


Abstract
Background There is a paucity of randomised controlled trials of weight management in primary care.
Aim To ascertain the feasibility of a full trial of a nurse-led weight-management programme in general practice.
Design of study Factorial randomised control trial.
Setting Primary care, UK.
Method A total of 123 adults (80.3% women, mean age 47.2 years) with body mass index ≥27 kg/m2, recruited from eight practices, were randomised to receive structured lifestyle support (n = 30), structured lifestyle support plus pedometer (n = 31), usual care (n = 31), or usual care plus pedometer (n = 31) for a 12-week period.
Results A total of 103 participants were successfully followed up. The adjusted mean difference in weight in structured support compared to usual care groups was −2.63 kg (95% confidence interval [CI] = −4.06 to −1.20 kg), and for pedometer compared to no pedometer groups it was −0.11 kg (95% CI = −1.52 to 1.30 kg). One in three participants in the structured-support groups (17/50, 34.0%) lost 5% or more of their initial weight, compared to less than one in five (10/53, 18.9%) in usual-care groups; provision of a pedometer made little difference (14/48, 29.2% pedometer; 13/55, 23.6% no pedometer). Difference in waist circumference change between structured-support and usual-care groups was −1.80 cm (95% CI = −3.39 to −0.20 cm), and between the pedometer and no pedometer groups it was −0.84 cm (95% CI = −2.42 to 0.73 cm). When asked about their experience of study participation, most participants found structured support helpful.
Conclusion The structured lifestyle support package could make substantial contributions to improving weight-management services. A trial of the intervention in general practice is feasible and practicable.
INTRODUCTION
Obesity presents an unprecedented public health challenge.1 In England, 24% of adults (aged 16 years and over) were classified as obese in 2007; and around one-fifth of men and one-quarter of women displayed a high risk of obesity-related health problems.2 If current trends persist, 36% of men and 28% of women aged 21–60 years in England will be obese by 2015.3 The cost of treating the consequences of obesity were approximately £1 billion in 2002 (2.3–2.6% of NHS expenditure),4 and could exceed £3 billion by 2015.3 The National Audit Office recommends greater effort to establish an evidence-based methodology directed at overweight, enabling the NHS to adopt a more consistent approach.5 It is recognised that reducing obesity, improving diet, and increasing exercise are priorities,6 and that primary care provides a unique resource for the identification and management of overweight.4
Weight concern among British women is high, but many overweight men are unaware of the problem.7 Only half the possible beneficiaries from weight reduction try to lose weight, and few receive health professional advice. Clinician counselling and treatment for smoking is highly cost-effective,8 but primary care remains under-used for obesity control. Few interventions have a sustained impact on weight, hence the need for effective, practical weight-management interventions for primary care.
The current authors have developed a multi-component intervention as recommended by the Medical Research Council (MRC).9 A survey of GPs and nurses was conducted to ascertain current levels of provision;10 interviews with health professionals and patients were carried out to ascertain which tools would deliver appropriate care,11 and an intervention was developed, based on the findings; this was pre-tested in three practices, and a pilot trial was conducted.
This paper describes the pilot trial of this intervention which comprises: (1) weight-management training including use of the National Obesity Forum's CD-ROM, ‘Managing Obesity in Primary Care’; (2) structured discussions using a computer program co-developed by a GP-based dietitian; and (3) provision of pedometers. The study evaluated the acceptability of questionnaires, measurement procedures, and the 12-week intervention, to assess the feasibility of a large-scale longer-term randomised controlled trial.
METHOD
Participating general practices
Eight general practices were recruited from the MRC's General Practice Research Framework of 900 UK practices (9%) with an average list size of 7500 patients, whose characteristics follow UK population norms. The list size in the study practices ranged from 1700 to 17 000, with one to six GPs in each.
Participants
Each practice was asked to recruit 16 patients, which was considered feasible within the time frame. Participants were identified by research nurses or doctors, and posters were displayed so patients could self-refer. Inclusion criteria were: age ≥18 years, body mass index (BMI) ≥27 kg/m2, able to walk for at least 15 minutes, not pregnant, and not on weight-loss medication. GPs confirmed patient suitability.
Patients were telephoned and invited for an appointment to assess eligibility and obtain consent. Following full explanation of the study, 123 participants consented and were randomly allocated using a 2 × 2 factorial design to: structured support with or without pedometer, and usual care with or without pedometer. Randomisation, stratified by practice, was carried out centrally.
Individual 30-minute appointments were arranged for usual-care participants. Structured-support group participants were informed they would be contacted 12 weeks later for a 45 minute appointment. To avoid ‘contamination’, nurses were trained in structured support after they had completed follow-up of the usual-care group.
How this fits in
Primary care could have a substantial impact on the increasing prevalence of obesity and its adverse impact on health. The lack of a proven intervention that is feasible in general practice may deter health professionals from providing the appropriate level of support required by overweight and obese patients. This study demonstrates that nurse-led lifestyle support could make a substantial contribution to improving weight-management services, and that a randomised controlled trial of the intervention is feasible in general practice.
Nurse training
Nurses received training in the study protocol and use of pedometers (Model SW-200 Yamax Digiwalker, London, UK) in September 2005. After follow-up of the usual-care patients, they were sent the National Obesity Forum's interactive CD-ROM tool: ‘Managing Obesity in Primary Care’ with an A3 wall poster of the management algorithm. Additional training in weight management and use of the ProHealthClinical computer package (KasTech Ltd, Cambridge, UK) was provided in January 2006. The structured programme (Appendix 1) included topics for discussion and five clinical counselling constructs: assess, advise, agree, assist, arrange.12 Nurses helped patients set realistic weight targets, aiming for a weekly loss of 0.5–1.0 kg; focused on long-term lifestyle changes; used a balanced healthy diet approach tailored to the individual's food preferences using ProHealthClinical suggested physical activity that could be incorporated into patients' everyday lifestyles; used behaviour change techniques including keeping a diary; and offered advice on coping with lapses and high-risk periods, such as Christmas and holidays.
Measurements
Height, weight, waist circumference, and blood pressure were measured; fasting blood samples were analysed for glucose and lipid profile. The self-completed questionnaires included validated measures of self-esteem,13 weight-related symptoms, quality of life, anxiety, depression, health status, and demographic details. These measures included the Hospital Anxiety and Depression Scale which performs well in primary care,14 and EQ-5D (EuroQol – 5 dimensions) and EQ-VAS (EuroQol Visual Analogue Scale), standardised non-disease-specific instruments for describing and valuing health-related quality of life, as generic measures of health status.15 To address the key domains relevant to obesity, the Obesity and Weight-Loss Quality of Life instrument was used, which measures the participants' global evaluation of position in life related to weight, weight loss, and weight-loss treatment; and the Weight-Related Symptom Measure,16 which focuses on the presence and ‘bothersome-ness’ of 20 symptoms commonly associated with obesity and obesity treatment. Additional questions were included in the final questionnaire on the experience of study participation. Participants randomised to receive a pedometer were shown how to use it, given a leaflet explaining the significance of 10 000 steps a day, and asked to record their steps each day. Nurses completed questionnaires on participants' obesity-related disease, smoking status, and current medication.
Statistical analysis
Data were entered using Epi-Info™, and analysed using Stata Statistical Software (version 10), on an intention-to-treat basis, with no substitution for missing data. The study was analysed as a factorial study using analysis of covariance for continuous outcomes. Comparisons between groups were performed using multivariable linear regression models, adjusting each intervention for the other, and for age, sex, and baseline value of the outcome variable. Changes were calculated as final value minus baseline value.
RESULTS
A total of 123 participants were recruited between October 2005 and March 2006, ages ranged from 22.1 to 68.5 years, weights from 66 to 165 kg, BMI from 27.6 to 50.9 kg/m2, and waist circumferences from 78 to 157 cm, and 95.8% (114/119) described themselves as white. Characteristics did not vary significantly by randomisation group (Table 1). Nearly 90% (105/119, 88.2%) said they were very or extremely motivated to lose weight, 16.1% (19/118) were ‘always on a diet’, and 8.4% (10/119) reported ‘always increasing physical activity’ to lose weight. Participants wanted to lose an average of 26.0 kg (standard deviation = 14.0 kg), representing 25.0% of their baseline weight.
Characteristics of participants at baseline.
Of the 122 participants who attended the baseline visit, 84.4% (103/122) were successfully followed up (Figure 1). Follow-up did not vary by randomisation group (P = 0.21) or baseline weight (P = 0.12), although non-completers were younger than completers (mean age = 40.7 and 48.4 years respectively; P = 0.007).

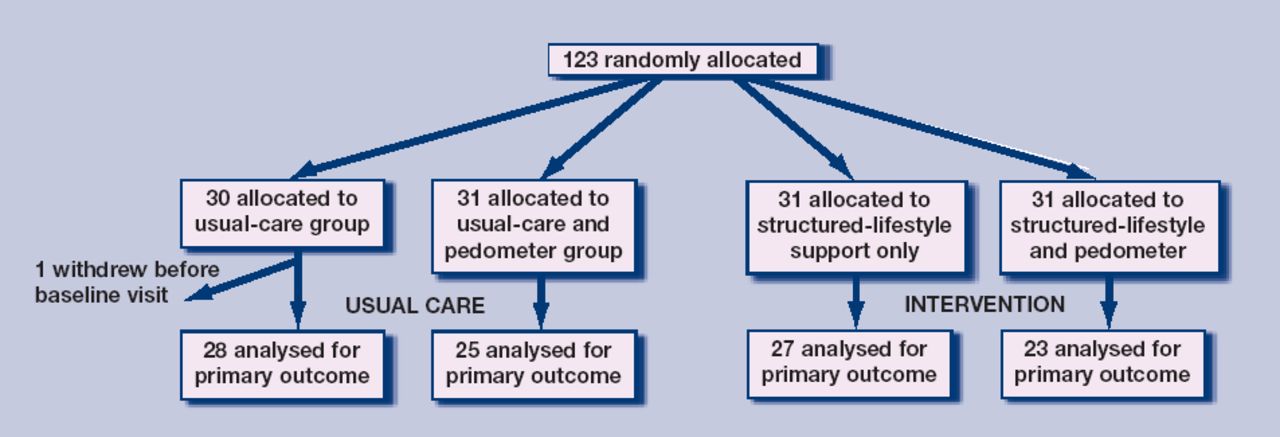{kind=link}
Participant flow.
Outcomes
The adjusted mean difference in weight in the structured support compared to usual care groups was −2.63 kg (95% CI = −4.06 to −1.20 kg), and in the pedometer compared to no pedometer group it was −0.11 kg (95% CI = −1.52 to 1.30 kg; Table 2).
Effect of the intervention on weight and waist circumference.
One in three (17/50, 34.0%) participants in the structured support group lost 5% or more of their baseline weight compared to fewer than one in five (10/53, 18.9%) in the usual-care group; provision of a pedometer made little difference (14/48, 29.2% pedometer group; 13/55, 23.6% no pedometer group). Assuming those lost to follow-up lost less than 5% would reduce these proportions somewhat (structured support: 17/61, 27.4%; usual care: 10/61, 16.4%; pedometer: 14/62, 22.6%; no pedometer: 13/61, 21.3%). Structured support resulted in a greater percentage weight loss than did usual care (adjusted difference mean −2.78%; 95% CI = −4.25 to −1.30%); provision of a pedometer did not affect the degree of weight loss (adjusted difference mean −0.36%; 95% CI = −1.82 to 1.10%; Table 2).
The difference in waist circumference change between the structured support and usual-care groups was −1.80 cm (95% CI = −3.39 to −0.20 cm), and between the pedometer group and no pedometer groups it was −0.84 cm (95% CI = −2.42, 0.73 cm; Table 2).
There was a trend for increasing improvement in blood pressure with increasing degree of weight loss (Appendix 2).
Weight loss was associated with improvement in weight-related quality of life, self-esteem, and health status; and decrease in weight-related symptoms, degree of their ‘bothersome-ness’, depression, and anxiety (Appendix 3). The level of change tended to be related to degree of weight loss.
The majority of participants reported finding structured support very or extremely helpful, particularly agreeing lifestyle goals (Table 3). While the majority of participants said they benefited from participation, a higher proportion in the structured-support groups reported satisfaction with level of weight loss, meeting their expectations, and achieving their goals (Table 4). The majority of participants in the pedometer group reported using the pedometer every day (28/44, 63.6%), or on most days (15/44, 34.1%). A majority of participants (55/97, 56.7%) said they would like to return monthly for continuing support.
Participants' views on elements of the nurse-led structured support (n = 45)a.
Participants' views on taking part in the trial.
Process evaluation
Participants were asked open-ended questions to ascertain their views on study participation. Benefits mentioned included: ‘knowing I was going to be weighed’, ‘pedometer encouraging extra exercise, setting daily goals’, ‘more aware of food quantities’, and ‘encouragement from the nurse’. They found that participation ‘changed my lifestyle totally’, ‘gave me focus-identified issues I could improve’, ‘made me walk more’, ‘[gave me a] good feeling to see graphs going down on computer’, and ‘gave me definite goal and deadline’. Participants particularly liked ‘being weighed regularly and getting support’ and being ‘able to talk to someone’. Some participants would prefer ‘being weighed every week’, ‘calorie-counted recipes’, and ‘info on exercise classes’. Personal illness, family circumstances, and holidays were reported as things that got in the way of participation. Participants would have liked to have lost more weight. Pedometers were helpful as ‘I realised how little I was active’ and ‘[it] spurred me on to walk more’, although some found it ‘uncomfortable to wear — often dislodged’, said it ‘got tiresome after a while’ and ‘kept forgetting to put it on first thing’.
DISCUSSION
Summary of main findings
While this study was not powered to compare differences in weight loss, the level achieved was a mean of 4.0 kg over 12 weeks for participants randomised to receive structured support compared to 1.2 kg in those receiving usual care. One-third (34.0%) of participants in the structured-support group achieved a clinically meaningful weight loss of 5% or more.
Strengths and limitations of the study
A few studies have reported weight reduction as a result of interventions in some patients,17–19 but interventions in this field are largely limited to obese patients or to overweight patients with comorbidities. This is the first study providing evidence for the feasibility of an randomised controlled trial for weight management in primary care, developed using a complex interventions strategy recommended by the MRC, and following the National Institute for Health and Clinical Excellence (NICE) guidance on the prevention, identification, assessment, and management of overweight and obesity.20 While the NICE guidelines provide a broad foundation, this study has developed a detailed programme of personalised advice and demonstrated its feasibility in primary care.
A cost-effectiveness analysis of the intervention was not carried out, nor did the study address the increased workload for nurses in general practice. Missing values were also excluded from the analysis rather than using multiple imputation methods.21 These aspects will be addressed in a full trial.
Intervention group entry was delayed until after control group follow-up to avoid contamination. This could introduce bias between groups if there were seasonal differences in weight or public health campaigns, although the difference in time was short. Any such bias could be avoided by a cluster randomised trial design, although contamination may be small and more than counterbalanced by the increased statistical power of an individually randomised trial.
Participants may have been selected or self-referred on keenness to lose weight, which is likely to reflect the type of patient presenting in general practice for advice on weight management.
Comparison with existing literature
The degree of weight loss achieved in this study was similar to the 3.34 kg average loss at 3 months in the Counterweight observational study,22 conducted in UK general practice. One-third of participants in the structured support group achieved clinically meaningful weight loss of 5%, compared to one-quarter in Counterweight.22 Similar levels have been reported from trials in primary care in US African–American women,23 and for overweight patients with hypertension in Finland.24 The present study achieved a follow-up rate of 84.4% compared to 54.6% at 3 months in Counterweight.22
Exercise appears to be the component of treatment most likely to promote long-term maintenance of reduced weight.25,26 Participants using a pedometer in this study lost an average of 2.5 kg, which was similar to those with no pedometer. However, patient-centred counselling in primary care has reportedly led to increased physical activity,27 and been associated with reduced weight, blood pressure, and cholesterol.28 A systematic review of studies using pedometers to increase physical activity and improve health showed an association with significant increase in physical activity of 26.9% above baseline, and significant decreases in BMI and blood pressure.29 A meta-analysis of pedometer-based walking programmes reported modest weight loss of 0.05 kg per week, with longer programmes leading to greater weight loss than shorter ones.30
Wider objectives of management of overweight and obesity such as optimising lipids, glycaemic control, and blood pressure, may be achieved by modest weight loss of 5–10%, improved nutrition, and modest increases in physical activity.31 Two recent reviews of randomised controlled trials in patients with hypertension or pre-diabetes reported such benefits from modest weight loss.32,33 Some effect on blood pressure, related to the degree of weight loss, was observed in the present study.
The high proportion of participants reporting anxiety and depression and problems with mobility, self-care, and carrying out usual activities reported here, has been observed by others; for example, raised BMI was associated with increased risk of depression in a cohort study conducted in Norway,34 and has been associated with lower health-related quality of life in the UK35 and US.36 In the present study, weight loss was related to reduction in anxiety and depression, and improvement in weight-related symptoms, self-esteem, and quality of life. Similar relationships have been reported for health-related quality of life16 and self-esteem.37
Healthcare professionals in general practice are often reluctant to counsel patients on weight management because of the perceived need for additional training.11 Nurses in the present study did receive training, and the majority of participants receiving structured support found study participation helpful in achieving their goals.
Implications for clinical practice
Obesity is significantly related to increased use of primary care and diagnostic services in the US,38 use of outpatient services and medical prescriptions in the UK,39 and increasing use of anti-obesity medication.40,41 The UK government aims to reverse the rising tide of obesity and overweight in the population.42 This study has developed an intervention, following guidelines recommended by NICE,20 and shown its implementation to be feasible in primary care. NICE guidelines stress the urgent need for well-designed randomised controlled trials to address the effects of non-pharmacological interventions and to evaluate multi-component interventions in primary care. The programme outlined here is now being evaluated in a fully powered long-term randomised controlled trial that includes cost-effectiveness and process evaluation.
Acknowledgments
We would like to thank the study participants; the nurses who implemented the study (Anna Baker, Lynn Crombie, Barbara Cunningham, Ursula Evans, Monica Lloyd, Clare Nicolle, Kate O'Brien, Hazel Price); members of the advisory group (Professor Philip James, Dr Susan Jebb, Professor Anthony Kessel, Dr Colin Waine, Dr Leslie Wilkie, Dr Paul Wilkinson); and Sandy Evans (KasTech) for contributing to the nurse training; and the senior nursing team (Kay Foulger and Nicky Fasey) at the GPRF coordinating centre.
Appendix 1. Structured programme overview.
Appendix 2. Relationship between degree of weight loss and physiological measuresa
Appendix 3. Relationship between degree of weight loss and psychological and quality of life measures.
Notes
Funding body
The work was supported by grants from the British Heart Foundation (PG/04/001) and the Department of Health
Ethical approval
Ethical approval was obtained from the North West of England MREC (05/MRE08/27), relevant local ethics committees, and the London School of Hygiene & Tropical Medicine ethics committee
Competing interests
The authors have stated that there are none
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received June 28, 2008.
- Revision received August 19, 2008.
- Accepted October 15, 2008.
- © British Journal of General Practice, 2009.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

