


Abstract
There is pressure on primary care trusts, and therefore on GPs, to reach specific levels of use of low-cost statins as a proportion of total statin prescribing. This simple study looks at some markers of the quality of the results achieved. A correlation is found between a higher proportion of low-cost statin prescribing and lower achievement raising questions as to whether financial savings may be offset by poorer results.
- cholesterol
- hydroxymethylglutaryl-CoA reductase inhibitors
- Quality and Outcomes Framework
- quality indicators
- secondary prevention
- statins
INTRODUCTION
The National Institute for Health and Clinical Excellence (NICE) has recommended that statin (hydroxymethyl glutaryl [HMG]-CoA reductase inhibitor) therapy should usually be initiated with a drug with a low acquisition cost.1 The NHS Institute has taken this a step further in developing an ‘indicator’ for primary care trusts (PCTs). In its guidance NHS Better Care, Better Value, it defines a clinical productivity indicator, ‘increasing lower cost statin prescribing’ as a percentage of total statin prescribing that is for low cost statins (simvastatin and prevastatin).2 At the time of writing, it stated ‘if PCTs with below 77% (achieved by the top quartile of trusts) of lower cost statins increased this to 77% over £24 million would be saved in a year’.
Although the NHS Institute specifies that ‘these indicators are not targets’, PCTs have encouraged practices to switch patients to lower-cost statins. In Somerset the percentage of low-cost statins prescribed has been explicitly set as one of the prescribing targets for practices engaged in the practice-based commissioning enhanced service, with an expectation that 80% of all statin prescriptions should be for simvastatin or pravastatin, these being two statins with the lowest ‘acquisition costs’ in the UK.3
The lower-cost statins tend to be less powerful in lowering cholesterol levels.4 This simple study was therefore designed to assess whether there is a correlation between percentage use of low-cost statins and performance in managing cholesterol.
The Quality and Outcomes Framework (QOF), established as part of the national GP contract in the UK in 2004, analyses patient records to assess performance against a variety of clinical indicators. Two of these specifically look at management of cholesterol for secondary prevention.
‘CHD8’ counts the percentage of the practice patient population, with a history of ischaemic heart disease, whose most recent total cholesterol was below 5.0 mmol/l.
‘Stroke8’ counts the percentage of the practice patient population, with a history of cerebrovascular disease, whose most recent total cholesterol was below 5.0 mmol/l.
The study performed a simple analysis to compare the ‘performance’ of Somerset practices in achieving a high percentage of low-cost statin prescribing against their performance in these two QOF markers.
METHOD
Somerset PCT regularly sends to all their practices a ‘prescribing scorecard’ which details practices' performance against various prescribing indicators. One of these indicators is the amount of simvastatin and pravastatin prescribed as a percentage of total statin prescribing.
The website www.gpcontract.co.uk provides a detailed breakdown of performance of individual practices against each QOF marker. This includes the percentage achievement results achieved for CHD8 and Stroke8.
The statin prescribing data from the prescribing scorecard for April 2007 were compared with the performance in managing cholesterol as measured by the data for the QOF for the financial year 2006–2007.
RESULTS
Practice use of the ‘low acquisition cost’ statins, simvastatin and pravastatin, ranged from 33.6% to 93.6%, with a median of 72.0%. Practice achievement of CHD8 ranged from 36.4% to 98.1%, with a median of 82.7%. Practice achievement of Stroke8 ranged from 46.7% to 97.2%, with a median of 75.7%.
Figure 1 is a scatter graph showing the practices' performance on the statin prescribing scorecard plotted against achievement in cholesterol management in patients with coronary heart disease and cerebrovascular disease.
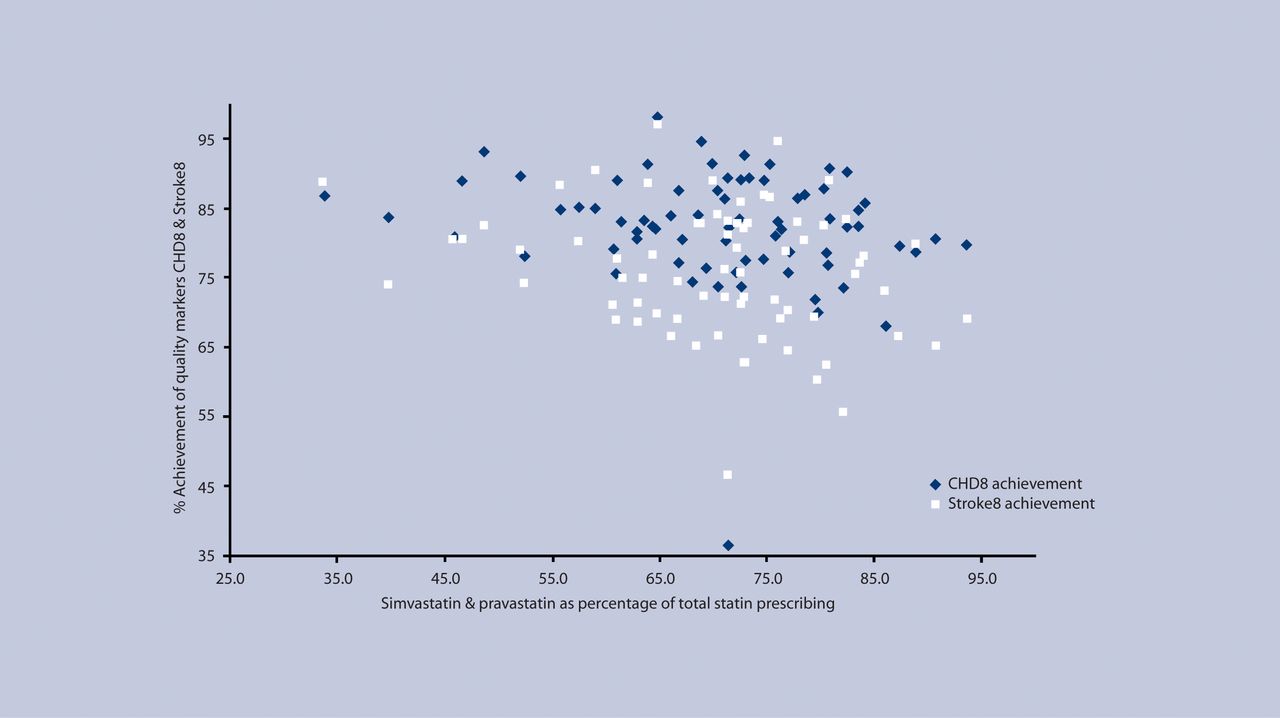
Achievement of cholesterol quality markers versus use of low-cost statins.
How this fits in
Statins have been demonstrated to be effective for secondary prevention of cardiovascular events and stroke. This study raises the concern that targets for practices to achieve high use of low-cost statins may be related to poorer achievement of cholesterol quality markers. There is a potential tension between the expectation to use cheaper medications and the drive to reach clinical targets.
There is one (very) outlier practice with very low achievement on coronary heart disease and stroke. Given the nature of the rest of the data and that this is the only obvious outlier, it was felt reasonable to omit this outlier and consider parametric (Pearson's) correlations. Using these methods, the correlation between statin choice and CHD8 achievement is –0.26, P = 0.028. Coincidentally, exactly the same correlation is found for Stroke8 achievement. The correlation is statistically significant by usual standards of <0.05 and therefore unlikely to have arisen by chance.
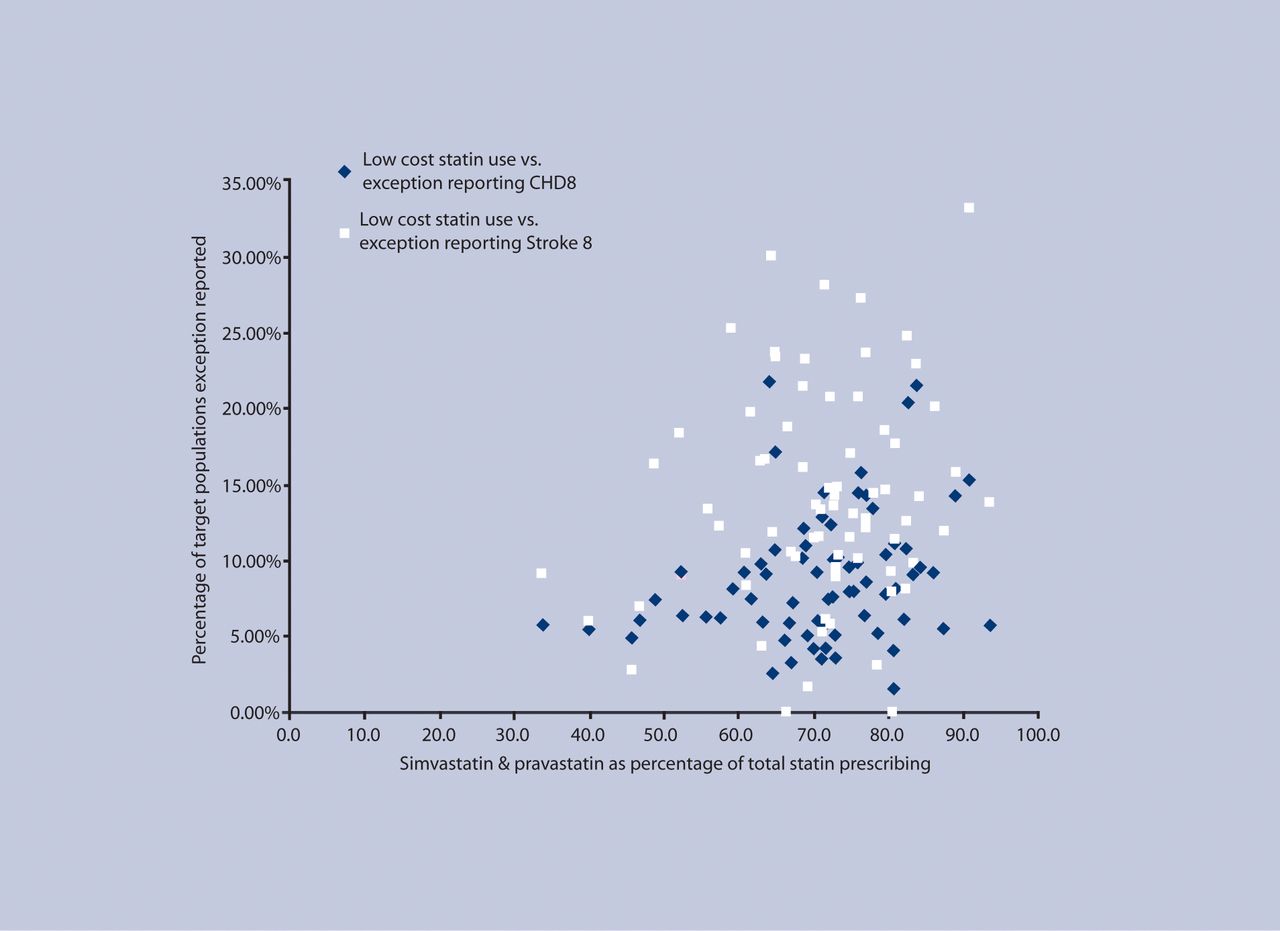
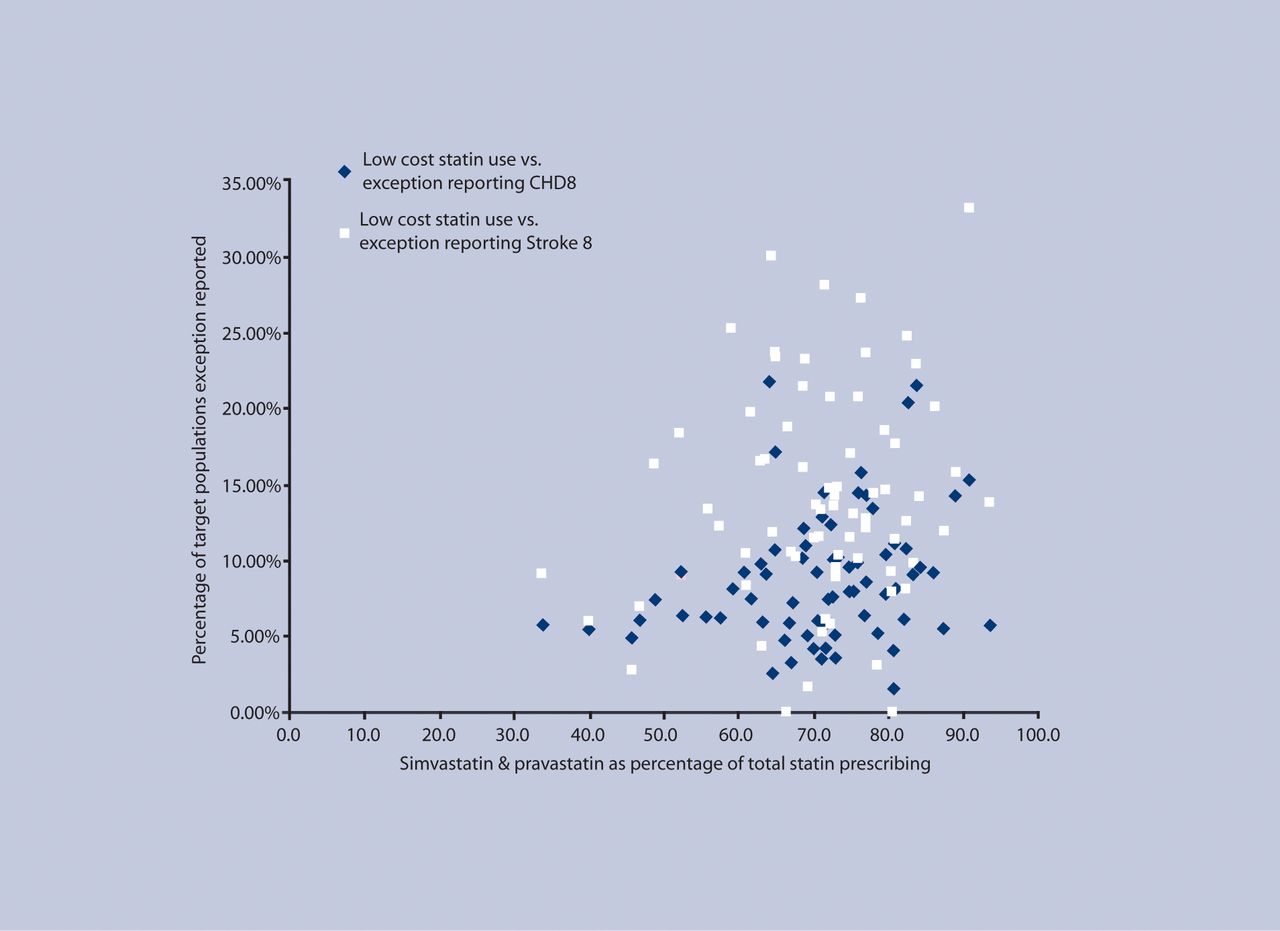
A key potential confounding factor regarding these data is the practice of exception reporting. Under the QOF rules, patients, who would otherwise be expected to fall within the denominator population, can be ‘exception reported’ for reasons such as intolerance of medication or being deemed as ‘unsuitable’ by their GP. The study therefore went on to use exception reporting data for the practices, obtained from the NHS Information Centre, to test whether there was a correlation with low- or high-cost statin prescribing. The data are presented in Figure 2.
{kind=link}
{kind=link}
Cholesterol quality marker exception reporting versus use of low-cost statins.
DISCUSSION
There does appear to be a correlation between an increasing proportion of ‘low-cost’ statin use and decreasing practice performance against the QOF indicators for secondary prevention.
In the light of the initial results, the study had considered whether practices with greater usage of more costly statins might also tend to have higher levels of exception reporting, making results easier to achieve. In fact the data, as shown in Figure 2, suggest that the converse is true with practices with greater use of ‘low acquisition cost’ statins tending to resort to higher exception reporting.
As the ‘low acquisition cost’ statins are defined as being simvastatin and pravastatin, the study also considered whether the variation in performance could be affected by which of these two statins practices tended to use. However, a review of data of relative simvastatin and pravastatin prescribing would appear to make this unlikely. Somerset as a whole has a very low prescribing rate of pravastatin. The number of items of pravastatin prescribed across Somerset for the year in question was only 2.66% of the total ‘low-cost’ statin prescriptions. For individual practices, the figure ranged from 0% to 23.95% but the median was 1.81%, with only three practices prescribing more than 10%.
There are other potential confounding factors that may independently affect a practice's achievement against QOF markers. Issues such as cardiovascular disease prevalence and deprivation may also affect a practice's statin use and performance, but this in itself may be an argument against applying blanket prescribing targets without considering such factors.
It would be of interest to look at those outliers who achieve good results with high proportional use of low-cost statins. It may be that some are making more use of additional therapy such as ezetimibe (as recommended by NICE) to augment treatment.5 With the cost of 28 days of ezetimibe being more than that of 20 mg daily of either atorvastatin or rosuvastatin, this may counteract the savings achieved.
The QOF markers are less stringent than the targets set by NICE in its most recent guidance, which recommends a maximum cholesterol target of 4 mmol/l for secondary prevention.6 It is possible that the achievement graphs might be steeper if the data were available to compare performance against these standards.
The results raise the concern that the pressure to prescribe low-cost statins may contribute to poorer control of cholesterol at the practice population level. Whether this has significant effects on mortality and morbidity is beyond the scope of this simple study, but NICE recommendations and QOF markers are based on the premise that tight control of cholesterol has significant benefits for secondary prevention. This de facto target for use of ‘low acquisition cost’ statins seems crude and does not allow for the characteristics of differing practice populations.
Acknowledgments
I would like to thank Dr Paul Ewings, Head of Research and Development at Taunton and Somerset NHS Trust for his advice and help with analysis of the data.
Notes
Ethics committee
Not applicable
Competing interests
The author is a Somerset dispensing GP whose practice has a 48.6% ‘low acquisition cost’ statin prescribing rate as at March 2009
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received February 27, 2009.
- Revision received April 17, 2009.
- Accepted June 1, 2009.
- © British Journal of General Practice, 2010.
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

