


Article Figures & Data
Figures
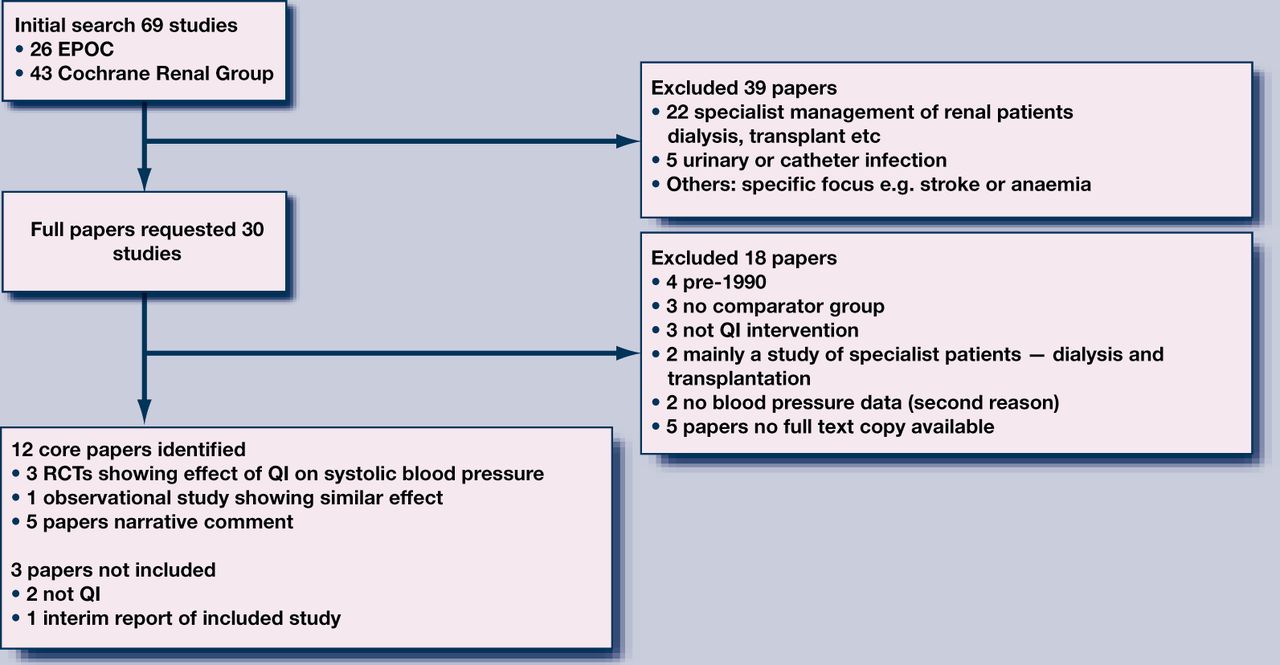
- Figure 1
Selection of core articles.
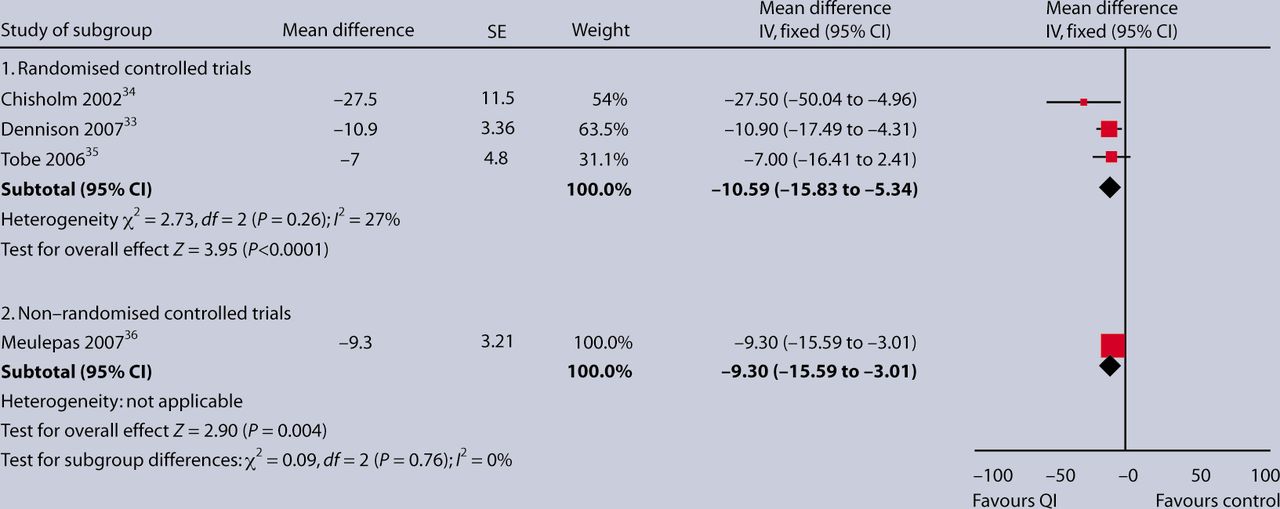
- Figure 2
Mean reduction in systolic blood pressure in three randomised and one non-randomised study of quality-improved interventions.

{kind=link}
{kind=link}
Tables
- Table 1
Controlled trials and an observational study of QI interventions to lower systolic blood pressure.
Brief reference Sample Type of study Intervention Outcome Notes on inclusion Randomised studies Chisholm MA, et al. Effect of clinical pharmacy services. Ethn Dis 2002; 12(3): 392–397.34 n = 13 intervention; n = 10 control RCT into receiving a pharmacy-based intervention compared with usual post-transplant care A clinical pharmacist performing medication reviews Patients in intervention group had a mean systolic blood pressure change at 12 months of –5 versus +18 mmHg in control Although transplant patients, they were well in the community and their kidneys were responsive to therapy, as in CKD Dennison CR, et al. Urban African-American men. Am J Hypertens 2007; 20(2): 164–171.33 n = 157 more intensive; n = 153 less intensive 5-year randomised trial of more- versus less-intensive care for hypertensive men Nurse-led educational, behavioural, and pharmacological intervention. More- intensive intervention involved education, individualised multidisciplinary care with nurse practitioner visits as needed every 2–3 months, annual home visits, engagement of social support, and adjustment of antihypertensive regime. Less-intensive intervention comprised education and provision of a list of community hypertension care sources The mean serum creatinine in the more- and less-intensive groups was 1.27 and 1.29 ?mg/dl; 36% and 45% respectively had microalbuminuria. Data include change in systolic and diastolic blood pressure (annually for 5 years); and proportion with blood pressure <140/90 mmHg (annually for 5 years) Results are likely to indicate slowing progression in CKD: increased proportions remaining free of 50% rise in creatinine or remaining free of increase in proteinuria during follow-up in intervention limb. Possible difference due to use of angiotensin-converting enzyme inhibitor Tobe SW, et al. Nurse-directed hypertension treatment. CMAJ 2006; 174(9): 1267–1271.35 n = 50 intervention; n = 49 control RCT of two community-based strategies for controlling hypertension in First Nations people with type 2 diabetes Home nurse following a hypertension and diabetes protocol compared with usual practice. In the intervention limb, the patient's drug regimen was titrated according to predefined management algorithm, utilising a stepwise approach to lower blood pressure to a target of <130/80 mmHg The primary outcome measure was difference in systolic blood pressure between the two groups after 12 months. At 12 months versus baseline, systolic blood pressure fell by 24.0 ± 13.5 mmHg in the intervention group and by 17.0 ± 18.6 mmHg in the usual practice group. Data on change in diastolic proteinuria are also reported Although severe renal impairment (serum creatinine >250 µmol/l) were excluded, mean serum creatinine in the intervention limb was 73 ± 16 µmol/l, and the population had significant proteinuria (albumin/creatinine ratio 25 ± 72 mg/mmol Non-randomised study Meulepas MA, et al. Logistis support of diabetes. Fam Pract 2007; 24(1): 20–25.36 n = 353 intervention (51 GPs); n = 129 control (21 GPs) Controlled non-randomised study. The study was based in the Netherlands. The GPs were the primary research subjects Introduction of a diabetes support service (DSS) to facilitate implementation of guidelines for management of type 2 diabetes in primary care. The DSS called up patients for laboratory testing, foot examination, fundus photography, and appointments with dietician and diabetes nurse. The DSS did not provide patient care itself 2 years post introduction of the DSS, the difference in the change in systolic blood pressure (from 1 year prior to intervention to 2 years post) was –9.3 (–3.0 to –15.6) mmHg in intervention group compared with control. Data on change in diastolic blood pressure, and proportions meeting blood pressure targets (150/85 mmHg) are also reported No direct measures of renal function were available. Study is included as a high proportion of individuals with type 2 diabetes will have CKD - Table 2
Narrative summary of other studies considered in depth but not contributing quantitative data.
Brief reference Sample Type of study Intervention Outcome Notes on inclusion Binik YM, et al. Live and learn. J Nerv Ment Dis 1993; 181: 371–376.37 n = 87 intervention; n = 92 standard education; n = 25 ‘not part of education’ A randomised study on 204 patients with advanced CKD (not yet on renal replacement) Enhanced or standard educational package predominantly nurse delivered. Education was directed towards preparation for dialysis, and involved an individually administered slide presentation and booklet A rising creatinine of >350 µmol/l was required inclusion. The setting was nephrology clinics in Canada. Those that received the enhanced and standard packages started dialysis after 14.9 ± 12.4 and 10.3 ± 11.8 months respectively Did not include blood pressure, so could not be included with the other quantitative analysis Jaber LA, et al. Pharmaceutical care. Ann Pharmacother 1996; 30(3): 238–243.38 n = 17 intervention; n = 22 control A randomised controlled study in diabetes (n = 532, predominantly older black females with type 2 diabetes) Patient and physician education by a pharmacist. Education was provided on diabetes, medications, diet, exercise, glucose monitoring, and self-adjustment of hypoglycaemic regimes Improvements in glycated haemoglobin found. No improvement in blood pressure or renal function No direct measures of renal function were available, mean creatinine was 88 µmol/l. No usable data (baseline and post-intervention blood pressure reported but no standard error) Mazzuca SA, et al. Diabetes education study. Diabetes Care 1986; 9(1): 1–10.39 n = 125, 134, and 138 for intervention groups; n = 135 control Random allocation into a factorial design of control, patient, physician, or patient and physician intervention groups. Subjects predominantly black older females with type 2 diabetes Intensive patient education, which was formalised and didactic, providing a systematic programme of diabetes education and delivered by a specialist multidisciplinary team; physician education from an expert; or both Reduction in fasting glucose and glycated haemoglobin No direct measures of renal function were available, mean creatinine 88 µmol/l. No usable data (baseline and post-intervention blood pressure reported but no standard error) McGhee SM, et al. Coordinating and standardizing long-term care. Br J Gen Pract 1994; 44(387): 441–445.29 n = 277 outpatient care; n = 277 shared care; n = 277 nurse practitioner care Randomised controlled trial Compares different types of care: either standard outpatient care or shared general practice-hospital care, whereby a hospital-based database generates an annual record on each enrolled patient for the GP and a patient-held record for the patient, including a prompt to attend for a review with the GP; overall responsibility for the patient's care lies with the GP, and the outcomes of the review are returned to the registry so further specialist recommendations can be made where appropriate Process measures of review and wish to continue with care offered Did not include blood pressure results or other indication that patients had CKD New JP, et al. Measuring clinical performance. Diabetologia 2000; 43(7): 836–843.40 n = 6544 patients with diabetes Observational study Before and after effect of introducing an information system All categories of monitoring improved Comparison of non-contemporaneous groups makes linking cause and effect difficult
In this issue

British Journal of General Practice
Quality-improvement strategies for the management of hypertension in chronic kidney disease in primary care: a systematic review








Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...
Intended for Healthcare Professionals

