


Abstract
Background Healthcare costs attributable to obesity have previously involved estimations based on costs of diseases commonly considered as having obesity as an underlying factor.
Aim To quantify the impact of obesity on total primary care drug prescribing.
Design of study Review of computer generated and handwritten prescriptions to determine total prescribing volume for all drug classes.
Setting Twenty-three general practice surgeries in the UK.
Method Stratified random selection of 1150 patients who were obese (body mass index [BMI]>30 kg/m2) and 1150 age- and sex-matched controls of normal weight (BMI 18.5–<25 kg/m2). Retrospective review of medical records over an 18-month period.
Results A higher percentage of patients who were obese, compared with those of normal weight, were prescribed at least one drug in the following disease categories: cardiovascular (36% versus 20%), central nervous system (46% versus 35%), endocrine (26% versus 18%), and musculoskeletal and joint disease (30% versus 22%). All of these categories had a P-value of <0.001. Other categories, such as gastrointestinal (24% versus 18%), infections (42% versus 35%), skin (24% versus 19%) had a P-value of <0.01, while respiratory diseases (18% versus 21%) had a P-value of <0.05. Total prescribing volume was significantly higher for the group with obesity and was increased in the region of two- to fourfold in a wide range of prescribing categories: ulcer healing drugs, lipid regulators, β-adrenoreceptor drugs, drugs affecting the rennin angiotensin system, calcium channel blockers, antibacterial drugs, sulphonylureas, biguanides, non-steroidal anti-inflammatories (NSAIDs) (P<0.001) and fibrates, angiotensin II antagonists, and thyroid drugs (P<0.05). The main impact on prescribing volumes is from numbers of patients treated, although in some areas there is an effect from greater dosage or longer treatment in those who are obese including calcium channel blockers, antihistamines, hypnotics, drugs used in the treatment of nausea and vertigo, biguanides, and NSAIDs (P<0.05) reflected in significantly increased defined daily dose prescribing.
Conclusions This large study of contemporary practice indicates that obesity more than doubled prescribing in most drug categories.
INTRODUCTION
The prevalence of obesity in the UK in 2001 reached 21% in males and 23.5% in females.1 As a result, widespread consequences include an impaired quality of life, increased social support and disability allowance for the social services budget, and an increased impact on healthcare resources. Despite consistent evidence for major clinical benefits from moderate weight loss and weight maintenance in large-scale and long-term studies,2–5 few resources are allocated to fund weight management in the primary care setting. Difficulty in establishing efficacious obesity management in primary care has been highlighted by the Brief Intervention Obesity (BIO) project, which recently reported the failure of a 4.5-hour training programme for GPs and practice nurses to achieve weight loss in participating patients.6
How this fits in
As healthcare costs continue to rise, much attention has been placed on ensuring good prescribing practice to optimise patient care within available resources. Previous estimates have given an indication of the influence of obesity on healthcare costs but none has documented evidence on the full impact this disease has across clinical areas including those not normally associated with being obese. This study has used a new approach based on defined daily doses to begin to clarify the extent of the problem.
Potential obstacles to providing weight management within normal health care include a lack of awareness of the extent of ill health attributable to obesity and of the multiple benefits of modest weight loss (5–10% of body weight), plus a perceived cost of intervention. Costs of some experimental interventions have been high, but the marked health benefits may be achievable by well-designed, cheaper interventions within routine care.3,4,7,8 The economic case for incorporating weight management within a healthcare service will depend on the balance between the costs of intervention versus potential cost savings from the reduced need to treat obesity-related comorbidities.
The costs of obesity in a variety of countries have been estimated at 4–8% of total healthcare budgets, mainly from the increased prevalence of comorbid conditions and general costs of their management.9–12 Direct costs of obesity were estimated at around £500 million plus indirect costs of around £2.1 billion in 1998 in England.13 A large proportion of these healthcare costs arise from drug prescriptions: around 25% of primary care trust (PCT) budgets have been spent on prescribing14 and drug costs absorb most of the non-fixed costs of primary care. As pressure builds on NHS resources, a number of recommendations have been made, which aim to benefit patients and generate savings in prescribing budgets;14 the balance of costs around obesity and weight management, however, have not been included.
The World Health Organisation (WHO) system of defined daily dose(s) (DDD[s]) reliably measures drug volume15 (Supplementary Appendix 1). Other studies assessing prescribing volume have used this method.16,17 The Counterweight Project7 included a baseline survey of medical practice that aimed to establish:
whether the population that is obese receives a greater volume of prescribing than age- and sex-matched controls of normal weight in terms of i) numbers of patients treated, and ii) volume per patient treated;
factors affecting prescribing rates, for example presence of comorbid conditions; and
the effect of an increasing degree of obesity on prescribing.
METHOD
Programme methodology
Practice recruitment and centres involved
The Counterweight Project methodology is published in detail elsewhere.7 Counterweight is being conducted in seven regions around the UK and was launched in March 2000. Participating practices were chosen from those who volunteered in response to letters of invitation offering assistance, which aimed to establish an effective weight management service within current practice resources. Counterweight consists of four phases:
baseline medical practice review;
support and training;
establishment of weight management programme; and
evaluation and feedback.
Data used for this paper were taken from the baseline review.
Baseline medical practice review
In each of the 30 practices recruited, stratified systematic random sampling was used to select 50 subjects who were obese (body mass index [BMI]>30 kg/m2) and 50 age- and sex-matched subjects of normal weight (BMI 18.5–<25 kg/m2). It was not possible to conduct the review in seven practices because of data protection issues or limited availability of data on computerised records. Data were, therefore, available from 23 practices. The total sample was 1150 subjects of normal weight and 1150 subjects who were obese. The practices were spread geographically across the UK, with address post codes indicating a wide range of populations from the affluent to the socially deprived.
Computerised and paper-based medical records were reviewed. Data were collected on every prescription issued over an 18-month period and included drug, dosage, number of prescriptions and quantity of drug in each prescription. The 18-month time frame was chosen to ensure inclusion of data that would be affected by annual reviews (such as diabetes), recognising that such reviews are commonly delayed by missed appointments or holidays. Due to variations in start dates of the reviews between centres, data collection started on 1 April 2000 and was completed on 6 September 2002.
For analytical purposes each drug audited was given an individual code and also coded according to main prescribing categories as listed the British National Formulary (BNF) (Supplementary Appendix 2). For some drug categories, sub-sections were also coded to allow for analysis in more detail. For example, the category of cardiovascular disease was broken down to allow analysis of antihypertensive drugs, then further subdivided to look at drug classes such as β-blockers. Trade names were ‘mapped’ onto their root drug.
Initial analysis examined the total number of patients who had no drugs or who received at least one drug from the 15 BNF prescribing categories over the 18-month audit period. In cases where a patient received an antihypertensive and a lipid regulator this would be counted as one patient receiving at least one drug from the cardiovascular category. To assess the impact of obesity on ‘polypharmacy’, the number of patients receiving at least four different root drugs over the 18-month period was calculated.
Prescribing volume was assessed using the WHO system of DDD(s). The DDD for each drug was entered and the drug sub-groups were analysed according to BNF sub-categories. Total DDD(s) were assessed for the groups of patients who were of normal weight and obese for each prescribing category.
To quantify the impact of obesity on prescribing rates in various drug categories we applied a ratio of prescribing volume; total DDD(s) for the population that was obese were divided by the total DDD(s) for the population of normal weight.
Data were collected on patients recorded as having ‘major’ comorbidities and ‘any’ comorbidity. These data were taken from computerised medical records and paper-based patient summaries including information from secondary care communications. Major comorbidities were those commonly accepted as having obesity as a contributory factor. Any comorbidity included the major comorbidities plus those clinical conditions also associated with or exacerbated by obesity, but hitherto not included in health economic analysis of the impact of obesity on healthcare resources (Supplementary Appendix 3).
Statistical methods
Probability values for the comparison between the percentages of patients who were obese and of normal weight who received at least one drug from each of the BNF categories were derived from a logistic regression analysis, with adjustment firstly for age group, sex, deprivation category, and country and, secondly, for the same four factors plus the presence of any comorbidity in that subject. Comparisons between total DDD(s) prescribed per patient for the both groups and for the volume of drug prescribed to each patient who received the relevant drug were carried out using the Mann-Whitney U test, to allow for non-normality of the DDD distribution. Analysis of the distribution of the number of root drugs prescribed for patients who were obese and of normal weight were carried out using the χ2 test for trend. Factors associated with the probability of a patient being prescribed four or more drugs were identified using logistic regression analysis in a two-stage procedure, initially excluding and then including the presence of comorbidity in the statistical model.
RESULTS
Drug prescribing
Table 1 shows the numbers and percentage of patients who were obese and of normal weight who received prescriptions during the 18-month audit period in each of the main BNF prescribing categories. Significantly more patients of normal weight (23.5% versus 16.0%; P<0.001) had received no prescriptions compared with those who were obese. In no prescribing categories were there significantly more prescriptions in the normal weight patients. For eight of the 15 BNF prescribing categories, significantly more prescriptions were made to obese patients after adjustment for age, sex, deprivation category, and country. Eight were still more often prescribed after adjusting for the presence of obesity-related comorbidities (P<0.05). A number of sub-categories of interest where DDD analysis was not possible were also prescribed to significantly greater numbers of obese patients including codeine preparations, anti-platelet drugs, corticosteroids, diuretics, drugs used for the relief of soft tissue inflammation, and drugs used in the treatment of rheumatic disease and gout.
Percentage of patients (obese and normal weight, each n = 1150) receiving prescriptions from each of the 15 main BNF prescribing categories during the 18-month period.
Defined Daily Doses
For a more complete reflection of prescribing volume over the 18-month audit period, total DDD(s) were calculated for all BNF prescribing categories for which DDD values were available. These results, shown in Table 2, reveal significantly higher prescribing volumes in those patients who were obese for a wide range of drug classes. For all drug groups, except selective serotonin re-uptake inhibitor (SSRI) antidepressants, antispasmodics and anion exchange resins, numerically more DDD(s) were prescribed to patients who were obese than to those age- and sex-matched controls of normal weight. This was significant for 14 out of the 25 drugs groups shown in Table 2. Table 2 also shows the ratio of total DDD(s) of the patients who were obese to those of normal weight for the drugs with a significantly different DDD (P<0.05). The prescribing ratio for most drug classes was at least 2.
Total defined daily doses prescribed during an 18-month observation period within BNF prescribing categories for patients who are obese and age- and sex-matched controls.
A closer examination of prescribing practice was conducted to examine the DDDs prescribed to each individual patient who received that drug group. The results in Table 3 show that in six drug classes, significantly greater drug volumes (P<0.05) were prescribed to the individuals who were obese receiving the drug than to the patients of normal weight receiving the drug. These findings should, however, be interpreted with caution because of multiple testing.
Defined daily dose values per patients who are obese and those of normal weight who received drugs from specific categories.
Polypharmacy
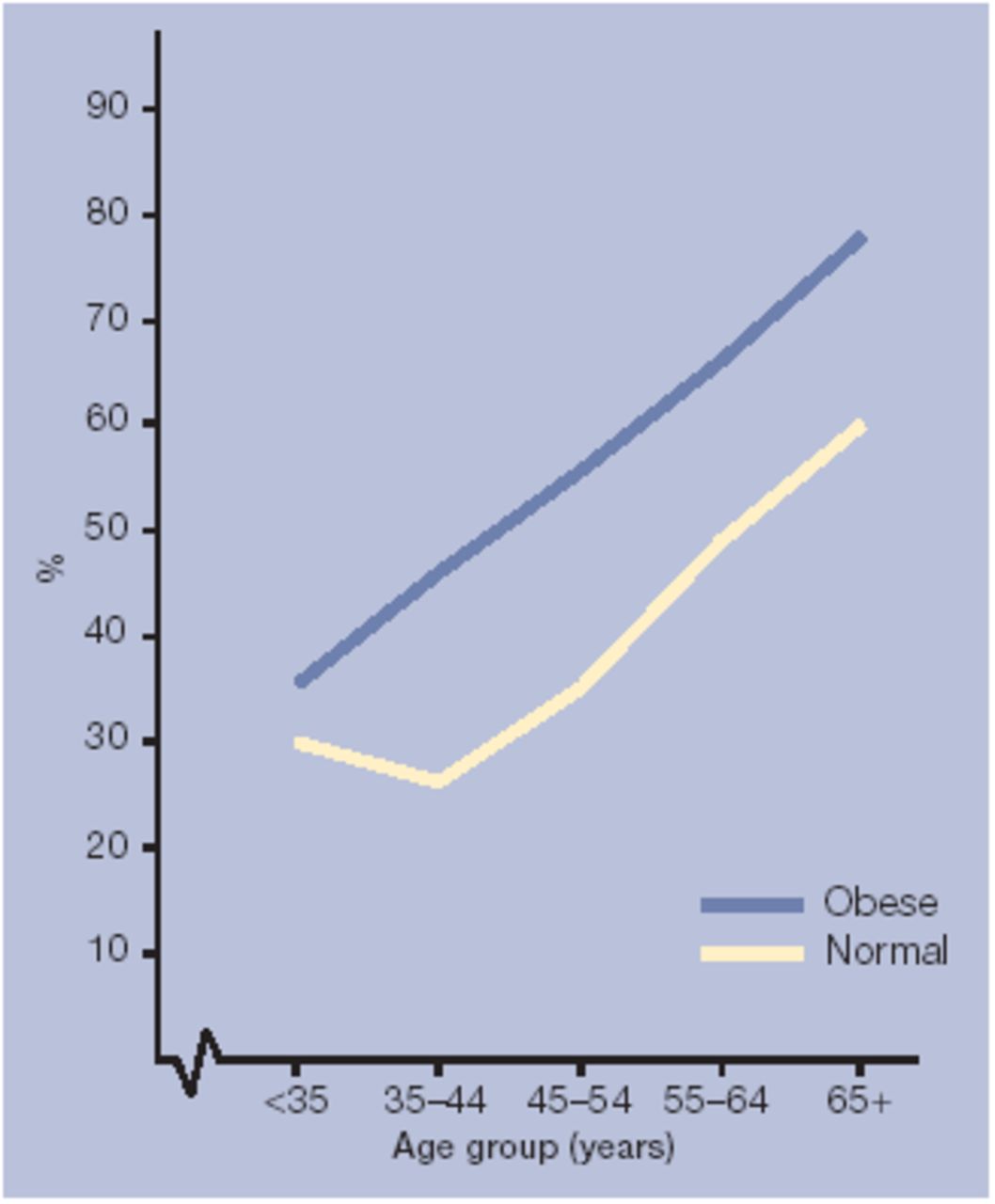
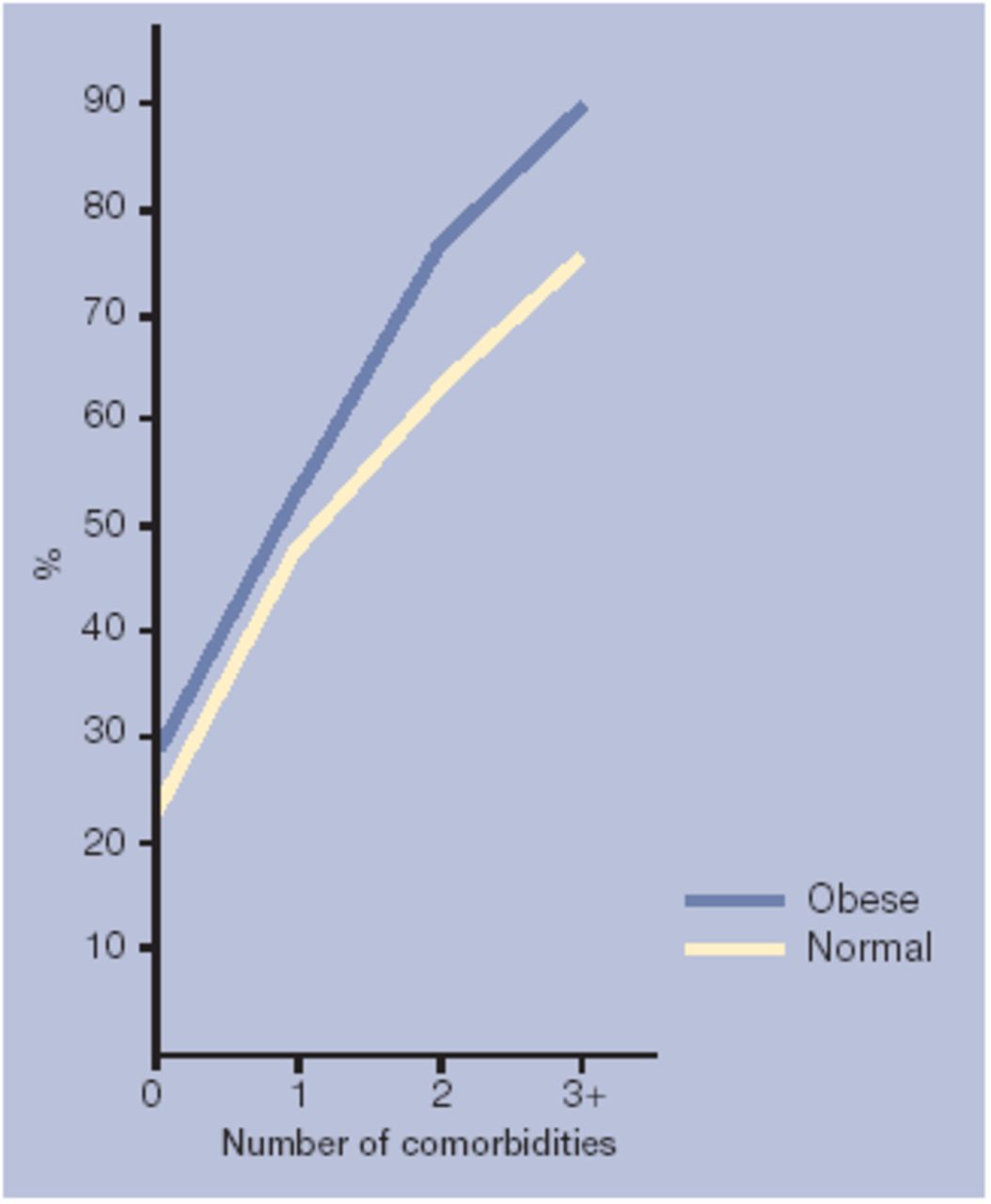
Table 4 shows that, for the most part, larger numbers of root drugs were prescribed to patients who were obese than those of normal weight (P<0.001). Four or more root drugs were prescribed over the 18-month audit period to 615 (53.5%) patients who were obese compared with 436 (37.9%) patients of normal weight. Figure 1 illustrates the additional impact of increasing BMI over and above the effect of increasing age on prescribing volume and Figure 2 illustrates the impact with an increasing number of comorbidities.

Prevalence of polypharmacy defined as >4 drugs during an 18-month period by body mass index status and age group.

{kind=link}
{kind=link}
Prevalence of polypharmacy defined as >4 drugs during an 18-month period by body mass index status and number of comorbidities (see Supplementary Appendix 3).
Number and percentage of obese and normal weight patients receiving root drugs over the 18-month audit period.
Degree of obesity
Table 5 shows that among patients with BMI ≥30 kg/m2, increasing degrees of obesity increase prescribing rates even after taking into account various other factors which were also found to impact on prescribing (age, sex and deprivation category as well as the presence comorbid conditions). There was no significant difference between prescribing in England or Scotland.
Logistic regression analysis to generate odds ratios for being prescribed four or more root drugs during an 18-month period using data from normal and obese patients (combined) adjusted for all other factors.
DISCUSSION
Summary of main findings
About 80% of all registered patients aged 18–75 years received at least one prescription in this 18-month period with patients of normal weight being 50% more likely to have no medications in the 18-month audit period.This is likely to be reflected in differences in rates, duration, and content of medical consultations.
More patients who were obese received drugs from the main prescribing categories than the age- and sex-matched controls of normal weight. The range of prescribing areas being affected by obesity was striking, reflecting the frequent presence of multiple comorbidity. It is well recognised that obesity affects categories such as cardiovascular disease, endocrine, and the musculoskeletal system. Increased prescribing to those who were obese in categories such as gastrointestinal, infections, and skin are not those which most clinicians would typically expect to be associated with obesity. These findings demonstrate the wide range of clinical conditions for which obesity is a contributory factor and for which there is an increased healthcare requirement.
The DDD data confirm that most of the prescribing attributable to obesity is due to the increased number of patients who receive prescriptions. Drugs such as codeine preparations, which have no DDD allocated, were also found to be prescribed to significantly greater numbers of the population that was obese. However, the volume of prescribing per affected patient was also significantly higher in those who were obese for antihistamines, drugs used in the treatment of nausea and vertigo, non-steroidal anti-inflammatories (NSAIDs), calcium channel blockers, hypnotics, and biguanides; multiple testing may, however, have produced one spurious result. Obesity, therefore, affects prescribing volume both at a population and individual patient level. The classes of drugs apparently affected by obesity are of interest; hypnotics are likely to be prescribed in larger quantities in relation to sleep disorders associated with obesity and NSAIDS due to lower back pain and musculoskeletal pain, but the increased dosages of antihistamines and drugs used in nausea and vertigo are less easily explained.
Comparison with existing literature
The higher prescribing levels in the patients who were obese is largely explicable in terms of medical conditions known to be increased in such individuals, but in some cases there may be multiple interactions. For example, more frequent prescriptions of antibacterial drugs in those who are obese are likely to be accounted for by more frequent chest, skin, and urinary tract infections. These are also likely to be more frequent in people with diabetes, who are over-represented among the population that is obese. It is noteworthy that seven prescribing categories not found to be affected by obesity (obstetrics and gynaecology; malignant disease; nutrition and blood; eye; ear, nose, and throat; vaccines; and anaesthesia) are relatively unimportant as far as healthcare expenditure is concerned. The total budget for these six categories for primary care prescribing in 2002 accounted for less than 13% of the total prescribing budget,18 whereas the prescribing categories that we have found to be significantly (P<0.05) affected by obesity formed 87% of primary care prescribing. Obesity, therefore, increased drug prescribing in all the most expensive prescribing categories.
The figures obtained in this study reveal a wider spread of costs attributable to obesity than previously known, in one of the most costly areas of medical practice. The data, therefore, provide further support for the view that the early management of obesity, rather than the late treatment of its multiple consequences, should underpin quality health care. The exaggerated healthcare requirement, which results from increasing BMI, is shown clearly in the data in Table 5 and Figures 1 and 2. The presence of cardiovascular risk factors has a major impact on prescribing independent of BMI. However, even after adjusting for the presence of hypertension, diabetes, dyslipidaemia, cardiovascular disease, or stroke, there remains a highly significant augmentation of attributable prescribing volume as BMI rises from 30 to over 40 kg/m2, to which other diseases contribute.
These data confirm the inextricable pathophysiological effect obesity has in relation to a wide range of clinical conditions that are largely managed pharmacologically with major cost implications. This study strengthens the economic case for weight management to be high on healthcare agendas, particularly now that effective low-cost interventions are being developed for the primary care setting.3,4,7
Strengths and limitations of the study
The data form the largest UK set of cross-sectional data on medical practice in relation to obesity. This study reflects current prescribing patterns in the UK and there are several reasons to believe that the results are representative of routine practice across the country. The populations served by the practices recruited showed a socioeconomic profile similar to that of the whole UK. There are, however, some limitations within the data. It is not possible to exclude some bias as a result of practices involved being motivated to take part in an obesity audit. Only 60–70% of patients in the Counterweight practices had their heights and weights recorded, to be able to calculate BMI. As such, about 30% of all patients were not available for audit. These will include fit people, who have never seen their doctor, and patients who are disabled and housebound, who may have heavy drug usage. Also excluded would be some patients with morbid obesity where weight checks may not be possible with equipment routinely available in the primary care setting. It is not possible to say if any net bias resulted from failing to include these patients. Although based on UK data the principles of this work will be universal.
Expressing volume of drug prescriptions as multiples of DDD is an increasingly accepted method for measuring prescribing volume and allows more detail than is provided by previous analyses using estimates of patients treated. It has not previously been applied to obesity. This method is the only way to prove our prejudice that the greatest impact on prescribing volume is on numbers of patients treated — without analysis of DDDs this fact would not be scientifically established. It is the only available method that can identify where increased volume of prescribing is the result of higher dosage or more prolonged treatments.
Implications for clinical practice and future research
The study provides new information that should be of value to clinicians, health service strategists, and health economists regarding the impact of obesity on primary care drug prescribing.
Although causality is not proved in the present study, there is ample supporting evidence to suggest that early correction of obesity or prevention of excess weight gain would help slow down the spiralling drug costs associated with obesity and its clinical consequences.
Supplementary Material
Acknowledgments
This paper was written by Mike Lean, E Louise McCombie and David J Hole with contributions to study design, analysis and/or writing from other authors.
Thanks go to Billy Sloan, data manager/computer programmer for the development of the drug dictionary and data handing methods that enabled analysis of the drug information including defined daily dose data. Thanks also go to all staff in each general practice involved in the study, particularly those assisting with the retrieval and filing of medical records. Dr Andrew Power, Audrey Thompson and Margaret Mackie, Medicines Management Advisers, Greater Glasgow Primary Care Trust are given thanks for advice on drug data collection and analysis.
Notes
Supplementary information
Additional information accompanies this article at http://www.rcgp.org.uk/journal/index.asp
Funding body
Educational grant-in-aid from Roche Products Ltd with no contractual or other obligations to the sponsoring company. Intellectual property rights reside with the Counterweight Project Team
Ethics committee
West Midlands Multi-Centre Research Ethics Committee (99/7/74); Grampian Research Ethics Committee (00102); Bath Local Research Ethics Committee (BA14/00-01); Solihull Local Research Ethics Committee (P22/00); Greater Glasgow Community/Primary Care Local Research Ethics Committee (43/00); Hammersmith Research Ethics Committee (2000/5870-M); Leeds Local Research Ethics Committee (MC. 00/049); South Bedfordshire Local Research Ethics Committee (May00/4b)
Competing interests
John Broom, Sudesh Kumar, Mike Lean, Julian H Barth and Nick Finer have received lecture honoraria. Helen Gibbs, John Broom, John Reckless, Paula Noble, Sudhesh Kumar, Louise McCombie, Mike Lean, Felicity Lyons, Marney Quinn, Julian H Barth, Sarah Haynes, Nick Finer and Hazel Ross have attended national/international meetings as guests of Roche Products Ltd. Mike Lean, Julian H Barth, and Nick Finer have been involved as above with other pharmaceutical companies with an interest in obesity. Gary Frost and Nick Finer have received research grants, and Hazel Ross is employed by Roche Products Ltd., but reports to the Counterweight Project Board.
- Received May 19, 2004.
- Revision received August 13, 2004.
- Accepted February 18, 2005.
- © British Journal of General Practice, 2005.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

