


Abstract
Background The efficacy of bed covers that are impermeable to house dust mites has been disputed.
Aim The aim of the present study was to investigate whether the combination of ‘house dust mite impermeable’ covers and a self-management plan, based on peak flow values and symptoms, leads to reduced use of inhaled corticosteroids (ICS) than self-management alone.
Design of study Prospective, randomised, double blind, placebo-controlled trial.
Setting Primary care in a south-eastern region of the Netherlands.
Method Asthma patients aged between 16 and 60 years with a house dust mite allergy requiring ICS were randomised to intevention and placebo groups. They were trained to use a self-management plan based on peak flow and symptoms. After a 3-month training period, the intervention commenced using house dust mite impermeable and placebo bed covers. The follow-up period was 2 years. Primary outcome was the use of ICS; secondary outcomes were peak expiratory flow parameters, asthma control, and symptoms.
Results One hundred and twenty-six patients started the intervention with house dust mite impermeable or placebo bed covers. After 1 and 2 years, significant differences in allergen exposure were found between the intervention and control groups (P<0.001). No significant difference between the intervention and control groups was found in the dose of ICS (P = 0.08), morning peak flow (P = 0.52), peak flow variability (P = 0.36), dyspnoea (P = 0.46), wheezing (P = 0.77), or coughing (P = 0.41). There was no difference in asthma control between the intervention and control groups.
Conclusion House dust mite impermeable bed covers combined with self-management do not lead to reduced use of ICS compared with self-management alone.
INTRODUCTION
Inflammation is the underlying pathophysiological mechanism of asthma. It leads to variable airflow limitations resulting in asthma symptoms.1 Inhaled corticosteroids (ICS) treat the inflammation, and are therefore the most commonly used asthma treatment.2–5 Because of possible side effects, the dose of ICS should be as low as possible.6 Reduction of ICS can often be achieved in patients with mild asthma.7,8
Self-management plans are used to optimise the dose of inhaled steroids, and have shown positive effects on several asthma outcomes.8–11 Asthma health outcomes are especially improved by individualised written action plans that are based on personal best peak expiratory flow, the use of action points (recommendations for stepping up and down dose of medication based on peak flow and/or symptoms), and recommendations of both inhaled and oral corticosteroids for early treatment of exacerbations. These observations support the use of individualised written action plans.12
Self-management plans for asthma are multifaceted. They often propose allergen avoidance as one of several strategies. However, it is not known whether allergen avoidance interventions are an effective part of self-management plans. A study by Thoonen et al found that self-management reduced the use of ICS compared with usual care.8 The authors also reported significantly higher costs for domestic house dust mite allergen avoidance measures in the self-management group compared with the usual care group.13 It is not clear whether these avoidance measures contributed to the positive effects of the self-management plan.
Treatments limited to inflammation inhibitors could be seen as insufficient, because they do not address the cause of the inflammatory process. In most patients with asthma, exposure to triggers like allergens contributes to the inflammatory process. Exposure to allergens, including house dust mite allergens, can cause and maintain inflammation.14,15 Reduction of exposure to allergens can reduce inflammation, and ‘house dust mite impermeable’ bed covers are the best method to lower levels of exposure to house dust mite allergens.16–20 However, the effects of house dust mite impermeable covers on clinical parameters are unclear.21 Studies investigating the effects of house dust mite impermeable covers have yielded conflicting results.17,20,22–27
The aim of the present study was to investigate whether house dust mite allergen avoidance using bed coverings impermeable to house dust mites improves outcomes when combined with self-management plans. The efficacy of this combined strategy was assessed according to whether this leads to less use of ICS and improvement of asthma control compared with self-management alone.
METHOD
Patient selection
Asthma patients in the south-eastern region of the Netherlands were enrolled from registration networks of GPs and though open recruitment advertisements in the local press. Patients willing to participate were screened for inclusion and exclusion criteria.
Inclusion criteria were: age between 16 and 60 years, GP-based diagnosis of asthma, allergy to house dust mites, and requiring ICS. The need for ICS was defined according to guidelines of the Dutch College of General Practitioners for the treatment of asthma,28 which are comparable to the international Global Initiative for Asthma guidelines.29 Allergy was determined with a Phadiatop test, which is a test for inhalant allergy (specific immunoglobulin E [IgE] to a group of common aeroallergens). If test results are positive, radio-allergo-sorbent tests (RASTs) would be performed for specific IgEs of grasses, pollen, house dust mite, cats and dogs. IgE levels above 0.35 kU/l (class 1 or higher) were considered to be positive. Classes 1 to 3 were regarded as low allergy responses, and classes 4 to 6 were regarded as high.
How this fits in
This study shows that house dust mite impermeable covers do not seem to have an added value in self-management plans in terms of medication use, asthma control, peak flow parameters, and symptoms. However, it could be possible that the covers are beneficial in environments with higher concentrations of house dust mite allergens.
Exclusion criteria were: serious disease other than asthma with a low survival rate; other diseases that influence bronchial symptoms and/or lung function (for example, congestive heart failure or respiratory diseases other than asthma); an exacerbation 1 month before the start of the study; the use of oral steroids or inhaled cromoglycates; already using house dust mite impermeable mattress and bedding covers; and allergy to cats or dogs while still keeping these pets.
All patients agreed to participate in the study by providing written informed consent.
Study design
This study was a prospective, double blind, placebocontrolled clinical trial with a baseline period of 3 months, followed by a 2-year intervention period. Patients were randomly allocated to intervention or control groups. A randomisation list was created before the study commenced. Patients were assigned to intervention or control groups according to the number on the list, in sequence of inclusion. The intervention group used active allergen avoidance measures, applying encasings for mattresses, duvets, and pillows, consisting of nonpolyurethane moisture-permeable covers impermeable to house dust mite allergens. The placebo group received encasings for mattresses, duvets, and pillows consisting of covers permeable to house dust mite allergens. Intervention and placebo covers (supplied by Cara C'air© B.V., Velserbroek, the Netherlands) were indistinguishable from each other. Patients did not receive information on other methods of allergen avoidance.
Self-management
Patients were trained to use a self-management plan to adjust the dose of ICS to symptoms and peak expiratory flow value during a run-in period. GPs or trained research nurses gave instructions according to a standardised method. Peak expiratory flow was measured using a portable peak flow meter (Asmaplan+, Vitalograph®, Buckingham, UK). Most participants used budesonide 200 μg in a Turbuhaler®. Dose equivalents for different types of ICS and delivery devices were calculated. The dosage of metered-dose inhalers was doubled in the calculations to obtain equipotent dosages with dry powder inhalers.30 Details of the plan have been provided by Thoonen et al.8 Box 1 presents a summary of the self-management plan.
Box 1. Summary of the self-management programme
Step-up instructions
Peak flow deteriorates <80% peak expiratory flow rate (PEFR) ≥60% of personal best value (PBV) for 2 out of 3 Consecutive days:
Double budesonide dosage.
In case of insufficient response within 3 weeks: again double budesonide dosage.
Peak flow deteriorates <60% PEFR ≥40% of PBV for 2 out of 3 consecutive days:
Increase budesonide dosage to 800 μg twice daily.
In case of insufficient response within 2 days: contact GP.
Peak flow deteriorates <40% of PBV:
Immediately contact GP to start a course of oral prednisolone.
Step-down instructions
Peak flow improves to ≥40% PEFR <60% of PBV:
Continue current budesonide dosage until PEFR is >80% of PBV.
Peak flow improves to ≥60% PEFR <80% PBV:
Continue current budesonide dosage until PEFR is >80% of PBV.
Peak flow improves to ≥80% of PBV:
Halve budesonide dosage when PEFR ≥80% for a period of 6 weeks.
Details of symptoms, morning and evening peak flow, and medication use (ICS, bronchodilators, and other medication) were recorded weekly in diaries.
After a 3-month run-in period, the intervention period commenced with placebo-controlled allergen avoidance and then a 2-year follow-up period. During the run-in period, patients were trained to use the self-management plan. Over three visits they were taught how to fill in the diary, use the peak flow meter, and make adjustments to their medication. After the training period, they started the allergen avoidance measures. During the intervention period, patients were visited at home every 6 months to check the implementation of the self-management plan.
Dust collection and ‘Der p 1’ assessment
Dust samples were taken from mattresses at the start of the intervention period (before the covers were put on), after 1 year, and after 2 years of intervention. Compliance with the use of the encasings was checked at the time of sampling. All dust samples were collected with a vacuum cleaner (Bosch Activa 60, type BS6, 1300 Watt). The upper surface of the entire bare mattress (or the upper surface of the mattress covers after encasing) was sampled in a standardised way at an intensity of 2 minutes per m2. Dust samples were stored in the freezer until they were analysed. The amount of dust was weighed and a 10% (w/v) extraction in 0.01 mol/l NH4HCO3 was performed by overnight rotation at 4°C. Samples were centrifuged and supernatants were used for detection of Dermatophagoides pteronyssinus (Der p) allergen 1 by enzyme-linked immunosorbant assay (ELISA).
Asthma control
Asthma control was assessed using the asthma control questionnaire©.31 Seven items were scored on a seven-point scale from 0 to 6. Five items were about symptoms during the past week, one was about use of short-acting β-agonists, and one was about airway calibre. All items were equally weighted. The overall score was the mean of the seven responses, ranging from 0 (well-controlled asthma) to 6 (extremely poorly controlled asthma).
Statistical analysis
The primary effect parameter was the difference between the two groups in the ICS dosages over the 2-year period. With an assumed difference of 250 μg between the intervention and control groups and a standard deviation of 485 μg, to achieve a power of 80% with α = 0.05, 120 patients were needed. Assuming a drop-out rate of 20%, the study needed to recruit 150 patients. Differences in patient characteristics between the two selection methods (GPs or open) or instruction groups (GPs or nurses) were tested with Student's t-test or χ2 test depending on the type of variable. As the distributions of the Der p 1 concentrations (in μg/g and in μg/m2) and amounts of dust (g) were positively skewed (and could not be normalised by log transformation), medians were presented as summary data. Researchers tested the differences between active and placebo groups for Der p 1 concentrations (μg/g and μg/m2) and amounts of dust (g), using the nonparametric Mann–Whitney U test.
Quarterly means per patient were calculated from diary data of the following variables: daily dose of ICS, morning peak flow, peak flow variability, dyspnoea, wheezing, and coughing. In view of the lack of normal distribution, nonparametric analyses were used to evaluate patients' mean responses over time. The ‘last observation carried forward’ method was used to replace missing values. Mann–Whitney U tests were used for between-group comparisons for the entire intervention period as well as for each 3-month period. Nonparametric 95% confidence intervals (CIs) were calculated for differences between groups.
Post-hoc analyses were performed for subgroups based on different smoking status, mono versus multiple allergies, house dust mite allergy low (RAST category 1 to 3) versus high (RAST category 4 to 6) and different categories of Der p1 concentration at baseline, measured in ng/g of dust (<2000 ng/g, 2000–10,000 ng/g, ≥10 000 ng/g).
All analyses were based on the intention-to-treat principle. Statistical significance was defined as P<0.05 for the primary outcome and P<0.01 for secondary outcomes. SPSS for Windows (version 12.0; SPSS, Inc. Chicago) and R32 (version 2.1.1) were used for nonparametric confidence intervals.
RESULTS
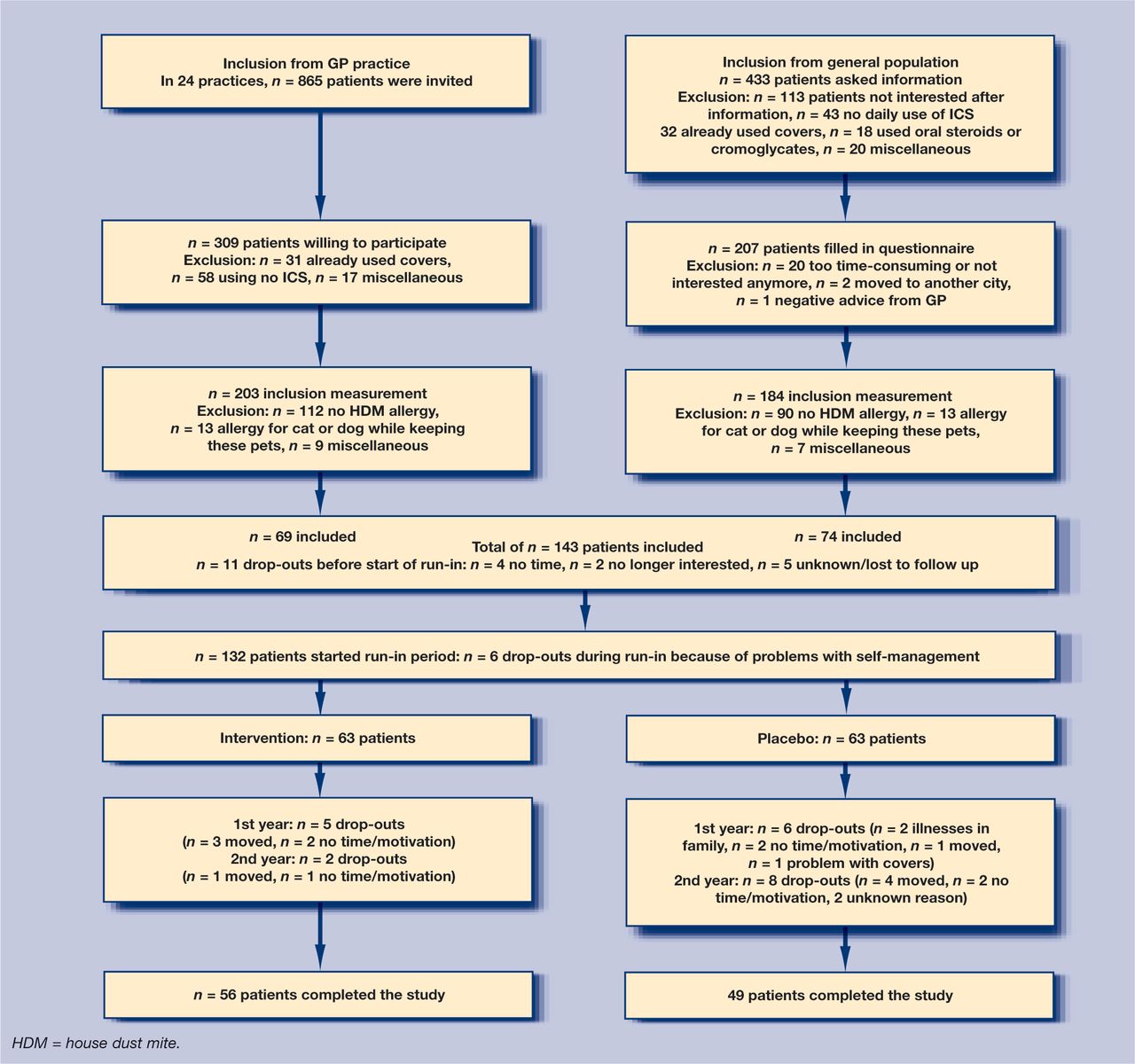
Patients were selected from general practices or open recruitment. Figure 1 displays the patient flow for the selection, inclusion, and study stages. Patients were recruited between September 1999 and December 2001. The last patient was studied in July 2004.
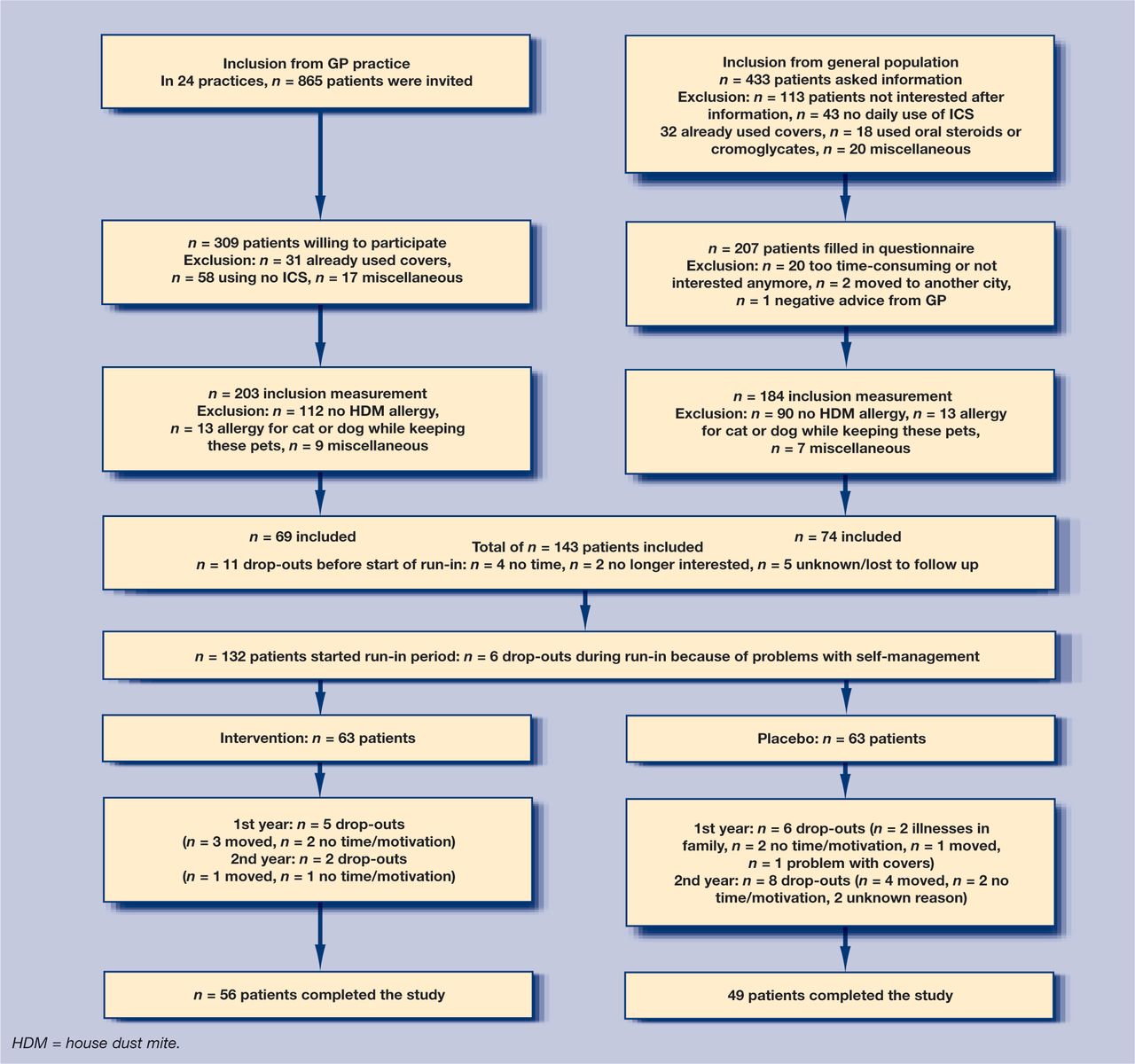
Patient flow for selection, inclusion and study stages.
One hundred and forty-three patients were included. Eleven patients dropped out before the start of the study, and six patients dropped out during the run-in period. Hence, 126 patients started the intervention with house dust mite impermeable or placebo covers. Table 1 shows the characteristics of patients who started the intervention.
Baseline characteristics for intervention and placebo groups.
There was no significant difference in any of the variables between the intervention and control groups. Patient characteristics were also compared between the GP-selected group and the open recruitment group, and between instruction by GPs and by nurses. The only significant differences found related to age (recruitment by GPs versus open: 37.7 versus 45.3 years; instruction by GPs versus nurses: 36.6 versus 43.6 years). As these were not a clinically relevant differences, analyses were pooled for the different selection and instruction groups.
Allergen avoidance measures were carried out after a run-in period of 3 months, in which patients learned about and became familiar with the use of the self-management plan. Results of the dust samples were expressed as the total amount of dust in grams, Der p1 concentrations in ng/g, and Der p 1 densities in nanogram per square metre of mattress (ng/m2).
At the start of the intervention, there was little difference between the intervention and placebo groups in the amount of dust (0.53 versus 0.54 g), Der p 1 concentrations (863 versus 806 ng/g), or Der p 1 densities (52 versus 61 ng/m2). After 1 and 2 years, significant differences between the intervention and placebo groups were found in Der p1 concentrations (377 versus 1070 ng/g, P<0.001; and 115 versus 895 ng/g, P<0.001 respectively), and Der p1 densities (9 versus 82 ng/m2, P<0.001; and 10 versus 115 ng/m2, P<0.001).
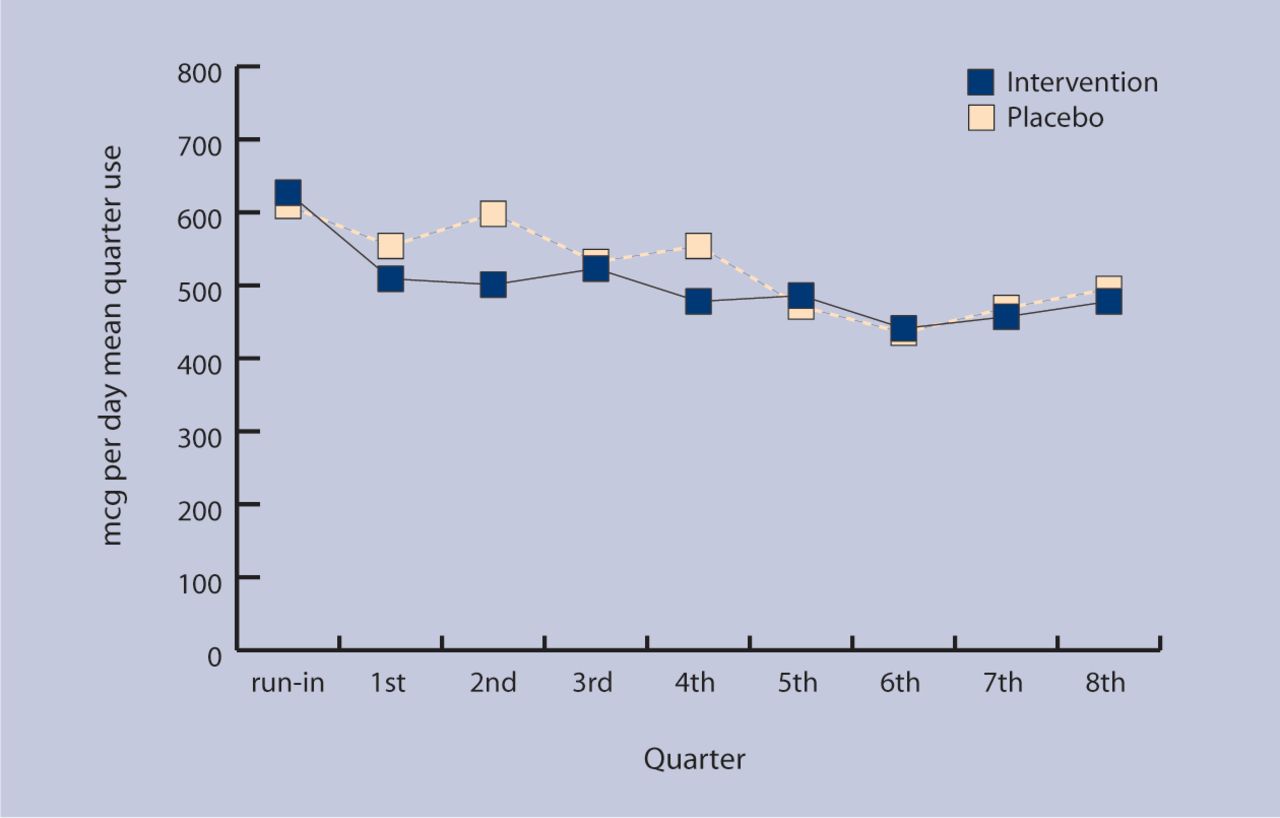
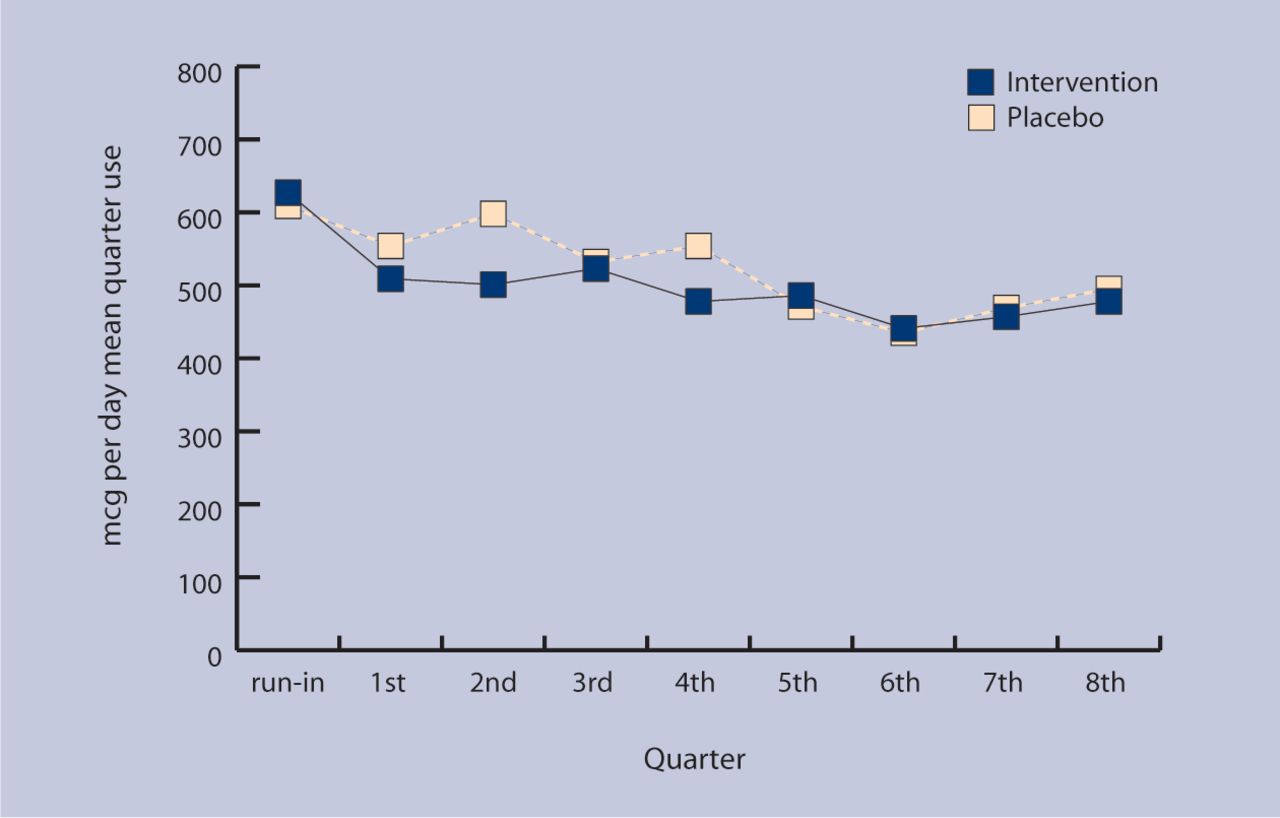
No significant difference in ICS dose was found between the intervention and control groups during the 2-year follow-up. Estimated difference in ICS use over the whole period between intervention and control groups was −830.8 μg, with a 95% CI of −1646.2 to 92.3 μg. Figure 2 shows mean inhaled corticosteroid use in the intervention and control groups during the two-year follow-up. Differences were tested with a Mann–Whitney U test; P = 0.08.
{kind=link}
{kind=link}
Inhaled corticosteroids use during the study.
No significant difference was found between the intervention and control groups in the secondary parameters morning peak flow (P = 0.52), peak flow variability (P = 0.36), dyspnoea (P = 0.46), wheezing (P = 0.77), or coughing (P = 0.41) during follow-up.
Subgroup analyses did not yield any significant difference for smoking status (current, ex-smoker, or never smoking), mono versus multiple allergies, house dust mite allergy low (RAST class 1–3) versus high (RAST class 4–6), or Der p 1 concentration at run-in (<2000 ng/g, 2000–10,000 ng/g, or ≥10 000 ng/g).
At run-in, asthma control was good in both the intervention and control groups (mean asthma control score 1.13 versus 1.05, on a scale from 0 to 6). Mean asthma control scores for the intervention group after 1 and 2 years were 1.23 and 1.03, while the control group had scores of 1.13 and 1.71. Although a difference in asthma control score of more than 0.5 can be regarded as clinically significant,33 these differences were not statistically significant (P = 0.27).
DISCUSSION
Summary of main findings
The present study did not find a clear difference in ICS doses between the intervention and control groups during 2 years of follow-up. No significant difference was found in asthma control, morning peak flow, peak flow variability, or symptoms. Asthma was well controlled at baseline and continued to be well controlled during the study in intervention and control groups. The high level of asthma control in this study could be partially explained by low allergen concentrations.
Strengths and limitations of the study
Rigorous selection criteria were used. All patients had to be sensitised to house dust mite allergens. Patients with allergies to cats or dogs who were nevertheless keeping these pets were excluded, as were patients already using impermeable bed covers. This selection resulted in a population that might benefit most from house dust mite allergen avoidance, without dilution of the effect due to exposure to other relevant allergens. Therefore, it is likely that the effect of house dust mite allergen avoidance in real life will be smaller than the effect found in this trial. Symptom scores were already very low during the run-in period, not leaving much room for improvement.
House dust mite allergen concentrations were also very low. At baseline, the majority of patients (66%) were exposed to Der p 1 concentrations <2000 ng/g of dust.
It could be expected that patients with a high baseline exposure to house dust mite allergens would benefit more from allergen avoidance than patients who already had a low exposure to these allergens. The number of patients with a baseline exposure ≥10 000 ng/g dust was very small (9%). The subgroup analysis of patients with a baseline exposure ≥10 000 ng/g did not yield a significant difference in ICS use between the intervention and control groups during the follow-up period. The low baseline allergen concentrations in the current study resulted in a small contrast between the intervention and control groups, leaving no room for clinically important improvement.
The majority of the patients (74.5%) had already made adjustments to their houses, such as hard-surface floors and limited use of upholstered furniture, adjustments which lower Der p1 concentrations. This large percentage could be due to well-organised asthma care. The Dutch College of General Practitioners' guidelines for the treatment of asthma recommend sanitation measures in patients' homes.28
It seems unlikely that the results of the present study can be explained by a lack of power, although there was a relatively high dropout rate. A post-hoc power calculation showed that with 50 patients in each group completing the study, a difference of 270 μg could be demonstrated, which the current authors think is reasonable.
Comparison with existing literature
Studies of the effects of house dust mite avoidance measures have shown conflicting results. Several studies, including a Cochrane review, failed to show beneficial effects of house dust mite avoidance measures.21–23,34 However, other studies have reported positive effects on several outcomes.17,20,24–27 One study among children found a reduction in the need for ICS after encasings were applied to mattresses and pillows.24 Nevertheless, none of the abovem-entioned studies featured avoidance measures in the context of a self-management plan.
Other studies in the Netherlands have also found low allergen concentrations.26,27 A study in a country with a climate comparable to that in the Netherlands found a 50% exposure to house dust mite allergen concentrations <2000 ng/g dust at baseline.22
It has been demonstrated that mattress encasings have a significant but modest effect on house dust mite allergen levels for mattresses that already have low mite allergen levels.35
A Der p1 concentration of 2000 ng/g dust is considered to be the threshold level for sensitisation to house dust mite allergen, whereas concentrations ≥10 000 ng/g dust can cause acute asthmatic symptoms in sensitised individuals.36
It has been demonstrated that the concentrations of house dust mite allergens are lower in homes of atopic patients than in those of non-atopic patients.37
The self-management plan used in this study had previously been shown to lower ICS dosages.8 The previous study also found that the costs of domestic house dust mite allergen avoidance measures were significantly higher in the self-management group than in the usual care group.13 Positive effects of self-management on asthma control and other outcomes have been previously identified.9,11,38
Implications for future research
On the basis of this study, it cannot be concluded that house dust mite impermeable covers have an added value in a self-management plan for medication use, asthma control, peak flow parameters, or symptoms. However, the use of house dust mite impermeable covers in other countries, with a warmer, more humid climate and higher levels of house dust mite allergens, could allow patients to reduce, and possibly limit, the use of ICS. Further research is required in this area.
Acknowledgments
We would like to acknowledge all participants of this trial and Cara C'air for the supply of intervention and placebo covers.
Notes
Funding body
This study was supported by a grant from the Netherlands Organisation for Scientific Research (grant no. 904-58-091), the Netherlands Asthma Foundation (project no.98.55), AstraZeneca B.V. and Boehringer Ingelheim
Ethics committee
The Medical Ethical Committee of the Academic Hospital Maastricht, the Netherlands approved the study
Competing interests
The authors have stated that there are none
- Received April 7, 2006.
- Revision received May 31, 2006.
- Accepted October 18, 2006.
- © British Journal of General Practice, 2007.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

