


Article Figures & Data
Figures
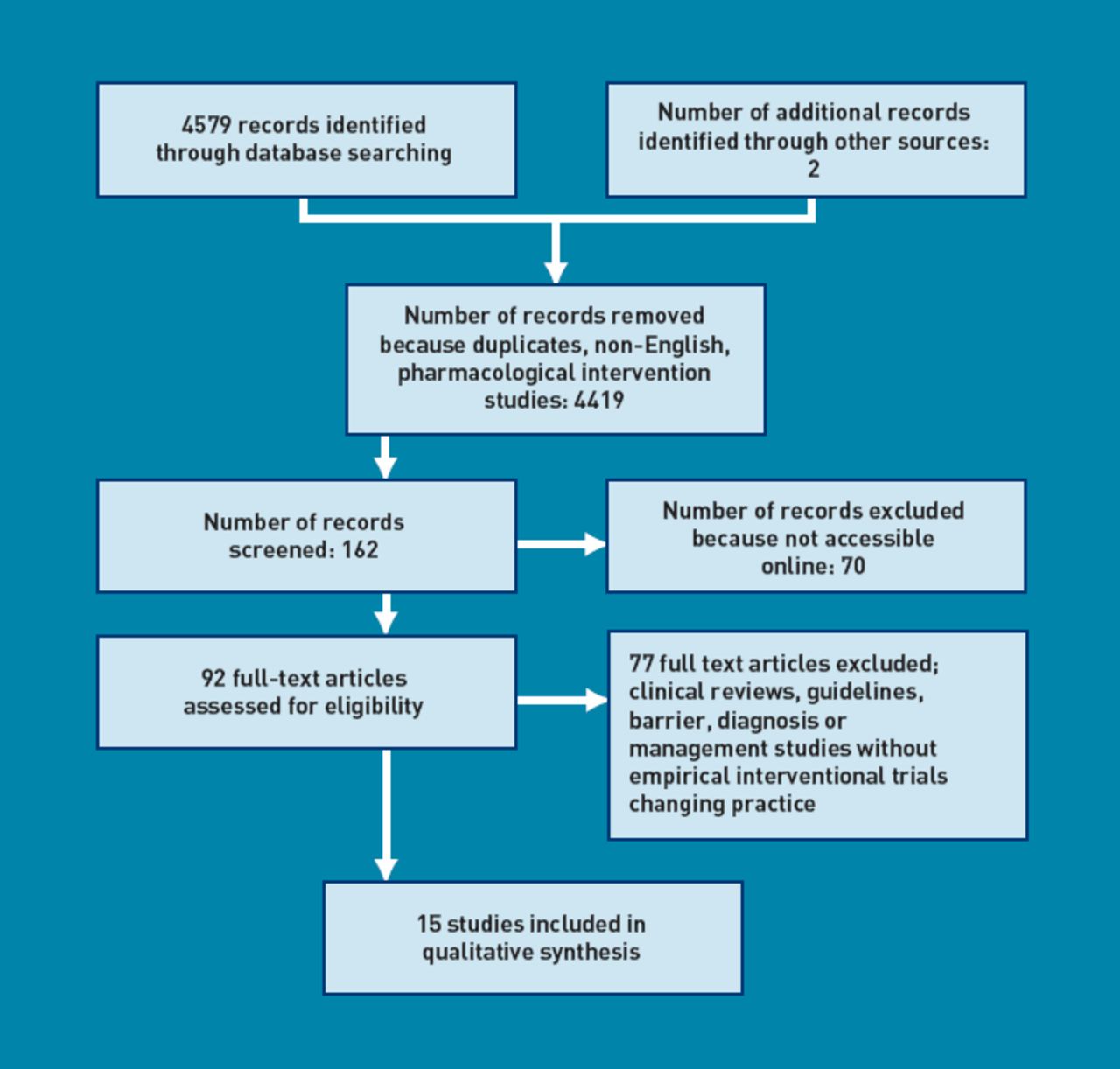
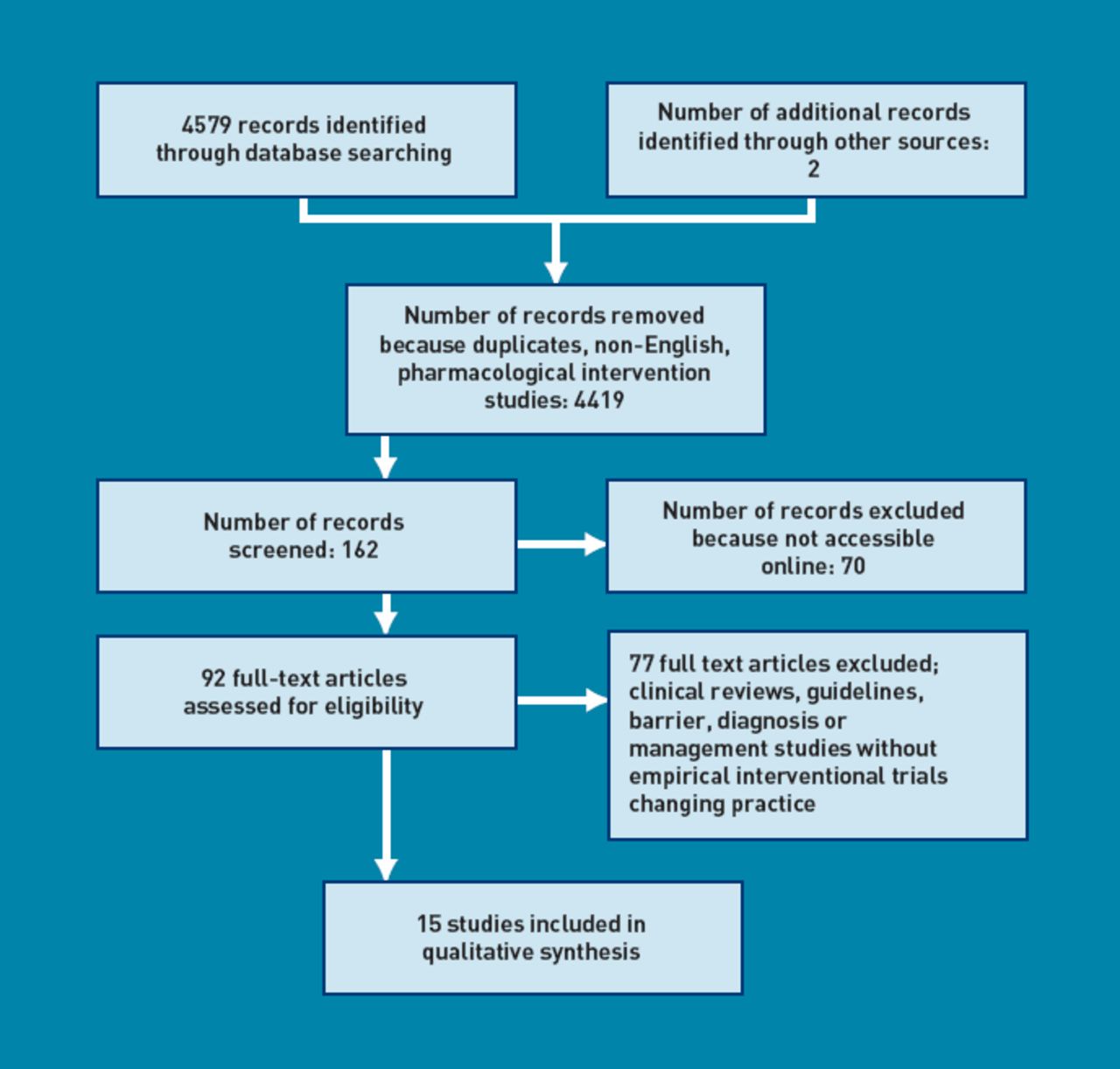
- Figure 1
PRISMA flowchart
{kind=link}
Tables
Authors, date and country Size Recruitment Intervention Method Outcomes Results Conclusions Waldorff etal 2003;14 Denmark 413 GPs in intervention, 122 in control group GPs identified from medical association and organisational database Assessment of a multifaceted strategy to implement guidelines Controlled before and after study Included dementia screening, thyroid function and vitamin B12 tests, cognitive testing and referrals to specialists; also questionnaire examining acceptability of guidelines No significant difference between control and intervention group was found in the number of diagnostic evaluations undertaken, the number of ordered, orthe amount of cognitive testing performed. Most GPs had read the guidelines and found them applicable Aftera multifaceted strategy for implementation, there was no improvement in the adherence to a guideline for diagnosing dementia. However, the outcomes were measured only 4-7 months after implementation, and while the intervention was delivered at GP level, the outcomes were measured at practice level Downs etal 2006;16 central Scotland and London 35 practices Local group meetings, postaland phone invitations, practice visits Threearms: (1) tutorial on CD-ROM, (2) decision-support software, (3) practice-based workshops Unblinded, cluster randomised before and after controlled trial Detection rates. Concordance with guidelines Significant increase in the detection of dementia inarms 2 and 3. No improvement in adherence to guidelines Might be useful to examine potential cumulative effects of combining educational interventions Rondeau etal 2008;19 France 684 GPs, 214 specialists, 3021 patients Random selection from a list of GPs throughout France Group educational meeting, and training in use of neuro psychological tests Cluster randomised controlled trial Primary outcome: suspicion of dementia by GP. Secondary outcome: diagnosis of dementia by GP No difference in diagnosis of dementia in intervention group Education ineffective Chodosh etal 2006;18 US 166 primary care clinics Questionnaires sent to all primary care health providers at 16 clinics Survey of knowledge, attitudes, perceptions following participation in the ACCESS study (Vickreyet al24) Survey following a cluster randomised controlled trial of a care management intervention Practitioners' knowledge about capacity determination, evaluation, treatment and patient safety. Measures of attitude, and perceptions of quality of care Intervention group knew more about determining capacity and more felt that management of dementia patients in primary care was difficult; no other difference in knowledge, attitudes or perceptions of quality of care Care management programmes may have a positive effect on care despite lack of educational gain Wenger et al 2009;1 US 357 intervention and 287 control community-dwelling patients Patients aged >75 years, with difficulty in falls, continence or cognition; two medical groups participated each having two sites, with one acting as a control and one as an intervention site Patients' problems were identified bya telephone call, then the physician triggered a condition-specific process of management and resulted with formulating a plan for the patient. Physicians in the intervention group had a 3-hour educational session on Assessing Care of Vulnerable Elders (ACOVE) quality indicators. Patients also completed questionnaires. Data were collected from medical records. Patients also completed questionnaires. Data were collected from medical records Controlled trial Percentage of quality indicators met after 13 months of medical record extraction For cognitive impairment, care as triggered by quality indicators did not differ; however, more attention was given to caregiver education, decision-making capacity, and discussion about driving occurred in the intervention group Care did not improve for patients with cognitive impairment. All physicians provided more recommended care for patients who presented with their symptoms (compared to those identified by screening) Vollmar et al 2010;20 Germany 389 GPs from 26 Quality Circles (QCs) All QCs within a 50km radius of Witten University were contacted by telephone or letter to the QC moderator. GPs were recruited at QC meetings, and required to participate in an extra session and have access to the internet. A control group was used for comparison QCs were randomly allocated to either arm of the trial: online learning + structured case discussion (‘blended learning’) or lecture + structured case discussion. Both groups received pocketbooks of the guidelines. Control group received only the pocketbook. Knowledge tests were carried out pre-and post- intervention, and at 6 months Cluster randomised controlled trial Primary outcome: knowledge gain from before to afterthe intervention. Secondary outcome: comparison of knowledge gain of the two groups. Both groups showed a significant gain in knowledge following the interventions. However, there was no difference in knowledge gains between the two groups Sub-group analysis showed that GPs who self-reported using the online learning had significant knowledge gain compared with theothergroup. The control group showed a knowledge gain that was significantly less than the intervention groups Blended learning’ was not more effective than traditional learning in improving dementia knowledge in GPs. However, when GPs self-report use of online modules, results suggest that blended learning techniques could be more effective Perry et al 2008;13 Holland 151 patients 54 GPs recruited patients >70 years into Dutch EASYcare study Geriatric Intervention Program (DGIP) Secondary analysis of data examining whether the DGIP (an in-home assessment) improves rates of detection of dementia in primary care. In-home assessment performed by specialist nurse, assessed function, mood, cognition, caregiver burden. A management plan was formulated Blinded, randomised controlled trial Primary outcome: the number of new dementia diagnoses. Secondary outcome: the level of under-registration of dementia cases The number of dementia diagnoses in control group (9%) was significantly less than those in intervention group (29%) (P= 0.02) An in-home assessment and management programme is effective in detecting dementia in the primary care setting compared with controls of usual care Callahan etal 2006 ;26 US 153 patients with Alzheimer's disease Primary care centres Collaborative care management Randomised controlled trial Neuro psychiatric inventory (NPI) cognitive function, carerstress, service use Intervention group had lower NPI scores but no difference in depression, cognitive status, or functional scores. Carers showed less stress. Intervention group had higher number of contact visits with physician/nurse, but no difference in hospital or nursing home admissions Collaborative care can reduce behavioural/psychological symptoms in patients, and stress in carers Vickrey etal 2006;24 US 408 patient and care-giver dyads from 18 clinics Patients identified from organisational database Dementia care manager with web-based support software for care planning, and coordination. Interactive educational seminars for practitioners in intervention group Cluster randomised controlled trial Primary: adherence to guidelines. Secondary: use of cholinesterase inhibitors, patient quality of life (QoL), caregivers knowledge. QoL, social support and confidence Intervention group care more adherent to guidelines and got more community services, were prescribed more cholinesterase inhibitors. Caregivers were more confident in intervention group Systems change by introducing care managers can improve quality of care, but is costly Fortinsky etal;27 2009 US 84-caregivers Family caregivers of patients with dementia were recruited from the Alzheimer's Association, and primary care Intervention group received educational materials which were discussed with a dementia care consultant Cluster randomised trial Primary outcome: admission to a nursing home in the study period. Secondary outcomes: caregiverself-efficacy, caregiver burden, depression, health, satisfaction with the service Intervention group were 40% less likely to end up in nursing home than control, but this did not achieve statistical significance No difference was found between groups for secondary outcomes. Inadequately powered study Clark etal 2004 ;25 US 89 participants with a symptom of memory loss or diagnosis of dementia, but no mention of how many in control and how many in intervention groups Patients registered with Kaiserwith diagnosis of dementia on medical records or symptoms indicative of cognitive impairment Intervention group received care-consultation: telephone interaction between Alzheimer's Association staff and patient/caregiver Randomised controlled trial Hospital admissions A&E visits, number of physician contacts satisfaction with service, depression, strain on patient Intervention group reported more memory symptoms, but were less likely to have hospital admissions or A&E visits, and had fewer physician contacts. Also experienced less embarrassment, isolation and relationship strain Overall, patients who had a care consultant had lower levels of negative consequences from memory problems, and reduced usage of certain services Trial Description of intervention Waldorff et al 2003;14 Local GPs and specialists collaborated in the design of the multifaceted strategy. Interventions included: 1. Seminars on specific clinical practice guidelines and screening tools, brain imaging as a diagnostic procedure, and pharmaceutical treatments for dementia 2. Three reminder letters covering the main recommendations in the clinical practice guidelines 3. An individualised small-group educational programme 4. Outreach visits by a trained GP facilitator, who underwent a 5-hour symposium of training. Downs et al 2006;16 Three interventions trialled: 1. Decision-support software was written inside medical electronic records and used prompts for the investigation and management of dementia. Assisted clinical reasoning and planning in real time. 2. CD-ROM — electronic tutorial using case analysis, reflections on knowledge, and considering complex clinical problems. Designed as electronic book’ format using indexing and hypertext links 3. GPs with experience in postgraduate education facilitated small-group workshop using clinical scenarios and case discussions in multidisciplinary groups. Rondeau et al 2008;19 Training on a battery of cognitive screening tests (the Short Cognitive Evaluation Battery, Robert et al 200346) which tests four cognitive areas which are often impaired in Alzheimer's disease (with a sensitivity of 93.8%) 2-hour group educational meetings on Alzheimer's disease and otherforms of dementia. Chodosh et al 2006;18 Intervention participants were offered five educational modules comprising a total of 100 minutes of presentation and discussion in small-group format (and available on the web). These were: 1. Assessment of capacity for making medical decisions 2. An overview of the dementia care management programme 3. The role of care managers 4. The recognition and treatment of dementia and depression 5. The recognition and treatment of dementia and delirium The survey instrument measured different facets of understanding: Five multiple choice questions (MCQ) addressing knowledge base on capacity, delirium, patient safety, and depression three MCQs on perceived value of screening, value of dementia care, and perceived difficulty in management. Also questioned on perceived quality of resources and ability to coordinate care, and value of correspondence from other providers. Wenger etal 2009;17 Educational sessions for practitioners and structured prompts on management and care for patients. For positively screened patients a prompt initiated collection of specific data, triggered recommendations of specific investigations, and suggested specific care processes. The prompt supported the facilitation of an impression and plan forthe patient, and included decision-support materials and patient education resources and information about local services. 3-hour educational session learning an efficient approach’ to the condition, using Assessing Care of Vulnerable Elders (ACOVE) quality indicators (ACOVE investigators 200147). After piloting practices met to share experiences of clinicians and to modify the structure of the intervention as necessary. Clinicians/practices were able to review and adapt the prompts to suit their local services and personnel. Vollmar etal 2010;20 Two interventions: 1. Online learning modules + structured case discussion. Online modules covered: the guideline. Interactive case stories relating to guidelines. 2. Lecture + structured case discussion. Lecture covered: 30 minutes slide presentation, on dementia-related training. Structured case discussion was 45 minutes. Participants in both groups completed knowledge test pre- and post-intervention, and at 6 months, as well as an evaluation form. The knowledge test comprised 10 MCQs on diagnosis and 10 MCQs on management of dementia. All participants received printed pocketbook of the guidelines. A control group received the printed pocketbook of the guidelines only. Perry et al 2008;13 GPs referred patients to the study who were then randomised to control or intervention. Geriatric Specialist Nurse visited patients at home for assessment using the EASYcare instrument (Richardson 200128). This tool assesses activities of daily living, mood, cognition and has goal-setting elements. This was followed by up to 6 visits in 3 months for management planning. The nurse, primary care physician, and geriatrician met regularly to discuss cases. Callahan et al 2006;26 Collaborative care management by the primary care physician and a geriatric nurse practitioner, for 12 months. All patient contacts were with the nurse. All intervention patients recommended for anticholinesterase inhibitors. Assessments on patient's behaviour and memory were made regularly and management planned accordingly. Primary care physicians were consulted to prescribe medications to help if non-pharmacological interventions hadn't been successful. Caregiver and patient education given, as well as regular psychological support for both caregiver and patient. Weekly meetings with multidisciplinary teams who reviewed care and adherence to guidelines. Support given by web-based system which helped with monitoring and multidisciplinary communication. Vickrey et al 2006;24 Twenty-three guideline recommendations identified (by a multidisciplinary group) as care goals. The same group designed an assessment and protocols, and organised care-coordination. Care managers (mainly social workers) were trained, and carried out the assessments. Follow-up was arranged based on need but regular 6-monthly format assessments were carried out. Assessments were made, software assisted in providing a care plan, and recommendations to primary care physician were made. The software also facilitated multidisciplinary communication, and referrals to other agencies. Up to five interactive seminars' of 90 minutes were offered to primary care physicians, educating on issues such as behaviour changes, determining capacity, and depression. Fortinsky et al 2009;27 Care consultant initiated monthly contacts with patient and caregiver over 12 months. Educational material for caregivers was given to intervention and control groups, including information about the course of disease, legal/financial issues, and community services. The intervention group was able to discuss these with the care consultants. Contacts were used to assess symptoms and concerns, and compose action plans for caregivers. The agenda was set by the caregiver. Primary care physicians were faxed care plans with the hope that they would discuss/review with caregiver and patient during consultations. Clark et al 2004;25 Care consultation offered by Alzheimer's Association specially-trained staff. The care consultants conducted structured assessments and developed care strategies using family and community resources. These might include education/training programs or support groups. Regular follow ups arranged initially bi-weekly then monthly or 3-monthly. - Table 3
APEDro (Physiotherapy Evidence Database) scale evaluation of studies in the review
Waldorff et al 200314 Downs et al 200616 Rondeau et al 200819 Chodosh et al 200618 Wenger etal 200917 Vollmar et al 201020 Perry et al 200813 Callahan et al 200626 Vickrey et al 200624 Fortinsky et al 200927 Clarke et al 200425 Study Design Controlled before and after study Cluster randomised triala Cluster RCT Cluster RCT Controlled trial Cluster RCT RCT RCT Cluster RCT Cluster RCT RCT Eligibility criteria were specified No No Yes Yes Yes Yes Yes Yes Yes Yes Yes Random allocation to intervention No Yes Yes Yes No Yes Yes Yes Yes Yes Yes Allocation concealed No Yes No Yes No Yes No Yes Yes Yes Yes Intervention groups similar at baseline Nob Yes Yes Yes Yes Nod Yes Yes Yes Noc Yes Blinding of all participants No No No No No No No Yes No No No Blinding of all therapists No No No No No No No No No No Yes Blinding of all assessors No No No No No No No Yes No Partial No Measures of at least 1 outcome obtained from >85% of participants Yes No Yes Yes Yes No Yes Yes Yes Yes Yes Intention to treat analysis Yes Yes No Yes No No No No Yes No No Results of between interventions group statistical comparisons are reported for at least 1 outcome Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Study provides both point measures and measures of variability for at least 1 key outcome Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes TOTAL (maximum points = 11) 4 6 5 8 5 5 6 9 8 7 8 ↵a Unblended, cluster randomised, before and after controlled study
↵b Except all from geographically similar areas.
↵c Groups of patients similar, but some statistically significant differences in caregiver group for example, age and male sex
↵d Groups of patients similar, but there were more single handed GPs in the ‘classical learning’ group than the ‘blended learning’ group, and significance for this difference has not been calculated.
In this issue

British Journal of General Practice
Dementia diagnosis and management: a narrative review of changing practice








Jump to section
More in this TOC Section
Related Articles
Cited By...
Intended for Healthcare Professionals

