


Abstract
Background GPs vary greatly in their clinical management of hypertension, for reasons that are poorly understood.
Aim To explore GPs' awareness of current hypertension guidelines and their self-reported implementation of them in clinical practice.
Design of study Questionnaire survey via the internet.
Setting Primary care.
Method Survey of GPs (n = 401), based on the ‘awareness-to-adherence’ model of behavioural change.
Results While awareness of recommendations was high, agreement and adoption were often less so. Almost all practitioners (99%) were aware of the guidance on statin therapy but fewer than half (43%; 95% confidence interval [CI] 38–48%) adhered to the recommendation in practice. Three-quarters (77%) were aware that blood pressure should initially be measured in both arms, but only 30% agreed with the recommendation (95% CI = 26 to 34%), and 13% (95% CI = 10 to 16%) adhered to it. Although the adoption of a recommendation was usually consequent on agreement with it, 19% of GPs (95% CI = 15 to 23%) reported adherence to financially-incentivised guidance on statin therapy without either being aware of it or in agreement with it. No significant association was found among age, sex, year of graduation, or post held and level of awareness, agreement, or adoption.
Conclusion The specific barrier and action needed to promote application of hypertension guidelines varies with each clinical action. Lack of awareness is seldom the problem. Most GPs are unlikely to implement elements of guidance they disagree with even if given financial incentives. High adherence requires a reflective workforce that can respond to the scientific evidence underpinning the guidance.
INTRODUCTION
Hypertension affects about 20% of adults worldwide and is ranked third as a cause of disability-adjusted life years.1 By 2025 it is projected that 29% of the world's population (over 1.56 billion adults) will have hypertension.
Provided that patients are identified and treated appropriately, much of the morbidity and mortality associated with hypertension is avoidable. However, many patients remain undetected or untreated, and only 14% of patients on treatment achieve the recommended blood pressure target despite an extensive evidence base.2 Many factors, both patient- and physician-related, contribute to the low level of blood pressure control. Major determinants include implementation of inappropriate treatment regimens that do not achieve target blood pressure, and poor patient adherence.3
Guidelines aim to assist clinicians in the management of patients with hypertension, and are developed to improve the suboptimal treatment of raised blood pressure.3–5 Although the majority of physicians support the concept of guidelines, several surveys suggest that recommendations vary in their degree of uptake.6 Non-implementation of guidelines may be due to several factors: lack of awareness, lack of agreement, lack of belief that one can actually perform a behaviour, lack of expectation that a given behaviour will lead to a particular consequence, the inertia of previous practice, and external barriers.7 However, little is known about the process and steps of physicians changing their practice after they become aware of a guideline.7 Thus a better understanding of clinicians' concerns, needs, and difficulties in the application of research and guidelines is vital in improving guideline format and uptake.
The standard model of how medical knowledge influences physicians' behaviour is based on the assumption that information that is synthesised and disseminated by respected national authorities consistently leads to changes in physicians' clinical behaviour. This model — the passive dissemination model — upon which the success of the guidelines movement initially was anticipated, is now recognised to be too simplistic and rarely accurate.8 The passive dissemination model fails to account for the legitimate concerns, information needs, and logistical problems that frontline clinicians need to consider as they apply research and recommendations in routine care.
An alternative staged model developed by Pathman et al,8 the awareness-to-adherence model, postulates a sequence of cognitive and behavioural steps that physicians make as they change behaviour:7,8 physicians, who are initially unaware of a specific piece of research or guideline recommendation must first become aware of it (awareness), then agree with it in principle (agreement), then decide it is appropriate and feasible to use in their own practice (adoption), and finally succeed in following it at appropriate times (adhere to it).
The current study aimed to survey UK GPs to understand better their reasons for not implementing specific guidance within the National Institute for Health and Clinical Excellence (NICE) and British Hypertension Society hypertension guidelines.4,5 This study also aimed to assess whether the behaviour of GPs is consistent with an awareness-to-adherence model of steps to clinical guideline uptake.
METHOD
A questionnaire was sent to 800 GPs in the UK on 10–14 May 2006. The questionnaire was presented as a link in a targeted electronic clinical bulletin distributed through doctors.net.uk. The questionnaire was adapted from the original four steps of the awareness-to-adherence questionnaire by Pathman et al.7,8 This questionnaire assesses the awareness, agreement, and adoption of the recommended practice. In addition, adherence was also assessed by asking GPs about their use of a systematic approach to implement a given strategy consistently.
Questions were based on seven recommendations from British Hypertension Society guidelines,9 and the NICE guidelines5 (Box 1). The questionnaire was piloted on a sample of GPs from the Department of Primary Health Care, University of Oxford to test for clarity and ease of completion. Based on these returns, minor changes were made to the original format of the Pathman et al questionnaire to improve clarity. Pilot data were not incorporated in the sample results.
How this fits in
GPs vary in their awareness of, agreement with, and adoption in practice of hypertension guidelines. Guideline developers should take into account stakeholders' agreement levels when developing specific guideline recommendations. If uptake of a recommendation is low, an analysis of the concerns and barriers is appropriate.
Box 1. Order of guideline recommendations assessed in the questionnaire survey.5,9
▸ Blood pressure based on home/self-monitoring treatment should be adjusted downwards by 10/5 mmHg.
▸ Blood pressure should be measured in both arms when making the initial diagnosis of hypertension.
▸ Verbal advice on lifestyle measures should be provided for all newly diagnosed patients with hypertension.
▸ Written advice on lifestyle measures should be provided to all newly diagnosed patients with hypertension.
▸ Patients with mild hypertension should be reviewed annually even if they are not receiving treatment.
▸ Statin therapy should be used for primary prevention in people with high blood pressure who have a 10-year cardiovascular disease risk ≥20%.
▸ In unselective hypertensive populations, no one class of agents is any more effective at lowering blood pressure than another.
Questionnaire responses were categorised in relation to each stage of the awareness-to-adherence model. Responders were classified as unaware of a recommendation if they had heard or read ‘nothing at all’ about the recommendation. Agreement was classified according to whether they agreed or did not agree with the guideline. They were considered to have adopted a guideline when they reported implementing it ‘more than half of the time’. They were considered to adhere to a guideline when they ‘always’ or ‘more than half the time’ applied it in clinical practice and specified in their free-text response the system they had in place to promote or monitor application. As this free-text information was not sought in relation to verbal advice and adjustment for home monitoring, adherence is not reported for these variables. Similarly, adoption and adherence categorisation could not be applied to the recommendation ‘no one class of agent being more effective’.
Data were analysed using SPSS (version 14.0). Fisher's Exact test was used to test for associations between individual characteristics and clinical behaviour; exact 95% confidence intervals (95% CI) are reported when appropriate to indicate the precision of estimates of proportion. Results reported in Figure 1 were analysed sequentially so that individuals giving responses inconsistent with the model of Pathman et al (for example, reporting disagreement with the guideline without reporting awareness) were excluded.8 Data on these individuals are reported separately in the text and are shown in Figure 2.
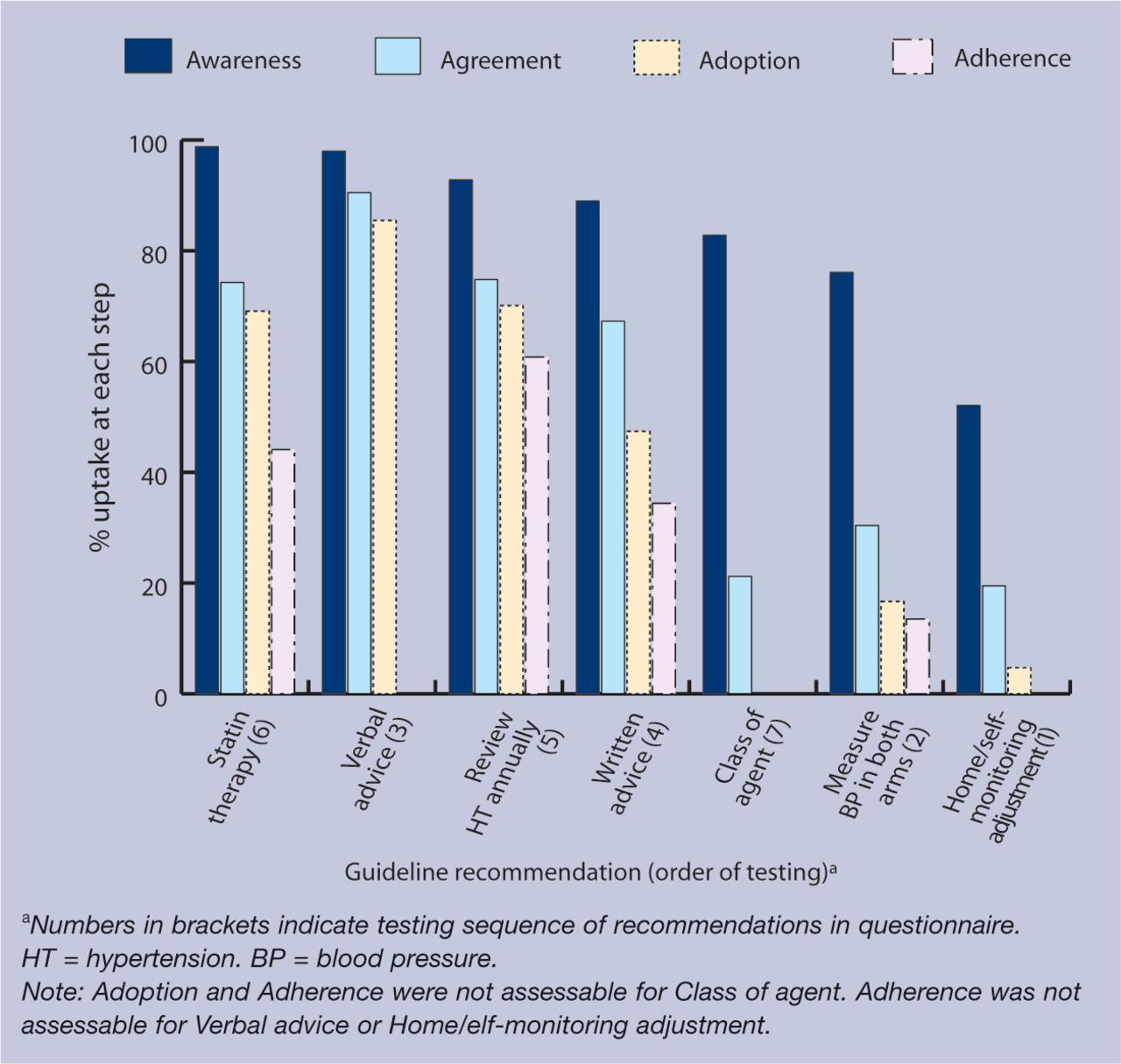
Sequential analysis of proportion of GPs reporting awareness of, agreement with, adoption of, and adherence to each hypertension guideline.
{kind=link}
{kind=link}
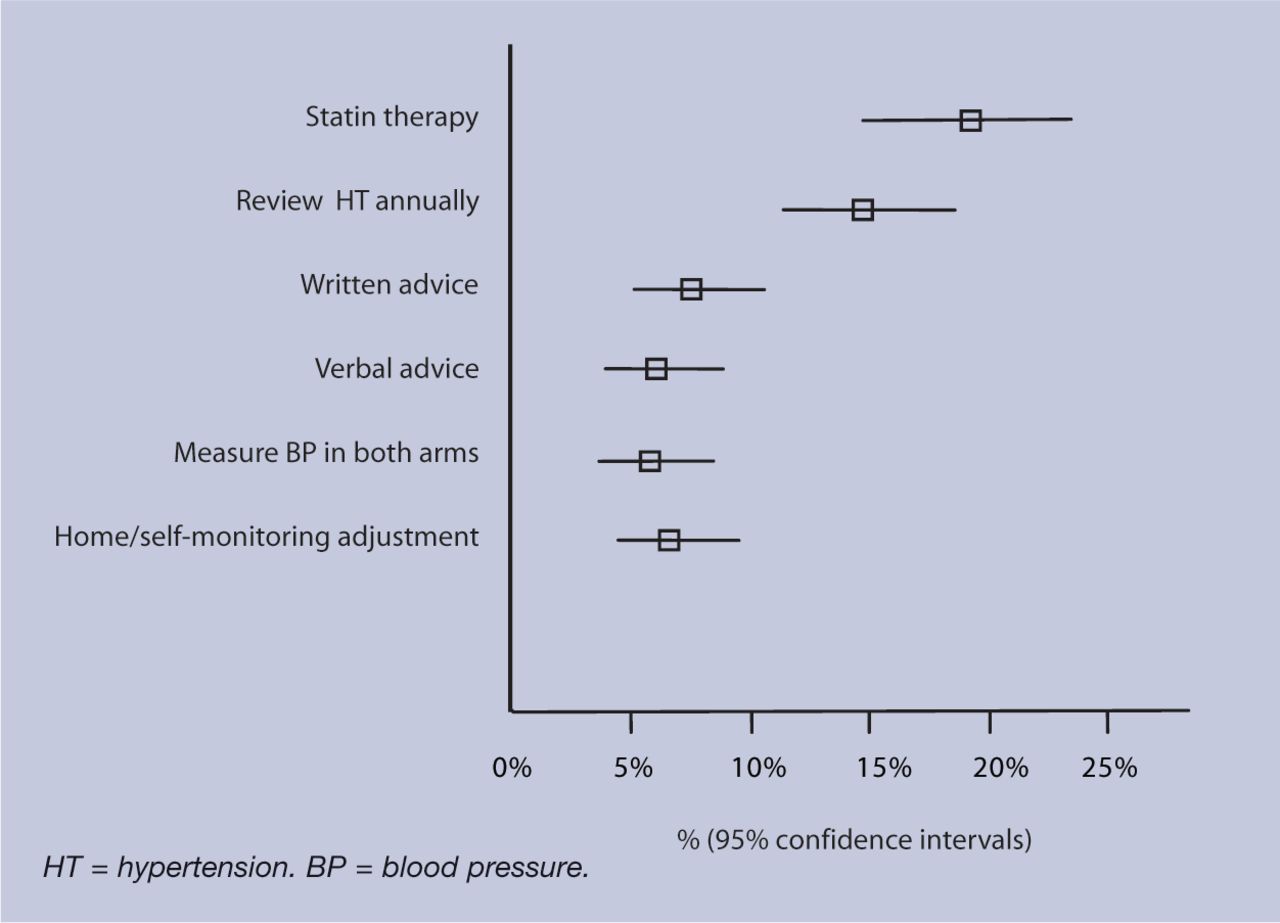
Percentage of GPs who report adopting each recommendation without reporting being aware or agreeing with it (error bars show 95% confidence intervals).
RESULTS
Of the 800 GPs sent the electronic questionnaire, 401 replied (50.1% response rate). Responders were similar to the English GP population in terms of sex (40% female in the survey versus 42% in the GP population) and employment status (10% versus 7% registrars), but differed in terms of GP partner principal status (57% in the sample versus 83% of the English GP population; Table 1).10
Characteristics of GP responders (n = 401).
Figure 1 illustrates the progression from awareness to adherence for those GPs for the seven guideline recommendations shown in Box 1. Awareness ranged from 99% (95% CI = 98 to 100%) for the need to prescribe statin therapy for patients with hypertension at high risk of cardiovascular disease to 52% (95% CI = 47 to 57%) for the need for blood pressures based on home/self-monitoring to be adjusted before comparison with clinic measurements.
The gap between awareness of guidelines and adherence to them was wide for all guidelines except the recommendation to provide verbal advice on lifestyle change: 97% were aware, 90% agreed, and 85% said they adopted this advice. In contrast, while almost all practitioners were aware of the guidance on statin therapy, fewer than half (43%, 95% CI = 38 to 48%) adhered to it. Similarly, three-quarters (77%) were aware that blood pressure should be measured in both arms, but only 30% agreed with it (95% CI = 26 to 34%) and 13% (95% CI = 10 to 16%) adhered to it. The biggest gap between awareness and agreement (62%) was for the guideline on the choice of class of antihypertensive agent. The guideline achieving least adherence was the recommendation on home/self-monitoring: despite 51% of GPs being aware of the guideline, only 5% (95% CI = 3 to 7%) reported their method of adopting it.
In reporting their agreement with a guideline, expression of uncertainty was uncommon (maximum 17%) but disagreement was common. Over half (54%, 95% CI = 49 to 59%) disagreed with the recommendation that blood pressure should be measured in both arms when making the initial diagnosis. Between 21% and 25% disagreed with the guideline on providing written advice along with the prescription of statins to all patients with hypertension at high risk of cardiovascular disease, and with the guidance that no single class of agent is any more effective at lowering blood pressure than another. No significant association was found among age, sex, year of graduation, or post held and level of awareness, agreement, or adherence.
For five of the seven guideline recommendations, the model of Pathman et al (that is, progression from awareness to agreement, adoption, and adherence) fitted the data well: only 6–8% of responders gave inconsistent responses. However, for the two guidelines for which there is a specific financial incentive, this proportion was higher (Figure 2). Specifically, 19% (95% CI = 15 to 23%) of GPs have adopted statin therapy for primary prevention, and 15% (95% CI = 11 to 19%) have adopted annual review of hypertension for those diagnosed with hypertension but not on therapy without expressing awareness of, or agreement with, the underlying guideline recommendation.
The one-third (34%) of GPs who adhered to the recommendation to provide written advice reported the source of the written information they used. Three sources provided more than three-quarters of the information distributed: the patient information leaflet service (47%; www.patient.co.uk/pils.asp), GPs' own advice leaflets (14%), and information from the British Heart Foundation (13%; www.bhf.org.uk/).
DISCUSSION
Summary of main findings
This study suggests that GPs may not adopt recommendations despite high awareness. There are likely to be several reasons for this finding. First, GPs may disagree with the recommendation if it is thought to be based on opinion, poor evidence, good evidence in inappropriate populations, or does not take into account the issues of patient values and preferences.11 Second, few recommendations are universally applicable, and they need to be accompanied by sufficient information on benefits and harms to allow clinicians and patients to make informed decisions. Precise targets and thresholds are likely to be arbitrary, and are often based more on re-interpretation of existing evidence and less on new knowledge.12 Third, recommendations may be impractical in many clinical settings because of limitations in consulting time, lack of local resources, or lack of attention to the logistics of implementation. Finally, the volume of recommendations and guidelines means that most GPs do not have time to read and memorise the full details of all guidance.12
Comparison with existing literature
The reduction observed with each subsequent stage of GPs' responses to hypertension guidelines provides support for the awareness-to-adherence model originally described by Pathman et al.8 Two previous surveys have used the awareness-to-adherence model. The 1996 survey by Pathman et al on vaccine recommendations showed that data for 91% of physicians fitted the model at every step.8 An assessment of physicians' treatment of stable angina pectoris showed that, despite high levels of both awareness and agreement, there was significant variation in guideline adoption in practice, suggesting practical obstacles to uptake.13
The awareness-to-adherence model may help to identify clinicians' concerns (legitimate or not), obstacles, and problems with specific recommendations. For example, the major gap with blood pressure measurement in both arms appears to be clinicians' agreement of the need to do this. However, most guidelines simply state this should be done, but do not point out that around 5% of patients will have at least a 10mmHg inter-arm difference in systolic blood pressure, and that such difference may be indicative of greater risk.14 Furthermore, no guidance gives specific advice on how to determine inter-arm difference accurately and feasibly. Such justification and practical advice would seem helpful for practitioners to agree to and adopt the additional measurements required.
Practical problems may also explain the greater extent to which GPs provided verbal lifestyle advice than written information. This appeared to be partly a lack of agreement that the additional work was worthwhile, and partly the ease of routinely providing such information in the consultation room. However, there is good evidence that written information is important for patient adherence.15–17
For two of the six specific recommendations (annual review of patients with hypertension not on therapy, and statin therapy for primary prevention of cardiovascular disease), a proportion of individual GPs appeared to adopt the strategy without agreeing with it. One explanation for this anomaly is that for both of these specific recommendations there is a direct financial incentive for implementation through the Quality and Outcomes Framework in UK general practice. This suggests that for a few GPs (up to 20%) a financial incentive from a respected organisation may obviate full agreement with the evidence underlying the recommendation. However, there cannot be a direct financial incentive for every important clinical intervention. Furthermore, most GPs appear unlikely to implement elements of guidance they disagree with, even if given financial incentives, suggesting that a more discerning strategy might be appropriate.
Strengths and limitations of the study
Limitations of this study include the sample frame and response rate of the internet survey, and the use of self-reporting. While the results may not generalise precisely to all GPs, the findings support the awareness-to-adherence model for at least a subset. Electronic surveys are rapid and allow tighter control of the order of questions, preventing responders from returning to change their answers or missing out responses.18 However, obtaining a representative sample of all GPs with an adequate response rate is problematic: a systematic review of internet surveys of health professionals suggested a national list of NHS.net email addresses as a solution.18 Currently, doctors.net.uk is the best feasible proxy: with a membership of 144 369 doctors it is the largest, active medical network in the UK. The response rate in the present study is comparable with previous internet surveys,18 and the characteristics of the GPs sampled broadly represent those of all English GPs.
Implications for future research and clinical practice
Potential problems and barriers to physicians' use of guideline recommendations have been identified previously, with the majority of surveys examining only one type of barrier.7 The model of awareness-to-adherence may help to identify GPs' specific concerns with recommended practice changes regarding their evidence, applicability, or practicalities of implementation.19 If uptake of a specific recommendation is low, a more subtle analysis of the concerns and barriers is likely to be appropriate; this might include pilot questioning of GPs to identify likely cognitive and practical difficulties requiring adaptation of a given recommendation. High research uptake requires a reflective workforce that can respond to the scientific evidence and practical clinical issues underpinning practice changes.
Acknowledgments
We thank Donald Pathman for providing a copy of his original questionnaire. We also thank Mike Moher, Anthony Harnden, Peter Rose, and Matthew Thompson for their help in the development of this questionnaire. We thank Neil Bacon and Tim Ringrose of doctors.net.uk for the preparation and dissemination of the survey
Notes
Funding body
This project was funded by the Office of Health Economics. Dr Carl Heneghan is funded by a Department of Health NCCRD award
Ethics committee
Not applicable
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received July 19, 2007.
- Revision received August 17, 2007.
- Accepted September 7, 2007.
- © British Journal of General Practice, 2007.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

