


Abstract
Background In England, the Expert Patients Programme, a lay-led chronic disease self-management course, was developed to improve self-care support and skills. The course is designed for anyone with a self-defined long-term condition, and attracts a heterogeneous group of patients. A randomised controlled trial has demonstrated effectiveness in improving subjective health. However, it is not known whether particular patient characteristics predict the impact of the course.
Aim To determine whether baseline characteristics predict clinical outcomes from attendance at a chronic disease self-management course; and to assess whether identification of such characteristics assists in targeting the course to individuals most likely to benefit.
Design of study A post-hoc subgroup analysis of data from a randomised controlled trial to explore predictors of three trial outcomes: self-efficacy, energy, and health-related quality of life.
Setting Participants with self-defined long-term conditions (n = 629) were recruited from community settings in all 28 strategic health authorities in England.
Method Multiple regression was used to examine interactions between baseline variables and trial outcomes.
Results The predictors demonstrating significant interactions were: age and general health, and baseline values for self-efficacy, energy levels, and health-related quality of life.
Conclusion Participants with lower self-efficacy and health-related quality of life at baseline demonstrated more positive health outcomes. The Expert Patients Programme may have a protective effect on health-related quality of life for patients with poor health and low confidence. Younger people benefited substantially more than older people. Results suggest that positive outcomes associated with the course will be demonstrated with a wide variety of patients, although it may be worthwhile encouraging attendance of younger patients, those lacking confidence, and those coping poorly with their condition.
INTRODUCTION
Recent government policy advocates self-care support to improve health for people with long-term conditions.1 Chronic disease self-management courses are one approach to self-care support. In the English NHS, the Expert Patients Programme has piloted a course open to anyone with a self-defined long-term condition.2 The Expert Patients Programme course was modelled on the Chronic Disease Self-Management Program, developed at Stanford University,3 which was based on four conditions (arthritis, heart disease, lung disease, or stroke).3,4 Further trials of the course have recruited patients with a self-defined long-term condition,5 adapted the generic programme to specific cultures,6–10 and tested condition-specific adaptations.11–13
A recently completed randomised controlled trial of the Expert Patients Programme showed it was effective in improving subjective measures of health, including a medium effect on self-efficacy (confidence in managing the effects of long-term conditions; effect size = 0.4), and small effects on energy (effect size = 0.2) and health-related quality of life (providing the equivalent of one extra week of perfect health per year).5 These findings accorded with previous trials of the Stanford course.3
The Expert Patients Programme trial had wide inclusion criteria to reflect the broader programme's philosophy of social inclusion: trial patients varied in demographic and health-related characteristics. Therefore, identifying groups of patients for whom the self-management course is most effective is an area for further research.
Secondary analyses to identify such subgroups have so far shown varied results. The initial trial of the self-management course found that outcomes did not vary between different conditions (arthritis, heart disease, stroke, and comorbid conditions).3 A secondary analysis of a culturally-adapted course also found no difference in effect by condition or sex.7 One study found indications that responses to the course varied according to cultural group (Vietnamese, Chinese, Italian, and Greek), with Vietnamese participants showing most change and Italians the least.9
Given the highly varied patient population that enters the Expert Patients Programme, a secondary analysis to identify patient characteristics associated with outcomes is potentially useful in helping NHS clinicians and service commissioners to target patients who are most likely to benefit. A previous study used analytic techniques to identify determinants of benefit, with the aim of developing screening tools to maximise the impact and cost-effectiveness of interventions.14
METHOD
Patients and intervention
The Expert Patients Programme is a group intervention (with 8–12 participants) which is led by trained lay people with experience of long-term conditions. It is designed to help participants to develop appropriate self-care skills. The intervention is an adapted and anglicised version of the Stanford Chronic Disease Self-Management Program.3 The course involves six 2.5-hour group sessions held weekly in non-NHS premises. The intervention is conducted according to a written manual, and includes sessions on relaxation, diet, exercise, fatigue, breaking the ‘symptom cycle’, managing pain and medication, and communication.
The trial was designed to reflect the broader Expert Patients Programme, and no specific inclusion or exclusion criteria were used beyond a self-defined long-term condition. Recruitment was carried out at community settings in all 28 strategic health authorities in England.
Trial design
The trial methods and results have been reported in detail elsewhere.5 In summary, the design was a two arm pragmatic randomised controlled trial with a waiting-list control group. A total of 629 patients were recruited between April 2003 and April 2005. Follow-up was at 6 months after baseline.
How this fits in
There is increasing evidence of the effectiveness of chronic disease self-management courses. Recent research has found they may have a small-to-moderate effect in improving people's subjective health. However, there is a lack of knowledge about the characteristics of patients who might benefit most from such an approach. This research addresses this and shows that younger patients and those who lack confidence and cope poorly with their condition may gain the most from attending an Expert Patients Programme.
Measures
Outcomes examined in the present analysis were restricted to a priori primary outcomes for which the Expert Patients Programme was found to have a significant effect:
Self-efficacy15 — the self-efficacy scale contained 19 items related to confidence in: achieving exercise participation (three items), and managing disease (five items), symptoms (five items), and depression (six items). Each item was scored on a 10-point scale ranging from ‘not at all confident’ to ‘very confident’. The final score was the mean of the four subscales expressed out of 100.
Energy15 — the energy scale had five items (for example, ‘Did you feel worn out?’, ‘Did you have enough energy?’) scored on a six-point scale ranging from ‘none of the time’ to ‘all of the time’. The final score was a sum of the items expressed out of 100.
Health-related quality of life — the EQ-5D, which is the EuroQol Group's health status instrument (five-dimensional format), measures patient health status across five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with three possible responses (no problem, moderate problems, or severe problems). This allows categorisation of patients according to state of heath, and each state is mapped onto a scale where zero equates to dead and 100 equates to full health, based on interviews with a sample of 3395 members of the UK public.16
One other primary trial outcome, health service use (the sum of self-reported GP visits, accident and emergency attendances, and outpatient visits), was not affected by the intervention and does not appear as an outcome in the present analysis.
The selected predictors included a range of sociodemographic variables and baseline values of the trial outcomes. Appendix 1 shows that the two groups were well balanced on all predictors at baseline.
Analysis
Analyses were conducted using multiple regression in Stata (version 9). To test whether a predictor moderated the effect of the course on the outcome variable (self-efficacy, energy, or health-related quality of life), the regression included terms representing the predictor's main effect and its interaction with treatment group.17
A separate regression was run for each predictor. Initially, the model consisted of treatment group, baseline value of the outcome, and the stratification used in the original randomisation: age category, sex, condition, general health, accommodation type, and ethnicity.
The predictor was then added as a main effect which was tested by determining if this improved the model (that is, significantly increased the R2 value), before adding and testing its interaction with treatment group.
Courses were clustered within tutor/trainer teams, based in strategic health authorities. Because the number of authorities was large relative to sample size, the study did not cluster by strategic health authority in the main analysis;5 instead, regressions were repeated with an adjustment for strategic health authority in a sensitivity analysis. Findings that were not supported by the sensitivity analysis are indicated in the Appendices 2 and 3. Interactions were tested using an alpha level of 5%.
RESULTS
P-values for the interactions and main effects were summarised (Appendix 2). Main effects measure the impact of a predictor on an outcome regardless of treatment group; these are reported purely for completeness and are not discussed further. Also, interpretation of main effects must be cautious for variables involved in a significant interaction. Six interactions were significant in both the primary and sensitivity analyses, related to age, general health, and baseline values for self-efficacy, energy, and health-related quality of life. To assist in interpreting these interactions, the scores were subdivided on each predictor into three subgroups (as equal in size as the data allowed, with the exceptions of age and general health which were pre-classified), and an effect size was calculated (Cohen's d) for each subgroup (Appendices 2 and 3). In accordance with Cohen, an effect of 0.2 was taken to be small, 0.5 to be moderate, and 0.8 to be large.18
Predictors of self-efficacy
The Expert Patients Programme had a significantly greater impact on the self-efficacy of participants with low self-efficacy scores at baseline (P = 0.006), compared with those who began with higher scores (Appendices 2 and 3). The effect on participants in the lower third of scores at baseline was moderate to large (effect size = 0.56; 95% confidence interval [CI] = 0.37 to 0.75), but only small for those with scores in the upper third (effect size = 0.22; 95% CI = 0.02 to 0.41; Figure 1).

Relationship between change in self-efficacy and baseline self-efficacy score, by treatment group (adjusted for patient age, sex, ethnicity, disease condition, general health, and accommodation). Error bars indicate 95% confidence intervals. EPP = Expert Patients Programme.
Although there was little or no improvement in self-efficacy for those who scored well initially, possible gains at the high end were restricted by the ceiling on self-efficacy scores (maximum possible score is 100). There is also weak evidence (P = 0.035) that the course had a greater impact on the self-efficacy of people who scored poorly in terms of health-related quality of life at baseline (Appendices 2 and 3), even after controlling for baseline self-efficacy scores.
Predictors of energy
In terms of energy, the Expert Patients Programme had a substantially greater effect on younger participants (P = 0.006). Patients under 40 years of age improved their energy score by an average of 13.0 (95% CI = 8.0 to 18.0) points, compared with mean gains of 4.2 (95% CI = 1.2 to 7.2) points and 2.7 (95% CI = 0.1 to 5.3) points for participants in the older age groups (Figure 2). In all age groups, control patients showed only small changes in mean energy levels.
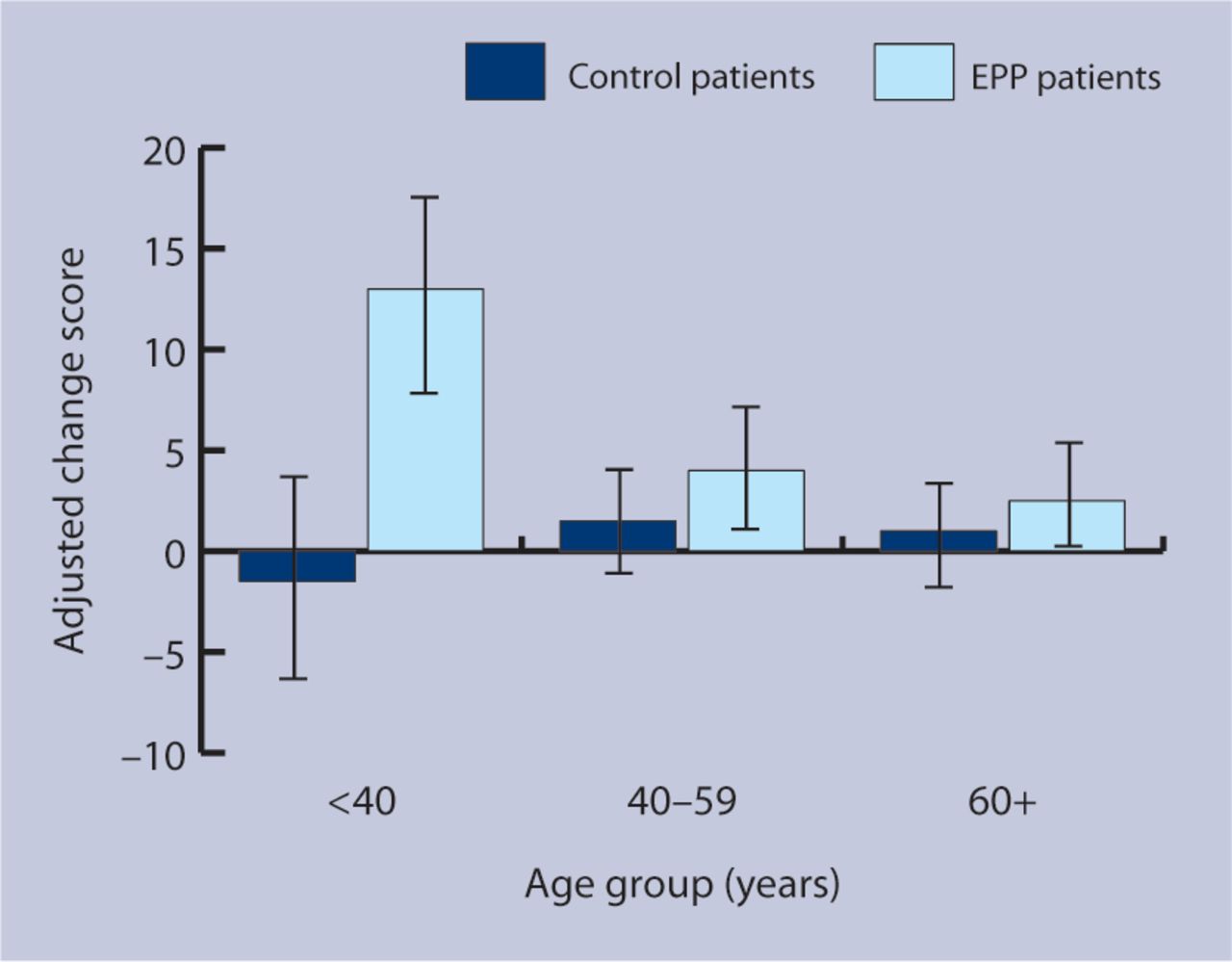
Relationship between change in energy and patient age, by treatment group (adjusted for energy score at baseline and patient sex, ethnicity, disease condition, general health, and accommodation). Error bars indicate 95% confidence intervals. EPP = Expert Patients Programme.
Predictors of health-related quality of life
The impact of the Expert Patients Programme on heath-related quality of life was significantly related to baseline levels of general health (P = 0.022), self-efficacy (P = 0.007), and health-related quality of life (P = 0.013). Relative to equivalent control patients, course participants who were initially at the lowest levels on these measures benefited most from the course. Effect sizes were small to moderate (Appendix 3), but the finding may be important for other reasons. Figure 3 shows that, whereas health-related quality of life declined in control patients with low-to-moderate levels of self-efficacy, no such decline occurred in intervention patients who, at baseline, had equivalent levels of self-efficacy. A similar result was observed in those with poor general health.

{kind=link}
{kind=link}
{kind=link}
Relationship between change in health-related quality of life and baseline self-efficacy, by treatment group (adjusted for health-related quality of life at baseline and patient age, sex, ethnicity, disease condition, general health, and accommodation). Error bars indicate 95% confidence intervals. EPP = Expert Patients Programme.
DISCUSSION
Summary of main findings
Results suggest that people who have lower self-efficacy and health-related quality of life at baseline gain most from the Expert Patients Programme. Younger people may also benefit substantially more than older people, although no other sociodemographic predictors of benefit from the Expert Patients Programme were identified.
Strengths and limitations of the study
Participants were volunteers with an interest in attending an Expert Patients Programme; therefore, the results and the subgroup analyses may not generalise to the wider population with long-term conditions.
The randomised controlled trial was not powered to detect predictors of outcome. Low power is sometimes used to argue against interaction tests, but it is also argued that they are of value for that very reason: they inhibit false or premature claims.17 In general, only strong interaction effects will reach statistical significance if the trial has low power. To aid interpretation, effect sizes were calculated for subgroups of the sample. The effect size estimates are precise enough (with error bounds of ±0.2 or less) to distinguish confidently between small, moderate, and large effects.
The large number of statistical significance tests conducted increased the likelihood that at least one test is significant by chance.19 This risk could be reduced by adjusting the α level for significance, for example via the Bonferroni method.20 However, protecting the type 1 error rate (the chance of falsely rejecting even a single test) increases the likelihood of type 2 errors (the chance of failing to detect one or more genuine relationships).21 The desirable balance between these two kinds of error depends on the application. For the purposes of exploratory analysis and hypothesis generation, it is important that the type 2 rate is not too high, or potentially important relationships may be excluded prematurely.22,23 For this reason, the conventional level of significance, P<0.05, was used.24
Guidelines concerning secondary analyses highlight a number of important methodological considerations other than statistical significance.19 Considerations relevant to the current results are: clinical significance of the results; whether the hypothesised predictors of outcome were specified in advance; consistency of the findings with the wider literature; and existence of indirect evidence that supports the hypothesised difference. Caution is necessary in interpreting the current analyses, as a relatively large number of predictor variables were tested, which were not specified in advance. Partly this reflects the lack of a comprehensive theoretical model that would allow such prespecification. The predictors tested were those available in the trial data set. Other unmeasured variables (for example, personality and social support) may be important predictors, but the need to minimise responder burden made more comprehensive assessment inappropriate.
Comparison with existing literature
The present findings concur with previous analyses showing that patients' underlying conditions do not predict any difference in outcomes.3,7 However, analyses of the impact of baseline self-efficacy and health have not been reported previously. It is also suggested that other research teams who have undertaken recent trials of chronic disease self-management courses7,11 investigate whether the present results can be replicated.
Implications for future research and clinical practice
The current results require validation by other studies, and if that occurs there are several important implications for the delivery of the Expert Patients Programme. This trial included an accompanying process evaluation which illuminated a number of practical implementation issues related to recruitment to the Expert Patients Programme. Recruitment of participants during the pilot phase was problematic, because the programme did not fit well with current delivery of chronic disease-management services in primary, secondary, and social care. Also, professionals were not engaged either in recruitment to courses or incorporating self-care skills training into their work with patients.25 It was found that Expert Patients Programme staff concentrated on ‘easy’ targets for recruitment (for example, patient support groups whose members are likely to appreciate and value self-care skills), to ensure there were enough course participants.26 As a result, recruitment tended to be biased towards people who were already good self-managers.
The present analysis suggested that patients with low self-efficacy and poor health gain most from the course, and might encourage service commissioners and healthcare professionals planning courses in chronic disease self-management to concentrate resources on targeting people who lack confidence in their abilities to self-manage, or who are coping badly. However, some caution must be applied, as those with very low self-efficacy and health at baseline may not have entered the trial at all, and may not demonstrate the same degree of improvement as patients in the current study.
Younger people were more likely to benefit from the Expert Patients Programme in terms of energy gain. A patient experience study by the present authors (not yet published) indicated that younger people found the course set up and group discussions unappealing, mainly because the majority of those on courses were older people with different needs or experiences. Possibly, more could be done to make the course more appropriate to the needs of younger participants (for example, increasing the focus on employment-related issues), to ensure that they are satisfied with the course and have improved outcomes.
The present results suggest that the Expert Patients Programme may have a protective effect on health-related quality of life for patients with poor health or low confidence. The course can help such patients to resist a deterioration in their health-related quality of life that would otherwise have occurred. If this is the case, the results have important implications. However, the finding is the outcome of a complex analysis controlled for many co-varying factors, and would need confirmation in other studies.
This study replicates previous findings that the patients' underlying conditions do not predict any difference in outcomes.3,7 This result strengthens the argument that self-care support can be provided on a generic basis, which may be easier and more efficient to provide. However, it should be noted that the patient experience study did report some dissatisfaction, among a proportion of patients, with the lack of disease-specific information provided.26
In summary, to maximise the impact and benefit of the Expert Patients Programme, more effort could be made to encourage health professionals to refer patients who are likely to be lacking in confidence or ability to self-manage. Changes to the course in order to make it more attractive to younger patients may also be required.
Acknowledgments
The authors would like to thank Fran Morris, Claire Chandler, and Sophie Jerrim for their hard work in the administration of the trial; the patients who kindly agreed to participate and complete the written assessments; the staff within the Expert Patients Programme and the primary care trusts who helped recruit patients; and Ayesha Dost and Geoff Royston at the Strategy Directorate of the Department of Health. NPCRDC is a department of the University of Manchester but is funded by the Department of Health. The views expressed in this paper are the views of the authors and not the funding body.
Appendices
Baseline predictors and comparison of intervention and control groups.
Summary of P-values for main effects and interactions.
Subgroup effect sizesa for significant interactions.
Notes
Funding body
The randomised controlled trial this study is based on was funded by the Department of Health (trial identifier: ISRCTN7053234)
Ethical approval
Ethics approval for the trial was given by North West MREC (MREC 03/8/3)
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss.
- Received May 30, 2007.
- Revision received August 2, 2007.
- Accepted December 17, 2007.
- © British Journal of General Practice, 2008.
REFERENCES
In this issue









More in this TOC Section
Related Articles
Cited By...

