, therefore, be omitted in these cases. By contrast, for the covariate patterns with wheeze and a negative family history of pollen allergy, the RAST may very well change the treatment decision.
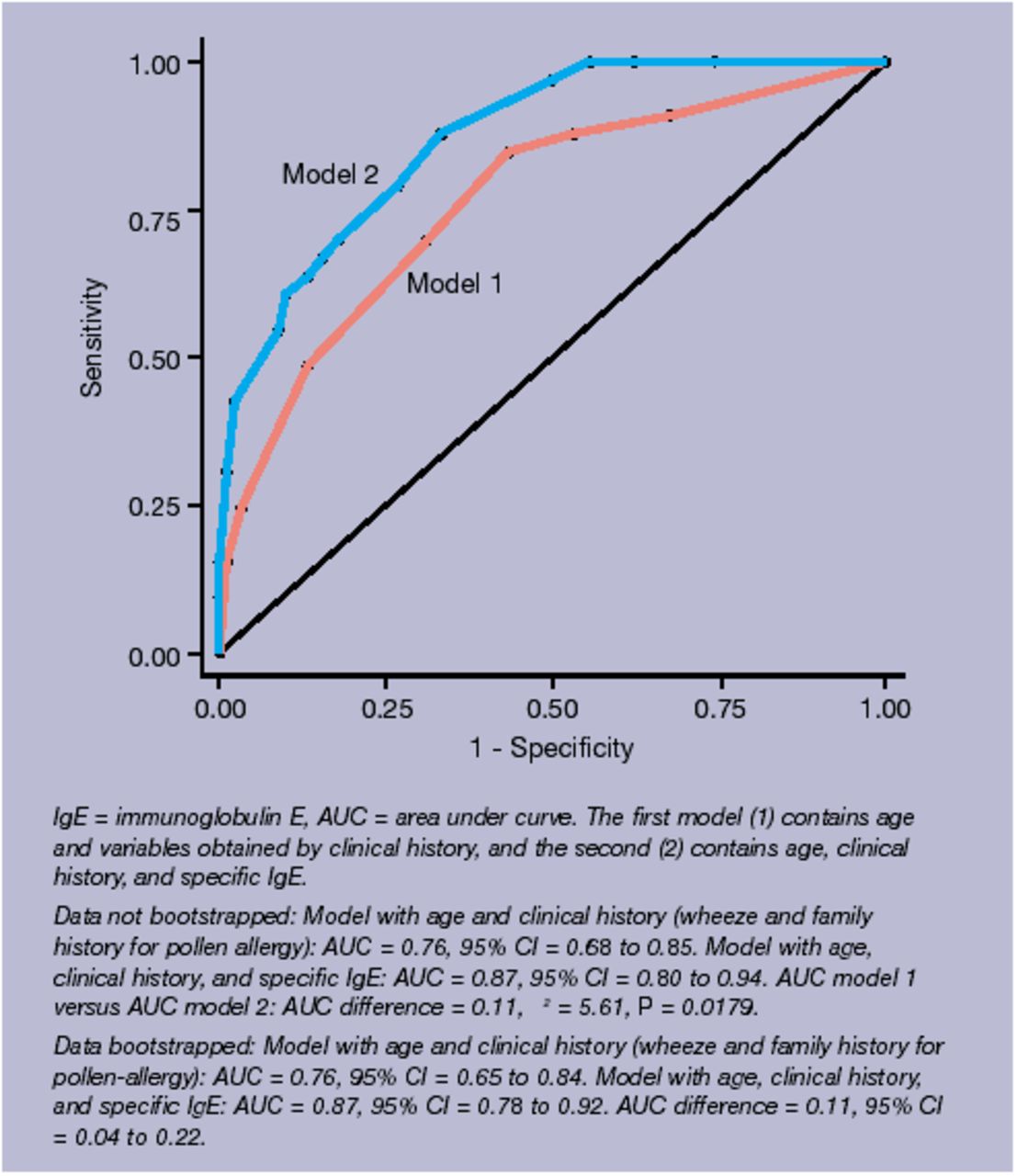
The area under the curve for the model containing items obtained by history taking increases from 0.76 (95% confidence interval [CI] = 0.68 to 0.85) to 0.87 (95% CI = 0.80 to 0.94) when specific IgE is added (Figure 4). Bootstrap methodology yielded CIs from 0.65 to 0.84 for model 1 and 0.78 to 0.92 for model 2; the 95% CI for the area-under-curve difference was from 0.04 to 0.22.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve for the models with asthma as the dependent variable.
DISCUSSION
Summary of main findings
In this study, we have investigated the diagnostic accuracy of IgE tests (RAST) to cat, dog, and house dust mites for the prediction of asthma at the age of 6 years in children under 5 years presenting with complaints of persistent coughing in primary care. After considering patient characteristics and clinical history, IgE testing improved the predictive accuracy, as indicated by an increase of the area under the curve by 11%. Furthermore, IgE testing improved patient differentiation as indicated by a change in the range of asthma probabilities from 6–75% pre-test to 1–95% post-test.
Comparison with existing literature
As was found in other studies,7,16 wheezing appears to be an important predictor of asthma. Children who did not wheeze had a less than 50% probability of developing asthma, even after a positive IgE test. For purposes of illustration, we used a 50% probability of asthma as a threshold for a GP to decide whether or not to start treatment. In reality, GPs' treatment thresholds may differ. Unfortunately, our study cannot answer the question of where a threshold should lie. Ultimately, that question can only be addressed by formal cost-effectiveness or cost-utility analyses. The current study may inform such analyses, which may then clarify the proper role of testing for IgE. Three other studies17-19 examined specific IgE as a diagnostic tool for asthma and found that it was important in predicting asthma. These results are in line with our study, although the children in these studies had wheezing as a presenting symptom and the studies were hospital based.
Strengths and limitations of the study
The fact that this study is based in general practice is a strength, but at the same time it can be considered as a limitation. Being based in general practice, the predictive function we constructed is likely to be valid for children who present at GPs' surgeries, and not necessarily for children in the general population. This is important as most research on asthma and allergy in children is either population-based or hospital-based; therefore, results from these studies cannot be applied straightforwardly to the primary care situation. As most children with allergy or asthma are diagnosed and treated in general practice, it is important to conduct research that can be applied straightforwardly to general practice.
Furthermore, most of the studies performed in the general population use wheezing as the inclusion criterion, whereas in this study, cough is used, because cough is the symptom most presented in general practice in this age group.
Although many researchers have studied asthma and allergy, this study is one of the few to construct a clinical prediction rule and to evaluate the added value of allergy tests for the diagnosis of asthma in young children in general practice. In other studies17-19 the value of IgE tests was examined in isolation, without reference to diagnostic information that is available in a diagnostic work-up in practice.
A limitation of this study is that some children may have received some form(s) of (intermittent) treatment. These were not included in the model. This implies that the predictive function we describe may be valid under current treatment practices according to international guidelines. If early treatments do not influence the probability of asthma at age 6 years, the function may have wider applicability. Currently, the impact of treatment is still controversial,5,20,21 although there is evidence that early treatment, such as inhaled corticosteroids, may improve lung function in the long run. In that case, in general practice, where most children with asthma are diagnosed, identifying those young children with a high enough probability of developing asthma is of clinical relevance.21,22
As data on wheezing was not collected at baseline, we reconstructed this variable from the retrospective review of the medical records and questionnaires completed after inclusion. If some random misclassification is assumed, wheezing may play even more of a differentiating role than reported here. There was no significant difference between reported wheeze in those children with an IgE-negative or IgE-positive status at inclusion. Thus, children in families with a heightened awareness of atopy were not more likely to have reported wheeze and therefore have it recorded.
Ideally speaking, all children at follow-up should have had the same diagnostic procedures. However, in this study, asthma was defined as the presence of asthma-related symptoms and/or use of asthma medication in the previous 12 months, together with a positive histamine test result from the lung function test. This means that children without asthma-related symptoms or medication in the previous 12 months would be diagnosed as not having asthma. Therefore, in symptom-free children a lung function test was not performed because it did not have any additional value for the diagnosis of asthma.
Implications for research and clinical practice
In diagnostic cohort studies, in contrast to aetiologic studies, the emphasis is not on some exposure of interest whose influence is to be quantified and adjusted for confounding factors. Rather, the contrasts in patients' test results (where ‘tests’ include clinical history items) are used to predict the likelihood of asthma at a later point in time. This also implies that the analysis is centred around efficiency, that is, optimal prediction using information that becomes available early in the diagnostic work-up and is often virtually free of charge (such as clinical history). Next, the diagnostic impact of added information that does not come free of charge (laboratory testing, imaging) is estimated as conditional on the information already available. So, the issue of confounding in aetiologic cohorts becomes an issue of redundancy of diagnostic information in studies such as the current one.23
Ideally, a prediction rule should be derived, and then validated prospectively on a separate population. Although we used bootstrapping techniques, the results are likely to be somewhat less robust when applied to a separate population.24 The prediction rule, therefore, should be validated in another primary care population.
Assessment of specific IgE to inhalants may be helpful in determining those children with persistent cough (≥5 days) who will and will not develop asthma at the age of 6 years. In particular, children who wheeze may be usefully categorised into low- and high-risk groups. A simple scoring formula using wheeze and a family history of pollen allergy in coughing children who are younger than 5 years of age may support GPs in selectively ordering an IgE test.
Supplementary Material
Acknowledgments
The study was supported by a research grant from the Netherlands Asthma Foundation. We would like to thank the GPs, children, and their parents for participating in the study. We would also like to thank J de Vrieze for performing the RASTs and the Department of Immunochemistry at Sanquin for measuring albumin in the blood samples, SJA Lone-Latif for performing the lung function tests, and AGH Kessels for writing the bootstrap command.
Notes
Supplementary information
Additional information accompanies this article at http://www.rcgp.org.uk/journal/index.asp
Ethics committee and reference number
Medical Ethics Committee of the Academic Medical Center, University of Amsterdam. MEC 98/114
Funding and reference number
The Netherlands Asthma Foundation. 93.56 and 97.36
Competing interests
None
- Received December 19, 2003.
- Revision received March 29, 2004.
- Accepted July 12, 2004.
- © British Journal of General Practice, 2005.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

