


Abstract
Background If all GPs target their prescribing appropriately, then a positive relationship may be expected between targeting quality indicators and associated prescribing expenditure. Little is known about this relationship.
Aim To explore the relationship between prescribing quality indicators and associated prescribing expenditures.
Design Observational study of prescribing expenditure and quality indicators.
Setting Seventy-one of the 121 practices in the Norfolk and Waveney area of East Anglia in England.
Method Data were collected on quality indicators for 2002–2003 in seven areas likely to produce the greatest number of lives saved over a period of 1 year. This was linked to routine data on associated pharmaceutical expenditure.
Results There was considerable variation in quality in all areas apart from influenza immunisation. Significant correlations between prescribing quality and expenditure were found in only two of the seven areas. When quality scores were combined into a composite quality index weighted by health gain, a small positive association was found, but this association is lost if all indicators are weighted equally.
Conclusions There appeared to be no relationship between quality indicators and prescribing expenditure at the practice level for most of the therapeutic areas studied. This suggests the possibility that there may be scope for some GPs to target prescribing more appropriately towards high risk patients — and thus save more lives — without increasing prescribing expenditure.
INTRODUCTION
The average English primary care trust (PCT) spends £18 million each year on pharmaceutical prescribing, which is about 16% of its total expenditure.1 In recent years, pharmaceutical expenditure has grown faster than NHS expenditure as a whole1 and is currently rising at approximately 10.3% each year.2
For the individual GP, pharmaceutical expenditure is not limited and he or she may prescribe with freedom in this respect. PCTs must support a prescribing decision deemed necessary by the GP, even if it exceeds a target prescribing budget.3 In contrast, PCTs have a statutory duty to operate within an overall budget.4 Prescribing expenditure therefore poses a significant financial risk for PCTs.
Policy makers have recently started to focus their efforts on improving prescribing quality, as well as containing prescribing expenditure, for example with the introduction in the UK of the 2003 GP contract.5 It is not known, however, whether there is a relationship between prescribing expenditure and quality. If there were a positive relationship, then there would be a difficult trade-off issue for GPs and policy makers between efforts to improve quality and efforts to contain prescribing expenditure. If there were no relationship (or a negative one), then GPs and policy makers could sensibly focus on efforts to improve prescribing quality without worrying that this might lead to spiralling prescribing expenditure.
How this fits in
After allowing for the observable characteristics of GP practices and their patient populations, there remains substantial unexplained variation in both prescribing quality and prescribing expenditure. This is the first study to examine whether practices with higher prescribing expenditure achieve higher prescribing quality, defined in terms of appropriate targeting of high-risk patients. For five out of seven top life-saving interventions in primary care, better prescribing quality was not associated with higher prescribing expenditure. This suggests the possibility that there may be scope for some GPs to target their prescribing more appropriately — and thus to save more lives — without increasing their prescribing expenditure.
There is significant unexplained variation in prescribing expenditure between practices, after controlling for population need.6 For example, a twofold variation between English practices has been identified in expenditure on asthma medications per age, sex and temporary resident origin prescribing unit (ASTRO97-PU).7
Less is known about prescribing quality, partly because measuring quality in primary care is notoriously difficult.8 One common approach is to record the proportion of a specific high-risk patient group who receive an appropriate prescription; for example, targeting statin prescriptions for patients with high cardiovascular risk. That is the approach taken in the new GMS contract9 and in most sets of primary care quality indicators.8
Given this approach, one would expect a positive association between prescribing expenditure and targeting quality if all GPs target their prescribing (equally) ‘appropriately’ towards patients in greatest need. If there is no scope for more ‘appropriate’ targeting (that is, re-directing prescribing from ‘low risk’ to ‘high risk’ patients), then quality cannot be increased without raising the overall volume — and, therefore, cost — of prescribing.
Not all GPs may target prescribing ‘appropriately’, however. Targeting accuracy may vary because of differences in GP practice style, patient presentation behaviour and preferences, and other local factors. If some GPs target prescribing more ‘appropriately’ than others, then there may be no overall relationship between prescribing expenditure and quality at the practice level. There might conceivably even be a negative relationship, if GPs who target prescribing more ‘appropriately’ also contain costs more effectively, for instance through generic prescribing and reducing prescribing to low-risk groups. Possible differences between practices in prescribing behaviour are explored in Figure 1.

Prescribing expenditure and targeting quality associations — a stylised interpretation.
There is evidence of ‘inappropriate’ prescribing. In a study of four primary care practices in England, prescribing to patients of low cardiovascular risk was found not to be ‘appropriate’ as defined by the National Service Framework for coronary heart diesase recommendations.10 Conversely, some patients at high risk were not receiving the appropriate treatments.11
A literature search found no evidence of research investigating the relationship between prescribing expenditure and quality at the practice level, possibly because electronic records for monitoring quality in general practice are under-developed. We examined this relationship using a set of targeting quality indicators selected on the basis of evidence for their potential to save lives, compared with prescribing expenditures in the relevant therapeutic areas.
METHOD
Data collection
The study was performed with data for 2002–2003 from general practices in the Norfolk and Waveney area of East Anglia in England. Research governance and ethical approval was sought, and consent was obtained from 71 out of the 121 practices in the area.
Data on quality were obtained relating to the top seven life-saving prescribing interventions in general practice as identified by McColl et al, in a previous study.12 Table 1 lists these prescribing interventions and estimates of their potential to save lives. Each individual quality marker (QM) is defined as the proportion of the high-risk patient group receiving the specified prescribing intervention. Smoking habit recorded in the age group 15–75 years was used as a proxy for smoking cessation advice and nicotine replacement. The QM appears in the 2003 GP contract in this format and it was therefore felt more likely that practices would collect it. In addition, there is evidence that discussion of smoking habit within the consultation is itself effective in smoking cessation.13 Likewise blood pressure recorded in patients over 45 years of age was used as a proxy for screening and treatment of hypertension.
Definition of main outcome variables — the seven McColl quality indicators and their related prescribing costs per appropriate demographic prescribing unit.
These quality indicators were also combined together into composite quality scores to represent an overall total score for each practice. Two composite scores were constructed:
with weights corresponding to the effectiveness of the intervention in terms of potential lives saved; and
with equal weights for each quality indicator.
Prescribing expenditure data were obtained from PACT (Prescribing Analysis and CosT). Prescribing data directly relating to the quality intervention were collected for: angiotensin-converting enzyme (ACE) inhibitor drugs in heart failure, influenza immunisation in patients aged over 65 years, aspirin in heart disease, warfarin in atrial fibrillation and statins in heart disease. Drug costs for hypertension (including ACE inhibitors) included sections 2.4, 2.5, and 2.6.2 of the British National Formulary.14 In four cases, ASTRO97-PU was used to adjust for demand. However, in three cases (QM2–4) where the quality intervention relates exclusively to a specific age group, the corresponding prescribing costs were adjusted for that age range using practice demographic data. This is because the size of the eligible population in the specific age range is a more precise estimate of demand than the overall age, sex and temporary resident origin status of the practice population as a whole. STAR-PUs (specific therapeutic group age–sex related prescribing units) were not used, as in Norfolk there are a significant number of temporary residents that are not accounted for in STAR-PU calculations.
Prescribing expenditure in each area was also combined together into a composite prescribing expenditure figure, to represent total prescribing expenditure in all quality areas examined in this study. Since different approaches to demand adjustment were adopted in different therapeutic areas, three different expenditure variables were analysed:
sum total expenditure per patient;
sum total expenditure per ASTRO97-PU; and
the sum of average expenditure per appropriate prescribing unit, that is, adjusting either for ASTRO97-PU or for the age-specific population as appropriate to the individual therapeutic area.
Other practice characteristics and practice population variables identified as possible confounders were obtained from the relevant PCTs and the national PCT database. These included percentage of partners who were trainers, percentage of female partners, number of partners, Low Income Scheme Index (LISI) as a marker of deprivation, percentage of rural patients, percentage of dispensing patients, and consultation length.
Statistical analysis
The relationship between prescribing expenditure and quality was analysed for each of the seven McColl indicators, and also for the composite scores comparing total quality scores and their associated total prescribing expenditures. Statistical analysis was performed with SPSS for Windows (version 11) and graphs created using Stata 8.0.
Bivariate analysis was performed to examine the relationship between prescribing expenditure and quality. All variables were continuous, and data was assessed for normality by examining normality plots and performing Shapiro–Wilk W tests. If both tests were significant, Pearson's correlation was performed. If both tests were not significant, Spearman's correlation was performed. If only one Shapiro-Wilk test was significant, both correlations were performed.
It is possible that the bivariate analysis could be confounded by other factors related to both expenditure and quality, such as the training status of the practice or the deprivation status of the practice population. To address this possibility, ordinary least squares regression analysis was performed with expenditure as the dependent variable and quality and other factors — including characteristics of the practice and its patient population — as independent variables. In each case, a linear model of best fit was estimated by initially performing backward stepwise regression, checking for mis-specification problems, and then eliminating further variables according to standard model selection criteria such as adjusted R2. Quadratic functional forms were also tested where appropriate; and separate regressions were run using a logarithmic transformation of the dependent variable to adjust for its (slight) skew away from a normal distribution.
RESULTS
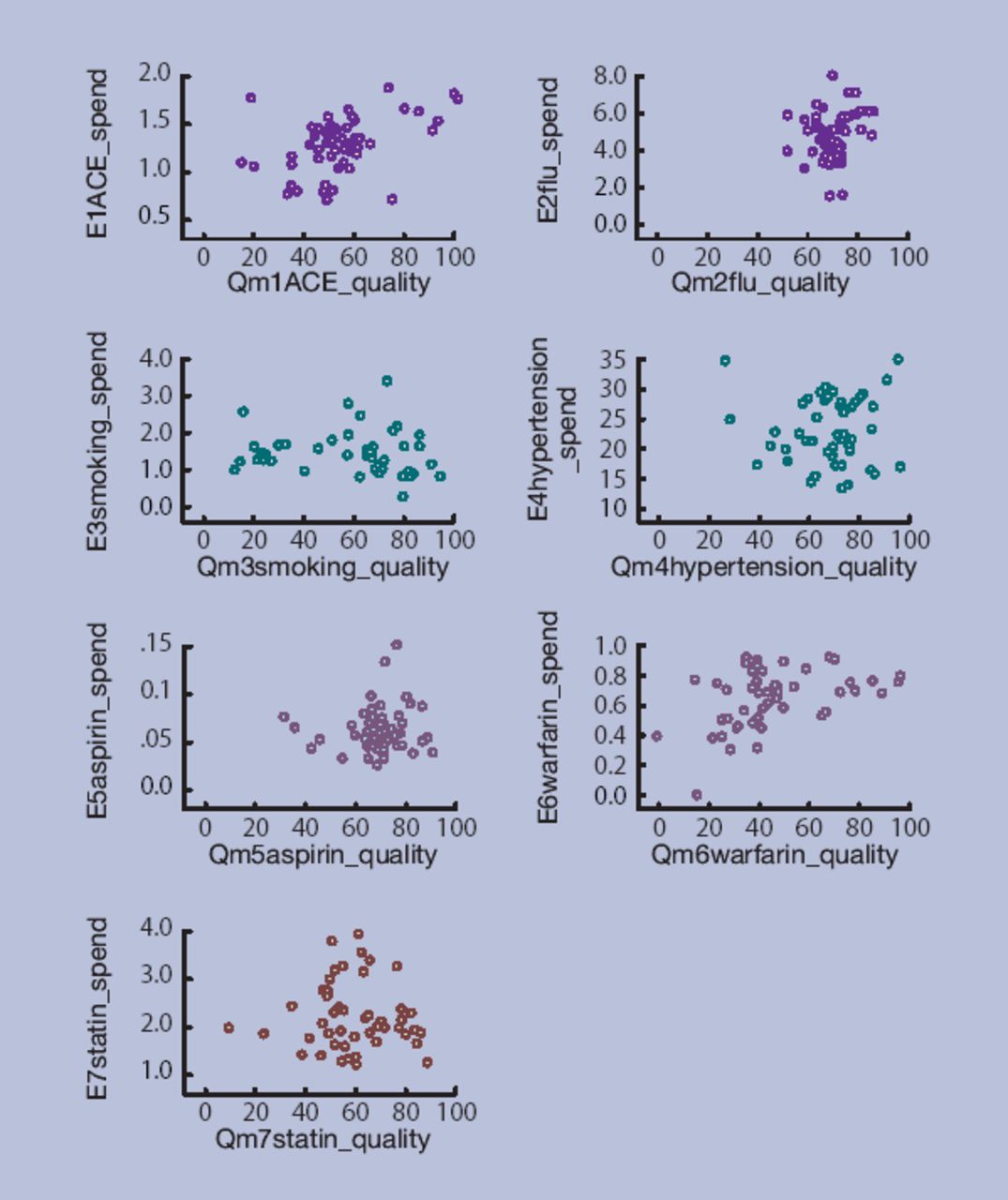
There was no association between prescribing expenditure and quality indicators in five areas: influenza immunisation; smoking cessation; hypertension; statins and aspirin in heart disease; and warfarin in atrial fibrillation. However there was a significant positive association in two areas: ACE inhibitors in heart failure; and warfarin in atrial fibrillation. Bivariate analysis for individual therapeutic areas are presented in Table 2, descriptive statistics for the expenditure and quality variables are presented in Table 3, and scatter plots for each of the seven areas in Figure 2. Regression analysis yielded the same results in terms of both the direction and significance of relationships between expenditure and quality. The only explanatory variable to reach significance at a 5% level was the deprivation status of the practice, which had a small but significant negative association with warfarin spend and aspirin spend per ASTRO97-PU (with P-values of 0.026 and 0.000, respectively).
Bivariate analysis of practice level association between quality indicators and prescribing expenditure in the relevant therapeutic area.
Descriptive statistics for the main outcome variables.

{kind=link}
{kind=link}
Scatter plots of pharmaceutical expenditure against prescribing quality indicator for all seven therapeutic areas.
Turning to the composite results, these suggest that the overall relationship between the composite quality score and prescribing expenditure is weak — and that there may be no significant relationship at all (Table 4). A significant relationship was found when composite quality score was weighted by potential lives saved. However, this gives a 43% weight to ACE inhibitors in heart failure — one of only the two areas that did exhibit a positive relationship. No significant relationship was found when each quality indicator was weighted equally, or when the composite expenditure variable was defined as total expenditure per appropriate prescribing unit, that is, for four of the six composite comparisons examined.
Bivariate analysis of practice level association between composite quality indicators and the relevant composite prescribing expenditure.
DISCUSSION
Summary of main findings and comparison with existing literature
The main finding of this study is that there was no association between pharmaceutical expenditure and quality indicators in the majority of areas studied. These results do not support any conventional view that there is a simple relationship between quality of care and overall prescribing expenditure. Furthermore, they raise the possibility that some GPs may still be treating low-risk patients before high-risk patients — a kind of ‘scattergun’ approach to prescribing. This is a concern if significant numbers of high-risk patients are receiving appropriate life-saving prescribing interventions. There is also a financial risk from poorly targeted prescribing, since pharmaceutical spending forms a significant proportion of the primary care budget and is increasing faster than inflation. In economic terms, some GP practices may be failing to maximise prescribing quality (and hence lives saved) for a given pharmaceutical spend. Therefore, it is possible that better targeting of prescribing may allow increased potential for saving lives at no extra costs to the system.
It is also interesting to note the substantial variation in quality indicator performance between practices in six of the seven therapeutic areas, as demonstrated by the standard deviations (Table 2). The one exception was influenza immunisation, with a mean of 70.4 and standard deviation of only 5.52. This was only indicator subject to incentive payments during the period under study, with a substantial bonus payment for reaching a target of 70. This study therefore confirms previous findings of a wide variation in prescribing expenditure at the practice level.6 It also supports previous research suggesting variation in quality, in that some high-risk patients are not receiving appropriate therapeutic intervention while some patients at low risk receive treatment.11
What is new, however, is the finding of no association between prescribing quality and expenditure in most areas. To our knowledge, there have been no previous studies of this association. Finally, this study highlights the need to acquire more understanding of how medicines are being used by doctors and patients before rolling out prescribing incentives and disincentives.
Strengths and limitations of the study
First, this study did not examine the non-pharmaceutical costs of prescribing — in particular, staff time input — nor possible long-term healthcare savings (or costs) arising from high quality prescribing. So it remains possible that there is a positive relationship between prescribing quality and the full economic cost of prescribing, that is, including staff time input and ‘knock-on’ costs. Secondly, this study did not examine the organisational constraints and incentives on GP prescribing behaviour. What is possible for GP practices to achieve in theory may not be possible or sensible to achieve in practice, as GP prescribing behaviour is, often quite rightly, influenced by factors other than the maximisation of lives saved. Thirdly, this study used a narrow, although important, definition of quality; that is, the potential for prescribing interventions to save lives. It would be desirable to include broader and more patient-centred measures of quality prescribing that allow comparisons between different disease areas, for example ones based on ‘quality-adjusted life years’ gained, although these are not yet routinely available. Finally, there is considerable noise in the system due to measurement and other problems, and so the lack of any observed relationship is not irrefutable evidence that no relationship between prescribing expenditure and quality indicators exists.
The study did allow for some of the factors that could produce noise, by including a range of demographic variables in the regression equations, and by using different measures of prescribing expenditure. Future research using different proxies for quality and practice variables would be useful in confirming or refuting the findings of this study.
The strengths of this study include the use of data on the quality of care not previously available, and covering a significant area of preventative practice. It examines baseline quality practice in primary care prior to the new GMS contract in 2003 and it is the first study of its kind to systematically examine the relationship of prescribing quality and cost at the practice level.
Implications for future research and clinical practice
This small-scale study provides tentative support for a policy of explicit incentives for prescribing quality, of the kind incorporated in the 2003 GP contract. Such initiatives may possibly have potential to increase prescribing quality without substantially increasing prescribing expenditure — although the cost of quality incentive payments is likely to be considerable. Future studies using more and better measures of quality would be welcome to either substantiate or refute the findings of this study. Qualitative studies of GP and patient perceptions of how medicines are being used in practices where prescribing appeared less ‘appropriate’ may also shed light on the relationship between prescribing expenditure and quality. Furthermore, future studies may be able to identify individual practices lying outside the normal range of variation in expenditure and quality with the use of detection theory.
The quality incentives in the new contract will inevitably increase the number of high-risk patients receiving preventative therapeutic interventions. What is not known is whether patients at low risk will also receive more therapeutic interventions. This could lead to a further substantial increase in primary care prescribing expenditure, and possible exposure of low risk patients to side effects of medication without clinically significant benefit.
The arrival of a broad range of robust quality indicators arising from the new GMS contract is a major opportunity to extend research into quality in primary care.15 However, this research will be challenging given the limited baseline of evidence on quality of care prior to introduction of the contract (of the kind in the present study), and the lack of information about quality of care in areas of practice not incentivised by the contract, which may potentially be neglected as a result.
Acknowledgments
We are grateful to the National Primary Care Database, and the Norfolk andWaveney PCTs, prescribing advisors and GPs for their help with data collection, with special thanks to Peter Richmond. We would also like to acknowledge the Eastern Region NHS Research Enterprise Award Scheme and Gt Yarmouth PCT for their support in providing protected time for Dr Fleetcroft; and to thank Dr Adrian Penn and Dr Alistair Lipp for their critique of the study design, and Professor Amanda Howe for her helpful comments.
Notes
Funding body
Funding was not required
Ethics Committee
East Norfolk and Waveney Research Governance Committee (2003HPP01)
Competing interests
Material from this paper was presented at the 5th World Congress of International Health Economics Association, Barcelona, July 2005, and at the 5th European Conference on Health Economics, London School of Economics, September 2004. An abstract of an earlier draft of this work was published as: ‘Fleetcroft R, Cookson R. Is there a positive relationship between the cost and quality of primary care prescribing at practice level? Appl Health Econ Health Policy 2004; 3(1): S24.’
- Received June 9, 2005.
- Revision received September 1, 2005.
- Accepted February 9, 2006.
- © British Journal of General Practice, 2006.
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

