


Abstract
Background Policies suggest that primary care should be more involved in delivering cardiac rehabilitation. However, there is a lack of information about what is known in primary care regarding patients’ invitation or attendance.
Aim To determine, within primary care, how many patients are invited to and attend rehabilitation after myocardial infarction (MI), examine sociodemographic factors related to invitation, and compare quality of life between those who do and do not attend.
Design of study Review of primary care paper and computer records; cross-sectional questionnaire.
Setting Northern Ireland general practices (38); stratified sample, based on practice size and health board area.
Method Patients, identified from primary care records, 12–16?weeks after a confirmed diagnosis of MI, were posted questionnaires, including a validated MacNew post-MI quality-of-life questionnaire. Practices returned anonymised data for non-responders.
Results Information about rehabilitation was available for 332 of the 432 patients identified (76.9%): 162 (37.5%) returned questionnaires. Of the total sample, 54.4% (235/432) were invited and 37.0% (160/432) attended; of those invited, 68.1% (160/235) attended. Invited patients were younger than those not invited (mean age 63?years [standard deviation ﹛SD﹜ 16] versus 68.5?years [SD 16]); mean difference 5.5?years (95% confidence interval [CI] = 1.7 to 9.3). Among questionnaire responders, those who attended were younger and reported better emotional, physical, and social functioning than non-attenders (P = 0.01; mean differences 0.44 (95% CI = 0.11 to 0.77), 0.48 (95% CI = 0.10 to 0.85) and 0.54 (95% CI = 0.15 to 0.94) respectively).
Conclusion Innovative strategies are needed to improve cardiac rehabilitation uptake, integration of hospital and primary care services, and healthcare professionals’ awareness of patients’ potential for health gain after MI.
INTRODUCTION
The importance of cardiac rehabilitation has been established,1 yet many potentially eligible patients with coronary heart disease (CHD) do not attend.2,3 Recent guidelines identify rehabilitation as an essential component in patients’ care following myocardial infarction (MI) and emphasise that integrated service provision is needed, recommending that rehabilitation plans should be included in every patient's hospital discharge summary.4 Primary care is attributed a key role in managing patients with CHD,5 but little information is available about what is known in primary care about their rehabilitation invitation and attendance.
Most rehabilitation programmes are provided from a hospital base, but evidence that home-based programmes produce similar outcomes is increasing.6,7 Inadequate funding,2,8,9 and acknowledgement that many patients prefer home-based programmes,10 indicate a need for more active primary care involvement in service delivery. Information about referral and the sociodemographic characteristics and quality of life of individuals who are not invited to current rehabilitation services is incomplete.2
How this fits in
Cardiac rehabilitation is a cost-effective treatment but many potentially eligible patients do not attend. Primary care is identified as having a key role in improving uptake, yet little is known regarding its knowledge of patients’ invitation and attendance. Information relating to rehabilitation was found in primary care for 77% of patients after myocardial infarction and indicated that 37% attended: those who attended were younger, with a better quality of life. Innovative strategies are needed to improve systems integrating hospital and primary care services and to maximise patients’ potential for health gain.
This study aimed to determine, from within primary care, how many patients, after a MI, are invited to and attend rehabilitation, to examine sociodemographic characteristics associated with invitation, and to compare quality of life between those who do and do not attend.
METHOD
Participants
Based on geographical location (health board area) and practice size, a stratified sample of 38 general practices in Northern Ireland (NI) was identified. Their combined list (236 430) had age and sex distributions similar to the NI population: 49.7% were males (117?393/236?430). Practices used a prespecified computer search strategy to identify patients with MI or acute coronary syndrome, and repeated this every 2?weeks (May 2005 to February 2007). Both diagnoses were included because pilot work identified inconsistencies between cardiologists in attributing these diagnoses.11 Patients with recorded evidence of electrocardiogram changes or cardiac biomarkers supporting the diagnosis of an acute event 12–16?weeks previously were invited to participate.
Data collection
Potential participants were posted questionnaires and a reply slip indicating consent for researchers to access their medical records. Data collected related to sociodemographic information, rehabilitation invitation and attendance, reasons for non-attendance, comorbidities, and quality of life (validated MacNew post-MI questionnaire).12
Non-responders were telephoned after 2?weeks, reminded of the invitation, and asked about rehabilitation invitation and attendance. If no contact was made, staff searched paper and computer records and returned anonymous data regarding rehabilitation, age, sex, and postcode, from which measures of socioeconomic status were derived (Multiple Deprivation Measure [MDM]: higher values indicate less deprivation). If no information was found, records were searched up to 6?months later.
Statistical analysis
It was estimated that 76 in each group would allow detection of a 10% difference between attenders and non-attenders in physical, emotional, and social functioning quality-of-life scores with 0.05 α and 80% power. This was derived from piloting the MacNew post-MI questionnaire in 30 patients and finding that 0.41 (relating to physical functioning) was the smallest difference observed between attenders and non-attenders. The study population was chosen to allow recruitment of 160 MI survivors within the study period, estimating 0.2% annual MI incidence, 50% survival, and 40% response rate.
Using SPSS (version 14.0), categorical data were compared between those who were and were not invited, and between those who did and did not attend, using χ2 tests; deprivation scores were compared by Mann–Whitney tests, and quality-of-life measures by t tests.
RESULTS
Demography of sample
Of 432 individuals identified, invitation data were obtained for 332 (76.9%) and attendance data for 330 (76.4%); 37.5% (162/432) responded to the questionnaire. Questionnaire responders and non-responders did not differ significantly in mean age (63.6?years [standard deviation ﹛SD﹜ 18.5, versus 66.3 [SD 13.7]), sex distribution (75.3% male [122/162] versus 70.0% [189/270]), or deprivation (median MDM 414.5 versus 364.0).
Invitation
Data indicated that, overall, 54.4% (235/432) were invited to rehabilitation, 22.5% (97/432) were not: no information was available for 23.1% (100/432) (Figure 1). Among those with invitation data, 70.8% (235/332) were invited: those invited were younger than those who were not (Table 1) but their sex distribution and socioeconomic status were similar. Questionnaire responses showed that the odds of retired people being invited were less, compared to those who were not retired (Table 2).

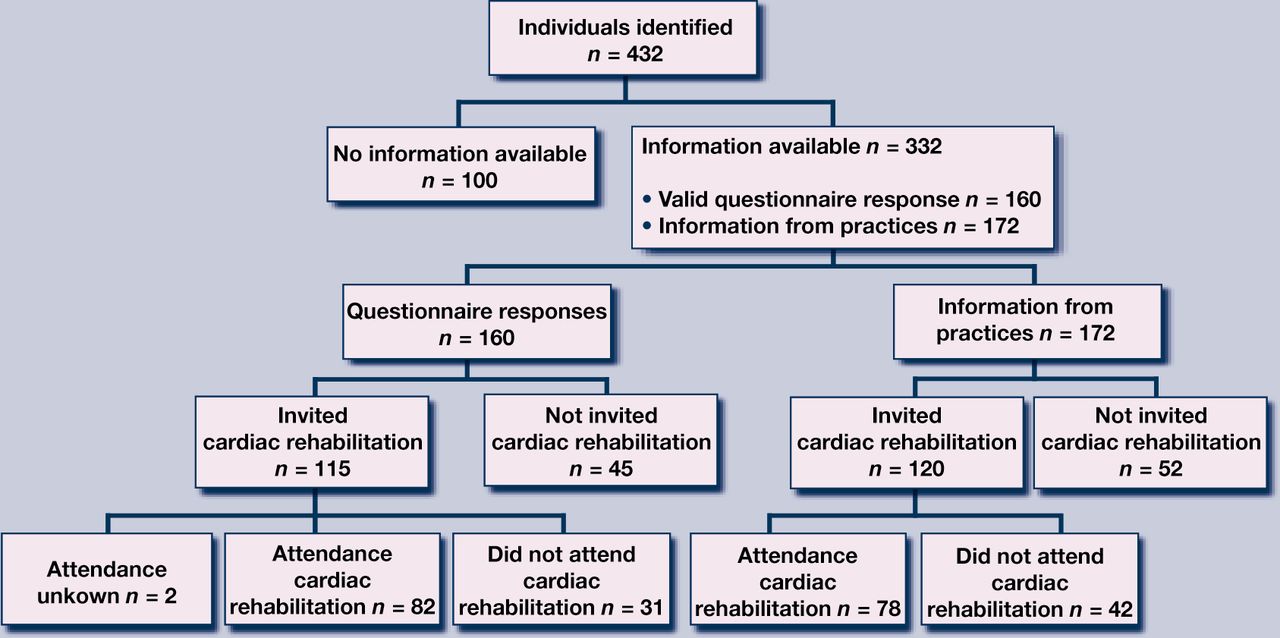{kind=link}
Flow of participants through the study.
Demographic characteristics of post-MI patients with cardiac rehabilitation invitation and attendance information (combined questionnaire and anonymous data).
Comparison of social, health and quality of life characteristics of questionnaire responders in relation to cardiac rehabilitation invitation and attendance.
Attendance
Overall, data indicated that 37.0% attended (160/432) but no attendance information was available for 102 (23.6%). Comparing ‘attenders’ with ‘non-attenders’ (including those not invited), showed that attenders were younger (Table 1). Of those invited, 68.1% (160/235) attended.
Among questionnaire responders who were invited, 71.3% (82/115) attended (Table 2). Home owners were more likely to attend than non-home owners but no other sociodemographic differences were found.
Further analysis, involving invited participants only, showed attenders’ deprivation score was higher than non-attenders’ (median 426.5 versus 250.5, P = 0.04).
Quality of life
Comparing those who attended with those who did not, including those who were not invited, showed that attenders had better emotional, physical, and social functioning, reflecting a better quality of life (Table 2).
DISCUSSION
Summary of main findings
This study found that no information about cardiac rehabilitation after MI was held in primary care for 23% of patients. Overall, data indicated that 37% attended: 54% were invited and two-thirds of these attended, but older patients were less likely to be invited and attend. Those who attended had a better quality of life.
Strengths and limitations of the study
The study findings have external validity: participants were similar to non-participants in terms of age, sex, and socioeconomic status and the participating practices were representative of the general practices in Northern Ireland. Every participant's primary care record contained a hospital discharge summary confirming their diagnosis, all NI hospitals contributed to management of some participants, and ample time was allowed for information transfer between services.
Absence of information relating to cardiac rehabilitation is likely to reflect non-invitation and non-attendance. It is recognised that the accuracy of all self-reported information was not checked. However, a quality check was performed on a random 10% sample of the questionnaire data and this indicated that the variation between self-reported and recorded information was small.
Comparison with existing literature
Previous studies found that younger, male,13,14 and married14 individuals were more likely to be invited to rehabilitation. However, no evidence was found in this study of invitation bias relating to sex or marital status. The study finding that 68% of those invited attended compares with recent audit data that approximately 77% of invited patients attend.2
A recent Canadian study reported that less than half of primary care physicians received information about patients’ progress in cardiac rehabilitation.15 The present study has also identified a communication gap between services. While this study preceded the launch of regional guidelines,16 anecdotes suggest that physicians in both primary care and hospital could attribute more importance to rehabilitation. Research indicates that patients who perceive their physician considers rehabilitation important are more likely to attend.17,18
Implications for clinical practice and future research
Previous trials reporting benefits of cardiac rehabilitation for quality of life showed small effect sizes, with varied outcome measures and methodological quality.19,20 The present finding of better quality of life among attenders may suggest that those with better quality of life are more likely to attend but may also indicate that benefit is derived from attendance. Regular reviews,21,22 and other organisational changes in general practice,23 have led to improved provision of secondary prevention. However, this is not necessarily associated with better quality of life.24 There is a need for more holistic care of patients following MI.
Strategies are needed to address gaps in systems, communications, and coordination of services. The responsibility for developing these must be shared between hospital and primary care. Further exploration of strategies to engage professionals and patients in rehabilitation and translate policy into practice is warranted, to minimise gaps in service provision and maximise patients’ potential for health.
Acknowledgments
We wish to thank all participating practices, their staff, and patients who contributed to the data collection, and Professor Ian Young, Dr Gavin Dalzell, Dr Barry Kelly, and Dr Noleen McCorry for their help and advice.
Notes
Funding body
The research was funded by the Research and Development Office (Northern Ireland). Margaret E Cupples and Mark A Tully are co-funded by the Centre of Excellence for Public Health (Northern Ireland), a UKCRC Public Health Research Centre of Excellence. Funding from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, Research and Development Office for the Northern Ireland Health and Social Services, and the Wellcome Trust, under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged.
Ethics committee
Queen's University Belfast Ethics Committee gave the study ethical approval (Ref No. 362/03, November 2003).
Competing interests
The authors have stated that there are none.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received August 24, 2009.
- Revision received October 26, 2009.
- Accepted January 7, 2010.
- © British Journal of General Practice, 2010.
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

