


Abstract
Background GPs investigate approximately half of all infertile couples with semen analysis and endocrine blood tests. For assessment of tubal status, hysterosalpingography (HSG) is recommended as a first-line investigation for women not known to have comorbidities.
Aim To test whether providing GPs with open access to HSG results in infertile couples progressing to a diagnosis and management plan sooner than with usual management.
Design of study A pragmatic cluster randomised controlled trial.
Setting Seventy-one of 173 general practices in north-east England agreed to participate.
Method A total of 670 infertile couples presented to 33 intervention practices and 25 control practices over a 2-year period. Practices allocated to the intervention group had access to HSG for those infertile women who fulfilled predefined eligibility criteria. The primary outcome measure was the interval between presentation to the GP and the couple receiving a diagnosis and management plan.
Results An annual incidence of 0.8 couples per 1000 total population equated to each GP seeing an average of one or two infertile couples each year. Open access HSG was used for 9% of all infertile women who presented to the intervention practices during the study period. The time to reach a diagnosis and management plan for all infertile couples presenting was not affected by the availability of open access HSG (Cox regression hazard ratio = 0.9, 95% confidence interval [CI] = 0.7 to 1.1). For couples who reached a diagnosis and management plan, there was a non-significant difference in time to primary outcome for intervention versus control practices (32.5 weeks versus 30.5 weeks, mean difference 2.2 weeks, 95% CI = 1.6 to 6.1 weeks, P = 0.1). The intracluster correlation coefficient was 0.03 across all practices.
Conclusion Providing GPs with open access to HSG had no effect on the time taken to reach a diagnosis and management plan for couples with infertility.
- family practice
- health services accessibility
- hysterosalpingography
- infertility
- primary health care
- randomised controlled trial
INTRODUCTION
Infertility affects approximately one in six couples during their lifetime,1,2 and a GP can expect to see one or two new infertile couples each year.1,3 GPs usually undertake an initial assessment of male fertility status and female ovulation status, with assessment of tubal patency being done under specialist care. In recent years the increasing regulation of fertility treatments has led to services being concentrated in dedicated tertiary care facilities.4 Referral of infertile couples to non-licensed units may delay access to definitive treatment. The inclusion of assisted reproduction in national 18-week-to-treatment targets requires a more rapid investigation and referral pathway. Recent National Institute for Health and Clinical Excellence (NICE) guidelines on assessment and treatment for people with fertility problems5 includes a recommendation that hysterosalpingography (HSG) should be considered as a first-line investigation for tubal status for women not known to have any comorbidities.5 Direct access to HSG is recommended for the primary assessment of infertile couples on the NHS 18-week commissioning pathway website.6 This may contribute to a reduction in time from referral to definitive treatment. This research tested whether providing GPs with open access to HSG enabled the infertile couple to reach a diagnosis and management plan sooner than with usual management.
How this fits in
In the diagnostic process of infertility, GPs do not routinely have access to hysterosalpingography. However, women with tubal infertility identified on hysterosalpingography require referral for in vitro fertilisation or intracytoplasmic sperm injection at a Human Fertilisation and Embryology Authority-licensed tertiary care fertility unit.
METHOD
Setting and participants
Seventy-one of the 173 practices (41%) approached in the Newcastle upon Tyne, North Tyneside, South Tyneside, Gateshead, and Northumberland Primary Care Trust areas agreed to take part. All GP principals within the practice signed a statement of intent to participate in the study (cluster-level consent),7 and were invited to a local launch meeting where trial allocation was revealed and literature, including a one-page summary of the NICE guidance on infertility management, was provided. Intervention practices also received open access HSG and hospital radiology request forms as well as patient information leaflets for the HSG procedure. Written consent of couples entering the trial was obtained by their GPs (patient-level consent). Incident cases of infertile couples presenting to their GP between 31 December 2004 and 31 December 2006 were eligible to enter the trial. The general practice complete electronic clinical records including scanned correspondence from hospitals were the primary data source for the study.
Design
This was a 1:1 cluster-randomised controlled trial with the practices as the unit of randomisation. Practices were stratified by geographical area.8 A permutated block design within each stratum ensured balanced allocation between intervention and control practices for large (>4 whole-time equivalent [WTE] GPs), intermediate (2–4 WTE GPs), and small (<2 WTE GPs) GP practices. Practices were randomly allocated, using SPSS (version 14.0), to intervention or control by a statistician with no prior knowledge of the practices.
Intervention
Intervention practices were able to request HSG through an open access service if their patients fulfilled predetermined eligibility criteria (Box 1). Use of the investigation remained at the discretion of the GP and the consenting woman. The open access service was provided at the radiology department of the Royal Victoria Infirmary, Newcastle upon Tyne (for Northumberland, Newcastle, North Tyneside) and at the Queen Elizabeth Hospital, Gateshead (for Gateshead and South Tyneside). In the control practices GPs did not have access to HSG, and following referral the investigation was traditionally requested by fertility specialists.
Box 1. Criteria for open access hysterosalpingography.
▸ The couple must have been trying to conceive for 1 year
▸ Normal semen analysis
▸ Normal coital function
▸ Female aged <40 years
▸ Regular menstrual cycle (<6 weeks)
▸ Day 2–5 follicle-stimulating hormone <10 IU/l
▸ Mid-luteal progesterone >20 nmol/l
▸ No history of tubal disease
▸ No known uterine or cervical abnormality
▸ Negative endocervical swabs for chlamydia and gonococcus
▸ Rubella status checked
▸ Female in receipt of folic acid
Objective
The study objective was to evaluate the effect of providing GPs with open access to HSG on time to diagnosis and completeness of the initial assessment for infertile couples. The latter was defined by the NICE recommendation which was embedded within the open access HSG criteria (Box 1).
Outcomes
The primary outcome was the time taken from presentation to the GP and the couple receiving a definitive cause and management plan for their infertility from a fertility specialist or their GP. A management plan was defined by the offer of treatment, whether ovulation induction with clomifene, in vitro fertilisation, intracytoplasmic sperm injection, donor eggs or sperm, weight loss, intrauterine insemination, or reversal of sterilisation, or no treatment offered. Couples with no record of a diagnosis and/or management plan were considered not to have reached the primary outcome. A secondary outcome was the completeness of the initial assessment for infertile couples.
Sample size
Assumptions were that the data were normally distributed with similar standard deviations, that an average practice of three GPs would see six couples in 1 year,1 and that 50% of all infertile couples would be recruited to the trial, with approximately 50% eligible for open access HSG, giving an estimated 1.5 HSG referrals from each practice, that is a 25% uptake of the intervention. The estimated time to diagnosis and management plan for controls was 26 weeks (standard deviation [SD] 14 weeks).3 With a best estimate for the intracluster correlation coefficient of 0.01,9,10 to detect a 30% (26 weeks to 18 weeks) reduction in primary outcome with 80% power and 5% significance level, 36 practices (54 couples or 216 assuming 25% uptake) would be required in each arm of the trial.
Statistical methods
Data were analysed using SPSS and MLwiN. A survival analysis using a Cox proportional hazards model11 was used to account for couples that had not reached the primary outcome measure. For couples that reached the primary outcome measure, a cluster analysis using multilevel modelling (MLwiN) was employed.12 The effect of clustering was quantified using patient- and practice-level variances and presented as the intracluster correlation coefficient for the primary outcome measure. Adjusted mean differences between groups are presented with 95% confidence intervals (CI), and P<0.05 was considered significant.
Secondary analyses on the primary outcome were adjusted for the effect of geographical area, use of open access HSG, and place of referral.
Secondary outcomes were a measure of the uptake of open access HSG and a logistic regression model for binomial response data (investigations performed in both groups), adjusting for patient clustering.
RESULTS
Participant flow
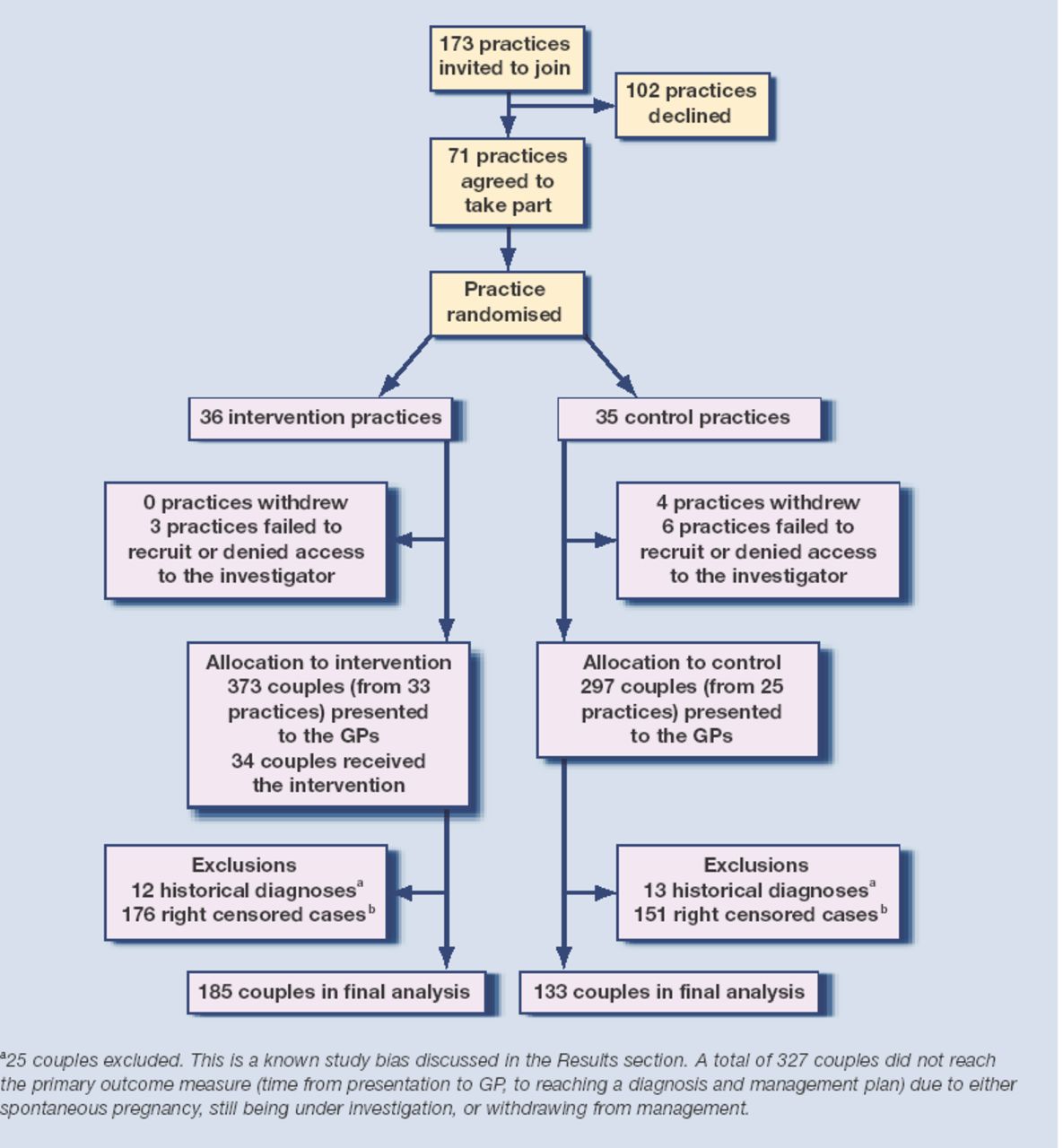
There were 670 incident couples over the 2-year period from 58 practices (Figure 1), with a combined list size of 403 263 patients (72 182 being women aged 16–42 years). This represents an annual incidence of 0.8 infertile couples per 1000 total population, or 4.6 couples per 1000 women aged 16–42 years. Characteristics of the trial participants are shown in Table 1.

Practices and participant flow.
Characteristics of the trial participants.
Initial investigations recommended by the NICE guideline, that is, semen analysis, mid-luteal progesterone, and follicle-stimulating hormone (FSH), were done for between half and two-thirds of couples. Of those couples referred (479/670), GPs were most efficient at passing on information about the length of time a couple were trying to conceive, their fertility status, menstrual cycle status, and mid-luteal progesterone result (Table 2).
Information recorded on GP medical record and referral letter; number (%).
Primary outcome
The time from first presentation to diagnosis and management plan comprises three elements: time from presentation to the GP to being referred, time from referral to being seen by the fertility specialist, and time from being seen by the fertility specialist to the couple receiving a diagnosis and management plan. In this study these intervals were 7.1 weeks (SD = 9.7), 9.7 weeks (SD = 4.4), and 14.3 weeks (SD = 13.6) respectively. Three per cent (11/343) of couples were given a diagnosis and management plan by their GP.
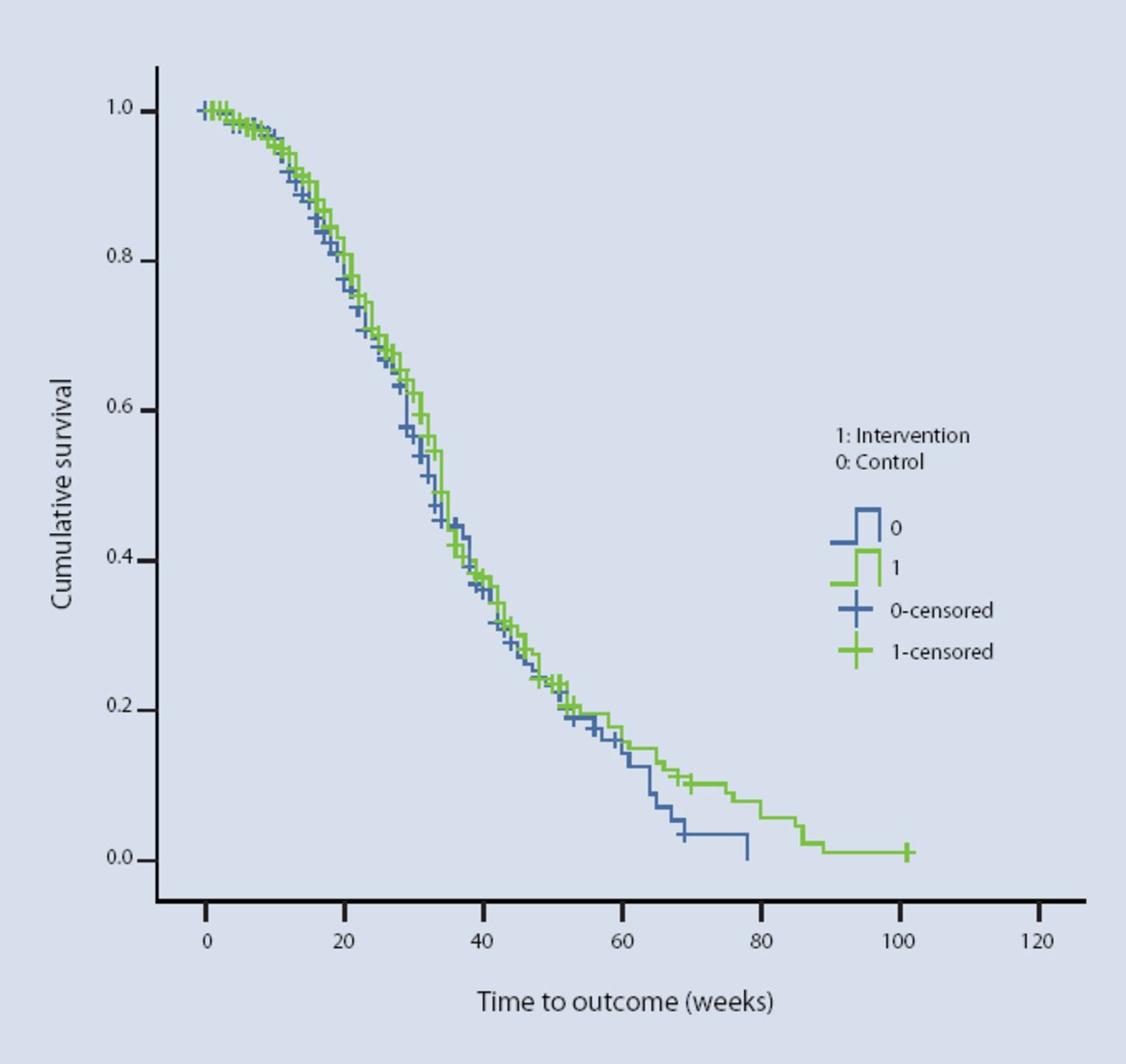
For all couples (n = 670), a Kaplan-Meier survival analysis and Cox regression/proportional hazards model (hazard ratio 0.9, 95% CI = 0.7 to 1.1, P = 0.3) demonstrated a non-significant difference between intervention and control couples reaching the primary outcome (Figure 2). A definitive diagnosis and management plan was reached by 343 (51%) couples (Table 3). Twenty-five couples (12 from intervention and 13 from control) who had an historical diagnosis were excluded, leaving 318 couples (133 control and 185 intervention) in the final analysis.

{kind=link}
{kind=link}
Kaplan-Meier survival curve: probability of reaching the primary outcome — intervention versus control.
Outcomes of infertile couples presenting to GPs; number (%).
Multilevel modelling on couples reaching outcome (n = 318 couples)
The intracluster correlation coefficient was 0.03 across all practices. There was a non-significant difference in time to primary outcome for intervention versus control practices (32.5 versus 30.3 weeks, mean difference 2.2 weeks, 95% CI = −1.6 to 6.1 weeks, P = 0.1).
Secondary analyses on the primary outcome: factors influencing time to definitive diagnosis and management plan
There were significant differences between areas; the average time to definitive diagnosis and management plan varied from 27.8 weeks (Gateshead) to 34.8 weeks (Northumberland).
Thirty-four couples underwent open access HSG. Mean time to primary outcome was 22.0 weeks compared to 32.5 weeks for couples that did not have open access HSG (mean difference −10.5 weeks, 95% CI = −16.4 to −4.6 weeks, P<0.001). Two-thirds of couples that had open access HSG performed (23/34) were subsequently referred. For all couples referred in the trial (n = 479), the completeness of information passed on in the referral letter was greater for patients who had undergone HSG (Table 4); however, this was not statistically significant given the small numbers in the open access HSG group. When compared with referrals to tertiary fertility units, referrals to secondary care took 8.7 weeks longer (95% CI = 5.2 to 12.2 weeks) to reach the primary outcome measure, but couples referred privately reached the outcome 8.3 weeks sooner (95% CI = −17.7 to 0.8 weeks).
Information recorded in the referral letter for all 479 couples referred in the trial; number (%).
Secondary outcomes
The uptake of open access HSG in the intervention practices was 9% (34/361). Intervention practices were no more likely than control practices to perform the initial investigations recommended by NICE guidance; semen analysis (adjusted odds ratio [OR] 1.1, 95% CI = −0.5 to 2.7, P = 0.3), mid-luteal progesterone (adjusted OR = 1.1, 95% CI = −0.5 to 2.7, P = 0.3), and serum FSH (adjusted OR = 1.1, 95% CI = −0.3 to 2.7, P = 0.3); (Table 2).
DISCUSSION
Summary of main findings
Making HSG available to GPs did not decrease the time taken for couples to reach a definitive diagnosis and management plan. Nine per cent of couples in the intervention arm of the study were referred for open access HSG, and these couples reached a diagnosis and management plan 12 weeks earlier compared with usual management. One-third of couples that had open access HSG performed were not subsequently referred as the GPs adopted a process of ‘watchful waiting’ with a diagnosis of unexplained infertility. For couples that had open access HSG performed, the guidance on initial investigations embedded within the form increased the likelihood that they were completed. Only 3% of the variation in primary outcome can be explained by clustering within practices, with most of the variation occurring at the patient level, showing that there is consistency of fertility management between practices.
Strengths and limitations of the study
This was a pragmatic trial that gives a measure of the usefulness of open access HSG in usual clinical practice. By randomising practices rather than individual GPs, contamination bias and selection bias were minimised. However, a high dropout rate of control practices may have contributed to a post-randomisation selection bias. Stratification minimised biases due to differential access and referral patterns. Following practice randomisation, differential recruitment within intervention and control clusters remained an ever present threat. There was low uptake of open access HSG by the intervention practices, which diluted its effect size. The secondary per protocol ‘on treatment’ analysis was underpowered and biased. Those that received open access HSG and were subsequently referred, not surprisingly, had better information transferred in the referral letter, which probably reflected individual GP interest in fertility management.
Comparison with existing literature
The incidence (one couple per 1000 population)1,13 and management of infertility in primary care has remained largely unchanged over the last 10 years.3,14–16 One survey has shown that 60–80% of GPs agree that the initial investigations recommended by the Royal College of Obstetricians and Gynaecologists and subsequently by NICE should be carried out in primary care.17 Clinical guidelines alone, however, are generally insufficient to influence GPs' behaviour and referral patterns,18–21 and the implementation of guidelines should be tailored to identify potential barriers.22 Two studies on infertility guidelines have shown a modest improvement in GP referral patterns,23,24 although this change in behaviour was not sustained.15 Embedding clinical guidelines within the open access referral process has been shown to increase compliance with referral standards and improved service efficiency for open access gastroscopy and open access urological investigations.25,26 The uptake of open access HSG was low in this study, with only 9% of couples being referred. Data that became available during this study suggested that 26% of couples presenting to GPs could be eligible for open access HSG based on this study's criteria.27
Implications for future research and clinical practice
Some GPs have shown a willingness to use criteria-driven open access HSG, enabling a management plan to be established at the first specialist consultation. In this study, 9% of couples benefited from open access HSG and reduced the duration of their ‘patient journey’ from presentation to the GP to specialist treatment, although this still fell short of the government 18-week target.28 If open access HSG is introduced for GPs, future research will need to assess its impact on the whole patient journey, referral patterns, and cost-effectiveness.
Acknowledgments
Academics within Sunderland University contributed to the study design; collection, analysis, and interpretation of data; production of the paper and the decision to submit the article for publication.
Notes
Funding body
We would like to acknowledge the NHS National Coordinating Centre for Research Capacity Development who funded this work through a National Institute for Health Research (NIHR) award held by Dr Scott Wilkes (RDA03/26); Primary Care Researcher Development Award, National Coordinating Centre for Research Capacity Development, Leeds Innovation Centre. All researchers involved in the production of this paper are independent from the funder. The trial is Current Controlled Trials ISRCTN18398372
Ethics committee
Ethical approval was granted from Newcastle and North Tyneside as the main REC with SSA approval from Northumberland, Gateshead, and South Tyneside Local Research Ethics Committees. Approval was also granted from Sunderland University Research Ethics Committee
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received August 9, 2008.
- Revision received October 27, 2008.
- Accepted December 19, 2008.
- © British Journal of General Practice, 2009.
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

