


Abstract
Background Anxiety disorders are prevalent in primary care. Psychological treatment is effective but time-consuming, and there are waiting lists for secondary care. Interest has therefore grown in developing guidelines for treatment that would be feasible in primary care.
Aim To compare the effectiveness and feasibility of guided self-help, the Anxiety Disorder Guidelines of the Netherlands College of General Practitioners and cognitive behavioural therapy (CBT).
Design of study Randomised controlled study lasting 12 weeks with follow-up at 3 and 9 months for primary care patients with panic disorder and/or generalised anxiety disorder.
Setting The first two forms of treatment were carried out by 46 GPs who were randomly assigned to one or the other form. CBT was carried out by cognitive behaviour therapists in a psychiatric outpatient clinic.
Method Participants (n = 154) were randomly assigned to one of the three forms of treatment. The main outcome measure used was the state subscale of the Spielberger Anxiety Inventory.
Results All three forms of treatment gave significant improvement between pre-test and post-test, and this improvement remained stable between post-test and the follow-ups. The results obtained with the three treatment forms did not differ significantly over time. The feasibility of the Anxiety Disorder Guidelines was low compared with that of guided self-help.
Conclusion Our results indicate that primary care patients with prevalent anxiety disorders for whom the GP does not find referral necessary can be adequately treated by the GP. Psychiatric outpatient clinic referral does not give superior results. Guided self-help is easier for the GP to carry out than a less highly-structured treatment like that laid down in the Anxiety Disorder Guidelines.
INTRODUCTION
The World Health Organisation study on psychological problems in general health care demonstrated a 10.1% prevalence rate for anxiety disorders.1 As a consequence, GPs often see these disorders in their patients. The most common forms are panic disorder, with or without agoraphobia, and generalised anxiety disorder.2 GPs often treat anxiety disorders with antidepressants or benzodiazepines. These drugs are effective but have several disadvantages, including the risk of dependency, side-effects and poor patient compliance. Furthermore, anxiety symptoms often recur when the drugs are discontinued.3,4 These disadvantages are irrelevant in treatment programmes based upon cognitive and behavioural principles. However, such programmes are usually not suitable for primary care because they are time-consuming and require extensive training of the therapist. Most research into the efficacy of cognitive behavioural therapy (CBT) has taken place in secondary care settings.5–7
In order to stimulate the use of simple cognitive behavioural techniques in primary care, the Netherlands College of General Practitioners recently developed guidelines for the treatment of anxiety disorders. The efficacy and feasibility of these guidelines is yet to be evaluated.8
Another development in the treatment of anxiety disorders in primary care is the use of self-help manuals based on cognitive behavioural techniques. Self-help treatment appears to be effective in both the short and the long term.9 However, the interpretation of these results has so far been hampered by small patient samples and the failure to use appropriate diagnostic criteria for the anxiety disorders studied.10,11 In addition, the effectiveness of self-help manuals for anxiety disorders in primary care has not been compared with that of CBT in secondary care, which may be considered the gold standard in this field.
How this fits in
Since the prevalence rate of anxiety disorders in primary health care is 10%, GPs frequently come into contact with patients with anxiety disorders. This study found that in primary care patients with anxiety disorders can be adequately treated by their GP with a guided self-help manual and treatment according to the Anxiety Disorders Guidelines of the Netherlands College of General Practitioners (NCGP). Referral to a psychiatric outpatient clinic for cognitive behavioural therapy does not give superior results for these patients. Treatment with the NCGP's guidelines was effective, but harder to perform than the guided self-help manual because the guidelines appeared to be difficult to follow and too time consuming for GPs.
The purpose of this study is to compare the effectiveness and feasibility of a self-help manual for anxiety disorders used by the patient under the direction of the GP (referred to from now on as ‘manual’) with CBT carried out by experienced cognitive behaviour therapists in secondary care. These two forms of treatment were further compared with the Anxiety Disorders Guidelines of the Netherlands College of General Practitioners (referred to henceforth as ‘guidelines’). Since the three treatments differed mainly in the intensity and complexity of the cognitive behaviour techniques used, we hypothesised that the most intensive form (CBT in secondary care) would give the best results, followed by ‘manual’ and with ‘guidelines’ as a significantly poorer third.
METHOD
Design
The effectiveness of the three treatments for panic disorder and generalised anxiety disorder was compared in a 12-week study with a 12-week treatment-free follow-up period. After that the patients were given conventional treatment tailored to their needs. Follow-up 1 was scheduled 24 weeks after pre-test, and follow-up 2 was 52 weeks after pre-test. The patients were randomly assigned to one of the following three forms of treatment: use of the self-help manual under the guidance of the GP; CBT, given in a psychiatric outpatient clinic by experienced cognitive behavioural therapists; and Anxiety Disorder Guidelines implemented by the GP.
Subjects and recruitment
The participants, all aged over 18 years, were recruited from 46 general practices in rural and urban areas of the Netherlands. GPs identified possible panic disorder or generalised anxiety disorder with the aid of the Short and Simple Screening Interview (SSI).12 If the SSI score was 5 or more, participants were invited for a diagnostic interview using the Structured Clinical Interview (SCID-IV) technique described in the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).13 The participants were asked to participate in the study when the results of this interview showed that they met the criteria for panic disorder or generalised anxiety disorder. Exclusion criteria were the presence of an organic mental disorder; mental retardation or a psychotic disorder; treatment of anxiety disorders in the recent past; use of antidepressants or the use of more than 30 mg oxazepam equivalents daily. After a full explanation of the study procedures, participants gave written informed consent.
Sample size and randomisation
The participating practices (n = 46) were first randomly assigned in a ratio of 1:1 to ‘manual’ or ‘guidelines’ as a primary care method.14 Next, within each practice, patients were randomly assigned to primary or secondary care in a ratio of 2:1. For both randomisations a computerised randomisation scheme was used. In both randomisation procedures (primary care practices and participants) the assignments were put in sequentially numbered, sealed, opaque envelopes by an independent statistician. At the start of the study the first author opened the envelopes for the participating practices. During the study the first author opened the envelopes after participants had given their informed consent.
Our aim was to find a medium ‘effect size’ (corresponding with a 5.5 point difference) on the state subscale of the Spielberger State-Trait Anxiety Inventory (STAI) between the treatment conditions. This effect size required a sample size (α = 0.05; two-sided β = 0.20) of 50 participants in each group. This estimated effect size was corrected for the difference between the two follow-up measurements (within-person correlation assumed to be 0.7) and the variation within GP groups (within-GP correlation assumed to be 0.2), using an assumed standard deviation of 10.15,16
It was found during the study that the practices randomly assigned to ‘manual’ treatment had on average twice as many patients as those assigned to ‘guidelines’. As a consequence, there was an unintended difference in size between the three study groups. Having consulted an independent statistician, the authors decided halfway through the study to change the primary care:secondary care randomisation ratio in the practices offering ‘manual’ from 2:1 to 1:2. Since this change could yield biased results because the equivalence of the treatment and control groups is relaxed, we analysed post-hoc whether the differences in inclusion and outcome before and after the change in the randomisation ratio critically affected our results. This did not appear to be the case. We did not find significant pre-test differences in demographic and clinical status variables, nor post-test differences in outcome.
Treatment
All participants received individual treatment for 12 weeks based on cognitive-behavioural principles. The three treatments differed mainly in intensity and complexity. GPs and therapists received relevant training. The GPs were present at two educational meetings on diagnosis and treatment of anxiety disorders. Supervision was provided by the first three authors every 2 months during the study. The cognitive behavioural therapists, all with extensive experience in the treatment of anxiety disorders, received weekly supervision from the fourth author.
Self-help treatment consisted of five 20–minute sessions. In the first session, the GP informed the participant about the contents of the manual, which comprised an explanation of the basic facts about anxiety, simple cognitive techniques, and relaxation and in vivo exposure exercises. The participants put the self-help techniques learnt from the manual into practice for 3 hours a week. In subsequent sessions, the GP reinforced the patient's achievements and motivated him or her to continue with the use of the manual.17
CBT comprised 12 45-minute sessions. The participants practiced for 3 hours a week. They received a CBT handbook explaining the basic facts about anxiety and the rationale of CBT, identifying anxiety-provoking cognitions and showing the patient how he or she can challenge these cognitions by means of a Socratic dialogue and replace them by more realistic and rational cognitions. The credibility of catastrophic cognitions was tested with the aid of behavioural experiments, and in vivo exposure exercises were given.18–20
‘Guidelines’ was the least structured form of treatment, and consisted of a very simple form of CBT. The GP was free to choose the number of sessions and the type of intervention, but was advised to start with an explanation about the nature of anxiety followed by reassurance, simple cognitive techniques and in vivo exposure. The GP was allowed to refer the patient for relaxation exercises or psychiatric treatment and to prescribe antidepressants or benzodiazepines.8
Measurements
Participants filled out questionnaires at four points in time during the study, to provide a measure of the presence and severity of psychopathological symptoms associated with panic disorder or generalised anxiety disorder: pre-test (immediately after informed consent had been given), post-test after 12 weeks, follow-up 1 after 24 weeks and follow-up 2 after 52 weeks.
Since the severity of anxiety is the psychopathological parameter most widely used in the diagnosis of panic disorder and generalised anxiety disorder, the state subscale of the STAI was used to determine the primary outcome measure.21 The following secondary outcome measures were: the trait subscale of the STAI and the Lehrer-Woolfolk Anxiety Symptom Questionnaire (LWASQ)22 as measures of ‘anxiety’; the Penn State Worry Questionnaire23 as a measure of ‘worry’; the Bodily Sensations Questionnaire and the Agoraphobic Cognitions Questionnaire24 as measures of ‘panic’; the agoraphobia scale of the Fear Questionnaire25 as a measure of ‘avoidance’; the Beck Depression Inventory;26 the General Health Questionnaire-12;27 and finally the Sheehan Disability Scale28 was used as a measure of ‘social adjustment’.
Statistical analysis
The three treatments were compared at pre-test for differences in demographic and psychiatric status variables. Outcome analyses were performed on an intent-to-treat basis. If an outcome value was missing, the pre-test value was used to replace the post-test, follow-up 1 or follow-up 2 value. The analyses were repeated after excluding the dropouts.
Primary and secondary outcome measures were subjected to analysis of variance (ANOVA) using the General Linear Model with 3×2 repeated measures, with the three groups as between-subjects factor and the two evaluations (pre-test and post-test) as within-subjects factor. The between-subjects factor was further broken down into two Helmert contrasts. The first contrast compared the mean change from pre-test to post-test scores for CBT and ‘manual’ with that for Guidelines. The second contrast compared the mean change from pre-test to post-test scores for CBT with that for ‘manual’. These analyses were repeated on the mean change from pre-test to follow-up 1 and from pre-test to follow-up 2. Significant time effects for the primary and the secondary outcome measures were further analysed by means of paired t-tests (pre-test versus post-test; pre-test versus follow-up 1 and pre-test versus follow-up 2) for each group separately. All statistical tests were two-tailed at α = 0.05, unless multiple test were performed, in which case α was divided by the number of tests (Bonferroni correction). Data analyses were conducted using SPSS 11.0.
RESULTS
Recruitment and attrition
Figure 1 shows the variation of the total trial population during the study and the reasons for dropping out. Completers and dropouts were evenly distributed over the three treatment groups (P>0.67).

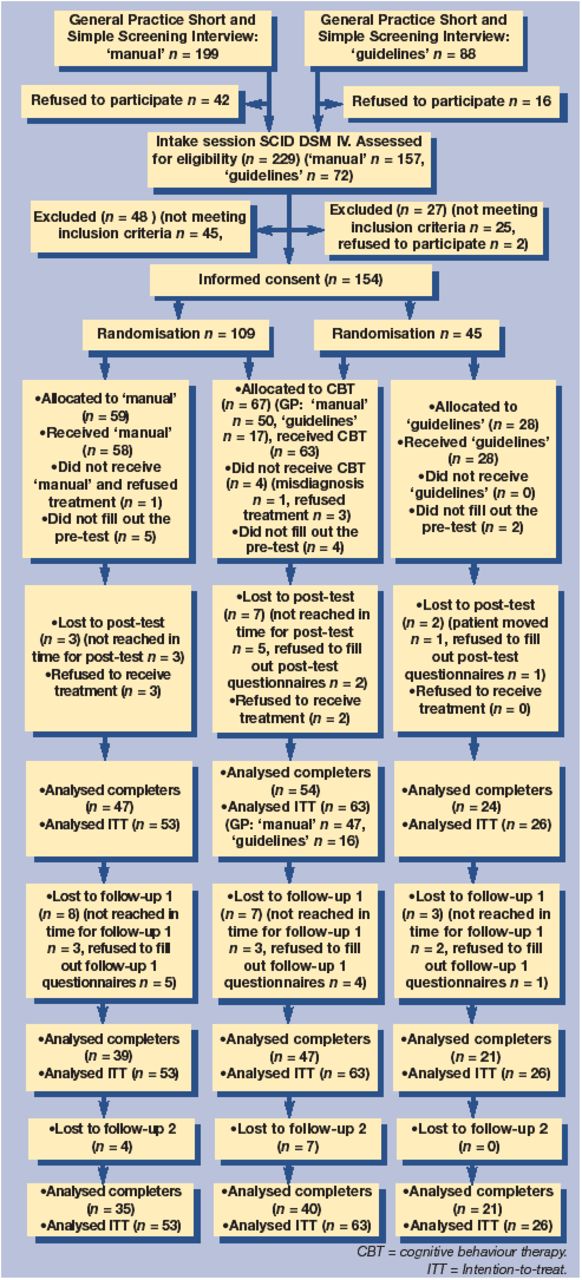{kind=link}
Recruitment to analysis.
Characteristics of the participants
Pre-test demographic characteristics and psychiatric status variables of the study sample are presented in Table 1 and 2. No statistical differences were found between the various treatment groups, and no significant differences were found between dropouts and completers at pre-test.
Baseline demographic characteristics of the study group.
Pre-test, post-test, follow-up 1 and follow-up 2 clinical characteristics of study group (intention-to-treat sample).
Outcomes
In the intent-to-treat sample, application of Helmert contrasts to the STAI state scores did not reveal significant differences between the two test points (pre-test versus post-test; pre-test versus follow-up 1; and pre-test versus follow-up 2) or between the CBT and ‘manual’ treatments on the one hand and ‘guidelines’ on the other (between pre-test and follow-up 2: effect size 0.06; 95% confidence interval [CI] = −5.3 to 2.5). No significant differences were found between CBT and self-help treatment (between pre-test and follow-up 2: effect size 0.03; 95% CI = −4.2 to 6.3). The same held for the analyses of the completer sample. Helmert contrasts yielded the same pattern of results for the secondary outcome measures (data not shown, the complete data can be obtained from the corresponding author). The three groups all improved significantly from pre-test to post-test, pre-test to follow-up 1 and pre-test to follow-up 2 on all outcome measures. No significant differences were found between post-test and follow-up 1 or follow-up 2.
GPs’ views on the feasibility of self-help (‘manual’) and ‘guidelines’ treatment
GPs randomly assigned to the ‘manual’ treatment group were much more active in putting participants forward for the study than those assigned to ‘guidelines’. Although 23 GPs participated in both treatment groups, 17 in the ‘guidelines’ group put forward a total of 88 possible participants while 19 GPs assigned to the ‘manual’ group put forward a total of 199 participants. All GPs were interviewed to identify the disincentive factors that were operative. Most GPs stated that they felt unable to carry out even the simplified CBT laid down in the ‘guidelines’, and that the time investment needed was too high. As a result, half of the participants were treated with antidepressants, and one third were referred to secondary care. The mean number of visits to the GPs in the 12-week treatment period was 5.4 (standard deviation = 3.3).
DISCUSSION
Summary of main findings
It may be concluded that panic disorder and generalised anxiety disorder can be effectively treated in primary care by a GP using the ‘guidelines’ or ‘manual’ method and by experienced cognitive-behaviour therapists in secondary care. We could not confirm our hypothesis that the effectiveness of the treatments was directly related to the complexity and intensity of the form of CBT given. The three treatments did not differ significantly in reducing anxiety and associated symptoms. The major part of the improvement was realised in the first 12 weeks of the study. The GPs in the ‘guidelines’ group referred less than half as many participants to the study than the GPs in the ‘manual’ group, as they knew there was a chance that their patients would be assigned to the ‘guidelines’ treatment, which they would then have to deliver. The feasibility of ‘guidelines’ was rather low, because the GPs concerned felt incapable of delivering it or found it too time-consuming. It appeared that about half of the patients did not actually receive the intended CBT. Instead, they were treated with antidepressants and/or referred to secondary care. The gold standard, CBT in secondary care carried out by experienced therapists, was, however, not superior to the treatments carried out by GPs. Primary care patients with anxiety disorders, when the GP does not consider referral to secondary care necessary, can receive optimal care from their GP. A more intensive secondary care treatment does not improve the outcome.
Strengths and limitations of the study
The results of this study suggest that ‘manual’ may be a feasible and effective treatment for panic disorder and generalised anxiety disorder in primary care. The effectiveness of self-help treatment was comparable to that of the gold standard: CBT performed by professionals in secondary care. The improvement brought about by self-help treatment was maintained during 40 weeks of follow-up. Our results can be generalised to primary care patients with panic disorder and generalised anxiety disorder. Case finding in this study was performed by the GP during normal practice, instead of screening general practice patients in the waiting room. Moreover, the anxiety disorders in this study were diagnosed in a valid way by means of a structural interview.
A limitation of our study was the low feasibility found for the Anxiety Disorder Guidelines. As a consequence, the sample size in this group only reached half the size originally intended. Therefore, it is difficult to draw definite conclusions about this intervention. We do not think, however, that the inclusion of only 26 participants from this group in the study population has led to a type II error (failure to reject a false null hypothesis). Inspection of the data and the confidence intervals did not reveal any differences between the three treatment groups that may have become significant if the sample size had been larger. To avoid further divergence of the size of the cells, we decided halfway through the study to change the randomisation ratio in practices randomly assigned to the ‘manual’ treatment group. We cannot rule out the possibility that this change in the randomisation ratio has biased our results. However, such bias seems unlikely as no differences were found in post-hoc statistical analyses before and after this intervention.
Comparison with existing literature
The finding that CBT in secondary care was not superior to self-help treatment was rather unexpected. Our study is the first in which these two treatments were compared in a single trial. The lack of difference found between CBT and self-help might be due to the fact that participants in both groups were given an equal number of hours of homework, or to the fact that the patients treated are taken from primary care, and therefore would have relatively mild complaints for which formal CBT may represent ‘over-treatment’. Another unexpected finding was the effectiveness of the Anxiety Disorder Guidelines. However, more than half of the patients assigned to this treatment group did not in fact receive this simple form of CBT but were given antidepressants or referred to secondary care. While ‘guidelines’ may be suitable for motivated GPs, it seems that in the Netherlands most GPs do not have the affinity with or knowledge of this approach — or the time — to give even simple CBT exercises to their anxiety disorder patients.
Implications for clinical practice
Our results indicate that primary care patients with panic disorder and generalised anxiety disorder may be treated effectively by the GP and that referral to psychiatric outpatient clinic does not yield better results. Moreover, self-help treatment is easier to carry out by a GP than a less structured treatment such as the Anxiety Disorder Guidelines, and results in fewer referrals to specialised care.
Notes
Funding body
Nederlandse Organisatie voor Wetenschappelijk Onderzoek (0703/AGIKO/920-03-026)
Ethics committee
The Medical Ethics committee of the VU University Medical Centre (95/174)
Competing interests
None.
- Received September 6, 2004.
- Revision received December 1, 2004.
- Accepted February 4, 2005.
- © British Journal of General Practice, 2005.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

