


Abstract
Background There is a high non-attendance rate for traditional clinic-based routine asthma care in general practice. Alternative methods of providing routine asthma care need to be examined.
Aim To examine the cost and effectiveness of targeted routine asthma care in general practice using telephone triage, compared to usual clinic care.
Design of study An open randomised controlled trial.
Setting A single semi-rural practice in the southwest of England.
Method Adult patients with asthma were randomised to receive either their routine asthma care in the surgery or care by telephone triage. Asthma control parameters, health status and NHS resource utilisation were measured over the 12-month study period.
Results One hundred and ninety-four patients were randomised and 35% per cent more patients (n = 84 versus n = 62) received more than one consultation in the telephone group. Asthma control as measured by the asthma control questionnaire (ACQ) was similar in the clinic and telephone groups: mean change in ACQ = −0.11 (95% CI = −0.32 to 0.11) versus −0.18 (95% CI = −0.38 to 0.02). Mean NHS costs were £210 per patient per year in the telephone group compared to £334 in the clinic group (P-value of bootstrapped difference = 0.071).
Conclusion Targeted routine asthma care by telephone triage of adult asthmatics can lead to more asthma patients being reviewed, at less cost per patient and without loss of asthma control compared to usual routine care in the surgery.
INTRODUCTION
The structured regular review of people with asthma in primary care has been shown to be associated with improved clinical outcomes in terms of school or work absence, reduced exacerbation rates and improved symptom control.1,2 Furthermore, observational evidence suggest that practice nurses with a diploma in asthma management can further improve standards of care.3 Such evidence has been instrumental in formulating the 2003 British Asthma Guideline,4 which recommends that, ‘in primary care people with asthma should be reviewed regularly by a nurse with training in asthma management’. However, there is evidence that many patients do not attend or do not want to attend for routine asthma review.5,6 In one study in a semi-rural general practice most non-attenders had low asthma morbidity in terms of asthma symptoms and exacerbations, but a significant minority (25%) were symptomatic and needed treatment change.5 This suggests that not all patients with asthma necessarily need routine face-to-face asthma check-ups and that hard pressed primary care resources might be better utilised by targeting routine surgery care on those patients with higher morbidity.
Previous studies have shown that high morbidity patients with asthma can be successfully targeted using a morbidity questionnaire administered by post.7,8 However, these studies showed relatively high non-response rates to the postal questionnaires. A 3-month study of using the telephone as a method of routine asthma consultation showed this to be a technique that allowed more patients to be reviewed compared to face-to face contact without loss of acceptability or health status.9
The Royal College of Physicians (RCP) ‘three questions’10 (Box 1) is recommended by the British Asthma Guidelines for assessing asthma morbidity.4 Our study looks at the cost and effectiveness of using the RCP's questions in routine asthma telephone consultations to target routine clinic care for high morbidity patients and dealing with low-risk patients by telephone alone.
Box 1. The Royal College of Physicians Morbidity Index.10
In the last month/week:
▸ Have you had difficulty sleeping because of your asthma symptoms (including cough)?
▸ Have you had your usual asthma symptoms during the day (cough, wheeze, chest tightness or breathlessness)?
▸ Has your asthma interfered with your usual activities?
METHOD
Patients were recruited from one semi-rural practice in Wiltshire between December 2002 and March 2003. Patients were deemed eligible for the study if they were aged 17–70 years and on the practice asthma list. They were excluded from the study if they were housebound, did not possess a telephone, or were unwilling to give informed consent. Patients gave written informed consent prior to randomisation. Patients were randomised using random number tables on a one-to-one basis into one of two intervention groups and followed up for 12 months. In addition, patients were stratified into severe asthmatics (on beclometasone or equivalent >800 mcg/day) or mild/moderate asthmatics (on beclometasone or equivalent ≤800 mcg/day). It was not possible to blind the patients or nurses to the groups into which the patients were randomised.
Clinic (control) group
Patients received ‘usual’ care by 6-monthly check up (at baseline, 6 months and 12 months) via a dedicated asthma appointment with a diploma-level asthma nurse. Symptom scores, inhaler technique, and peak flow measurements were checked and all patients issued with an asthma action plan. Additional reviews were arranged according to clinical need. Patients received written invitations to attend for review, and defaulters were reminded by messages on overdue repeat prescriptions.
Telephone group
Patients were contacted by telephone at 6-monthly intervals by one of two trained asthma nurses. If no reply was obtained the patient was telephoned at another time until contact was made. The patient was then asked the RCP's ‘three questions’ plus two extra questions related to a high risk of asthma death (‘have you ever needed treatment in intensive care for your asthma?’; ‘have you been admitted to hospital with your asthma within the last year?’).11 Patients were considered ‘low risk’ if they answered ‘no’ to all the questions above. The nurse formulated an individualised asthma action plan with the patient, with advice on what to do if asthma control deteriorated. A written version of the plan was sent to the patient with an agreement that the patient would be routinely followed up in 6 months time. If patients answered ‘yes’ to any of the questions, they were deemed ‘high risk’ and a clinic asthma review actively arranged. When asthma control was deemed stable for 3 months patients were returned to telephone review.
How this fits in
Many patients with asthma do not attend for routine asthma review in the surgery. A 3-month study has shown that asthma review by telephone is acceptable and allows more patients to be reviewed. This 12-month study shows that targeted asthma review by telephone using the Royal College of Physicians Morbidity Index10 allows more patients to be reviewed, without loss of control, with improved health status, and at a saving to the NHS of 37% (£122) per patient per annum, compared to usual clinic care.
Procedure
The primary aim of the study was to investigate whether routine asthma care by telephone triage could be carried out without loss of control compared to usual clinic care, and to compare NHS costs in the two groups. The primary end point was the six-question asthma control questionnaire (ACQ),12 with secondary endpoints of health status as measured by the mini asthma quality-of-life questionnaire (mini-AQLQ)13 (both questionnaires administered by post to all patients at baseline, 6 and 12 months).
Evidence of mild exacerbations (an increase in the number of times the reliever was used above baseline of >1 on 2 consecutive days) and severe exacerbations (oral steroid use or hospitalisation) was gained from patient-held diary card data and retrospective analysis of health records.
The economic evaluation was carried out from the perspective of the NHS. We identified three main categories of resource use: costs associated with the delivery of routine asthma care, non-routine health care contacts, and asthma-related medication. The cost of routine care for patients in both groups included nurse administration time spent contacting patients to organise appointments, and clinical time of the nurse and the GP, spent assessing patients either in the surgery or over the telephone. Non-routine contacts included any extra GP or nurse consultations, out-of-hours contacts, visits to A&E, and any secondary care contacts that were respiratory-related. Medication identified as being directly related to asthma control included relief inhaled β2 agonists, inhaled steroids, oral steroids, antibiotics, leukotriene-receptor antagonists, and theophyllines.
During the trial, the asthma nurses recorded the length of time they spent on administration of patient care writing to and telephoning patients to arrange appointments. They also recorded, separately, time spent on the telephone assessing patients clinically. Non-routine healthcare contacts and prescribed medication were taken from patient records and patient diary card data.
The time of healthcare professionals was valued using Netten and Curtis14 with the asthma nurses conservatively valued as practice nurses (grade F). NHS reference costs were used to value secondary care15 and medication costs were taken from the British National Formulary (March 2004). The technique of bootstrapping16 was used to construct confidence limits around the mean of the skewed health resource use data (1000 replications were carried out).
In the context of primary care, in-patient hospital stays are few and relatively expensive. We assessed the effect of these on the results by conducting a sensitivity analysis. Neither costs nor outcomes were discounted as both were evaluated within a 12-month time frame.17
Statistical methods
Using a sample size of 115 in each group, a two-group 0.050 one-sided t-test had 90% power to reject the null hypothesis of non-equivalence in favour of the alternative hypothesis (that the means of the two groups were equivalent), assuming that the difference between the equivalence limit and the expected difference divided by the common standard deviation was 0.387 or greater. Due to a lower than expected recruitment rate and and high drop-out rate in the clinic group the number of analysable cases was 62 versus 84 in the telephone group reducing the power value to 74%.
Comparison of the mean ACQ change was made using ANOVA (using Student's t-test) with correction for baseline differences. Comparison of median mini-AQLQ values and exacerbation rates was by Mann–Whitney analysis.
RESULTS
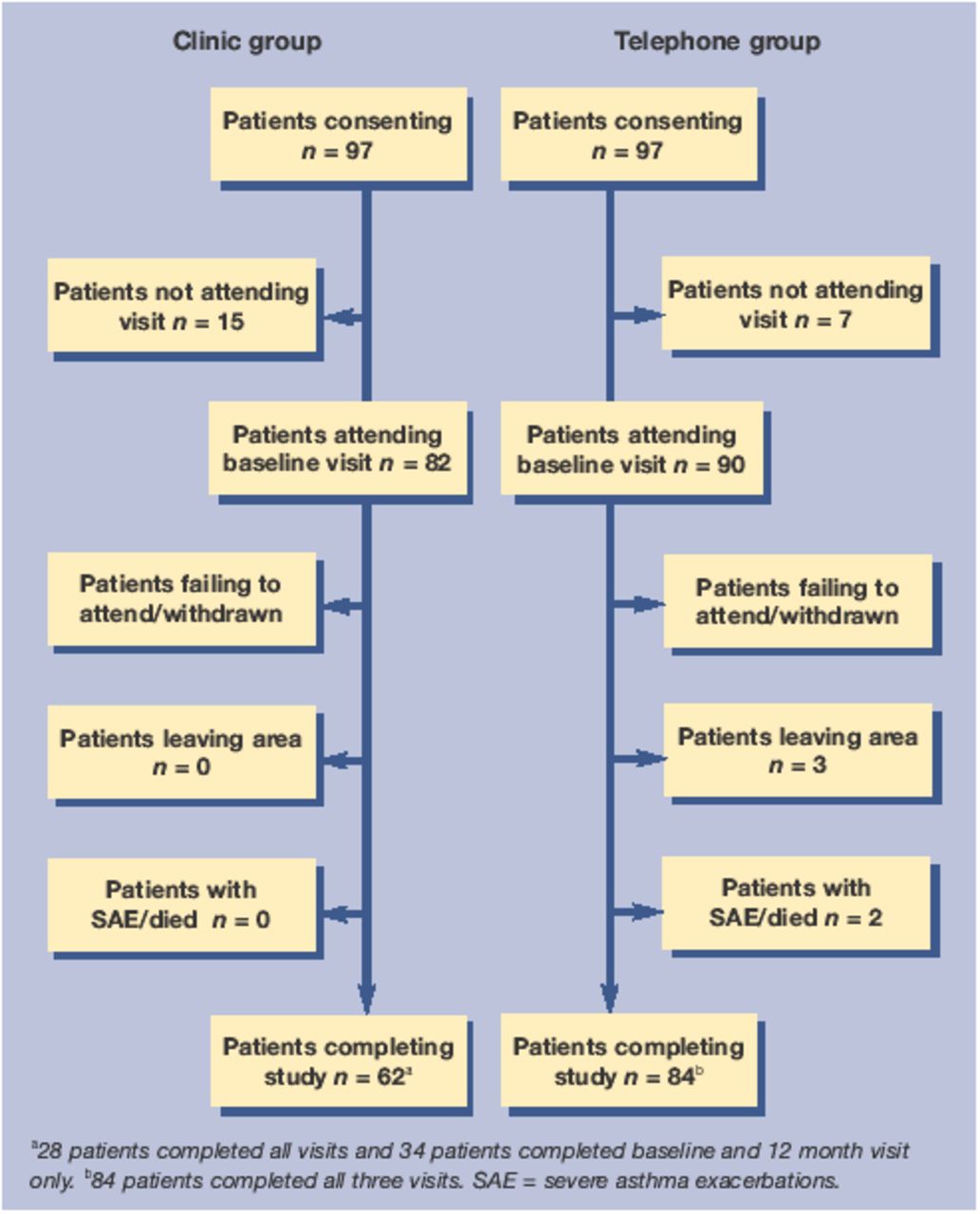
One hundred and ninety-four patients were enrolled in the study (97 in each treatment arm). Table 1 shows the baseline characteristics of the patients and Figure 1 shows the patient flow through the study. There were 20 withdrawals in the control group after the first visit (mainly due to non-compliance or non-attendance) and six in the telephone group (only one was due to non compliance or attendance). Thirty-five per cent more patients (n = 84 versus n = 62) had more than one asthma consultation over the year in the telephone group versus the clinic group.
Baseline characteristics of patient groups.
{kind=link}
Patient flow through study.
Table 2 shows the results of the primary and secondary endpoints. The mean change in ACQ was −0.11 (95% CI = −0.32 to 0.11) in the clinic group and −0.18 (95% CI = −0.38 to 0.02) in the telephone group. This was not significant. (A negative change in ACQ represents an improvement in control.) There was a trend to improvement in health status in the telephone group. The median change in mini AQLQ was +0.07 (interquartile range = 1.27) in the clinic group and +0.23 (interquartile range = 0.87) in the telephone group (P = 0.028 corrected for baseline differences). (A positive change in AQLQ represents an improvement in health status).
Summary of primary and secondary endpoint result.
Stratification of groups did not affect the results although there were too few patients in the ‘severe’ group (five in the clinic group and six in the telephone group) to make accurate statistical comparisons.
All patients in both groups said that they were ‘satisfied’ or ‘very satisfied’ with the system of asthma care that they had received over the year. Of the telephone patients, 88% expressed a strong preference for this system compared to their previous system of care.
Table 3 gives resource use and cost by randomisation group. There were savings across all three categories of resource use, with mean total cost per telephone patient estimated at £210 compared to £334 per clinic patient. Bootstrapped results gave a mean cost per head of £332.73 (95% CI = £329.54 to £335.92) for the clinic group and £210.39 (95% CI = £208.93 to £211.84) per head for the telephone patients.
Resource use and cost by randomisation group and category.
Three patients had a stay in hospital during the trial: two from the clinic group and one from the telephone group. Excluding the costs associated with these stays, the difference in mean cost per patient between the two groups was reduced to £93 (P = 0.115).
DISCUSSION
Summary of main findings
This study shows that using the RCP's ‘three questions’ to triage routine care of adult asthma patients by telephone consultation can be carried out equally effectively and at a 37% (£122) reduction in costs per patient than by usual clinic care.
There was an improvement in asthma control in both groups but the difference between groups was not significant. Similarly, mild and severe exacerbation rates were low and not statistically different in both groups, although incomplete diary records of mild exacerbations may have led to under-reporting.
There was a trend towards improvement in health status, in the telephone group, however this change is not clinically significant. A 3-month study by Pinnock et al9 showed that telephone consultations in asthma are acceptable and also do not result in a loss of health status. The present study, which used a more focused approach via the RCP's three questions and specifically looked at asthma control as a primary endpoint, suggests that the benefits of telephone consultations extend, at least, over a 12-month period.
Strengths and limitations of the study
This study was carried out in one asthma-interested semi-rural practice and could therefore be criticised as not being generalisable. However previous non-attendance rates in this practice are as high as those found elsewhere in the country.6 In addition, this study was designed to be as ‘real world’ as possible. If this had been a multicentre study it is probable that the small number of patients recruited from each practice would be those more likely to comply with the protocol. In this study we were deliberately looking to see if the telephone system could encompass patients who would previously be deemed as poor compliers or attenders. Indeed a retrospective analysis of randomised patients showed that 42 (43%) of the clinic group and 48 (49%) of the telephone group patients had not attended for routine asthma review in the previous year.
One other limitation of the study is that the assessors were not blinded to the interventions due to limited resources.
The 2003 GMS Contract18 states that patients with asthma should be reviewed at least annually. Thirty-five per cent more asthma patients received their annual review after baseline in the telephone group than in the clinic group (84 versus 62). This is consistent with a previous study where telephone consultations significantly improve access to routine asthma care.9 The patients who dropped out of the clinic group did so mainly because of non-attendance. The large number of poor compliers could raise concern about attrition bias, that is, the telephone group results seemed better than they really were because the less severe patients in the clinic group had dropped out. However, a post-hoc analysis of the patients withdrawing from the clinic group showed that they were matched by inhaled steroid dose and subsequent exacerbation rate with patients who remained in the study.
Patient satisfaction with the system was 100% in both groups. However, only patients who completed the study were asked and were more likely to be ‘satisfied compliers’. However, 88% telephone triage patients stated a strong preference for telephone review compared to the previous system of care (which was likely to be clinic appointments).
The economic evaluation was limited to the perspective of the NHS. We attempted to collect data from patients on their direct costs (travel, loss of earnings) and societal indirect costs (time off work), but these were too poorly recorded to be of use. However, the scale of savings we found across all categories of resource use suggests this limitation would not have affected the main conclusion, that telephone triage is likely to be cheaper than face-to-face review in the surgery. Most saving arose from a significant reduction in mean nurse face-to-face consultation time and nurse administration time in the telephone group. An observational study by Seale et al19 of face-to-face nurse practitioner consultations showed that a lot of time was spent on explaining treatments, discussing social issues and waiting for doctors to sign prescriptions. In this study the telephone consultation was very focused, using the RCP's three questions reducing consultation times considerably. The mean number of telephone calls to achieve success was 1.4. Patients were mainly telephoned in the early evening. We are currently looking at whether pre-booking the telephone appointments will reduce further the wasted telephone time spent contacting patients or will be counterbalanced by the increased time spent on administration.
Implications for future research
This study shows that routine telephone triage is an effective method of care for adult asthma patients. Further studies need to be carried out to determine if telephone triage is appropriate for children where factors, such as checking inhaler technique, may be more important. The use of the telephone is likely to be more limited in areas where there is a high ethnic minority and language difficulties may arise and there is a need to look at alternative ways of encouraging access to routine asthma care in this group of patients.
Acknowledgments
The authors are grateful to Maggie Roberts and Maria Kerr for help with carrying out the study and to Elizabeth Juniper for her invaluable help with the study design.
Notes
Funding
The study was funded by a research grant from Asthma UK (02/007)
Ethics committee
Bath Local Research Ethics Committee (BA267)
Competing interests
None
- Received November 17, 2004.
- Revision received February 3, 2005.
- Accepted May 20, 2005.
- © British Journal of General Practice, 2005.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

