


Abstract
Background Early detection and management of dementia in primary care are difficult problems for practitioners. England's National Dementia Strategy 2009 seeks to improve these areas but there is limited evidence on how to achieve this most effectively.
Aim This review aims to identify and appraise empirical studies of interventions designed to improve the performance of primary care practitioners in these areas.
Design A narrative review of primary-care based studies.
Method Publications up to February 2010 were identified by searching the electronic databases MEDLINE, Embase, and PsycINFO, and bibliographies. The criterion for inclusion was that studies had to be of interventions aimed at improving detection or management of dementia in primary care. Exclusion criteria included studies in non-English publications, pharmacological interventions, and screening instrument studies. Quality was assessed using the PEDro (Physiotherapy Evidence Database) scale.
Results Fifteen studies were identified, of which 11 were randomised controlled trials. Eight reported educational interventions, and seven trialled service redesign, either by changing the service pathway or by introducing case management. Educationally, only facilitated sessions and decision-support software improved GPs' diagnosis of dementia, as did trials of service-pathway modification. Some of the case-management trials showed improved stakeholder satisfaction, decreased symptoms, and care that was more concordant with guidelines.
Conclusion The quality of the studies varied considerably. Educational interventions are effective when learners are able to set their own educational agenda. Although modifying the service pathway and using case management can assist in several aspects of dementia care, these would require the provision of extra resources, and their value is yet to be tested in different health systems.
INTRODUCTION
Due to the ageing of the population, the prevalence of dementia is rising. The costs to the NHS budget of caring for people with dementia in the UK has been estimated at £17 billion, which is more than for heart disease (£4billion), stroke (£3 billion), and cancer (£2 billion).1 Improving the detection of dementia was identified as an area for development in the National Service Framework for Older People,2 as well as the National Dementia Strategy;1 and keeping a register and demonstrating regular reviews of patients with dementia have been added to the list of clinical domains for the Quality and Outcomes Framework in the UK.3 GPs are in an ideal position to recognise the symptoms and signs of early dementia, and trigger the necessary investigation into the diagnosis of dementia.4 However, early detection of dementia is difficult to achieve, and is a problem for primary care practitioners around the world, who often report difficulties in recognising dementia and responding to the needs of patients with dementia.5-7
Barriers that delay diagnosis of dementia, or hinder management, have been discussed in another rapid appraisal review.8 These can be categorised as patient or societal factors, GP factors, and system factors. Patient or societal factors include stigma, and consciously or unconsciously delayed presentation. GP factors include diagnostic uncertainty, insufficient knowledge or experience, difficulties in disclosing the diagnosis, or the inhibiting effects of societal stigma which often perpetuates a diagnosis of dementia, and the therapeutic nihilistic views (that is, the futility of knowing the diagnosis of dementia) held by some healthcare professionals. Finally, healthcare systems create barriers, including time constraints and lack of support for practitioners, as well as financial or remuneration factors that militate against the management of complex patients in primary care.
A body of research exists that has explored and examined GPs' knowledge about dementia, how they go about making the diagnosis, what their management practices are, and whether they adhere to guidelines.8 Empirical studies have tested new interventions to improve the detection and management of dementia in primary care. This review investigates whether these interventions overcome established barriers to the underdiagnosis and suboptimal management of dementia in primary care, with the aim of informing the implementation of the National Dementia Strategy.
METHOD
Search strategy
A rapid appraisal approach was adopted to inform the current implementation of policy. Healthcare policy is influenced by many factors other than research evidence, including political pressure, ideological stance, and the need to take action. Influencing policy development and implementation is now an issue for researchers in all those countries with government-driven dementia strategies, and as Black has pointed out,9 timing is important:
‘Windows of opportunity to make change open up only rarely and briefly, when policy makers' values happen to coincide with the implications of research’.
How this fits in
Primary care practitioners are ideally positioned to detect and manage dementia, but it has been consistently shown in many countries that this is difficult to achieve: barriers to detecting and managing dementia in primary care are well established. There have been trials testing interventions aimed at improving these areas, but no general extrapolations have yet been made. Educating primary care practitioners can improve the detection of dementia, but only when the education is facilitated in small groups or provided as decision-support software. Changing the service pathway or provision can also improve aspects of diagnosis and care, for example with adherence to guidelines, patient or carer satisfaction, and reduced behavioural symptoms.
A rapid appraisal approach was adopted to inform the current implementation of the National Dementia Strategy in England, introduced in 2009. To avoid delays in the analysis and completion of the review, papers that were not easily accessible were not included. Publications about the detection and management of dementia in the community were searched for using MEDLINE, Embase, and PsycINFO, without restricting the date or language of publication. Searches were carried out between May 2009 and February 2010. A broad search strategy was adopted and search terms are listed in Box 1. This was executed as a two-step process with educat* added as the second step, after all the other search terms. Bibliographies of articles discovered for additional relevant literature were also examined.
Box 1. Description of two-step electronic database search process
Dementia
OR Cognitiv* Impair*
OR Alzheimer's Disease
AND
Primary Care
OR General Practi*
OR Family Pract*
AND
Diagnos*
OR Manag*
AND
Educat*
Search selection
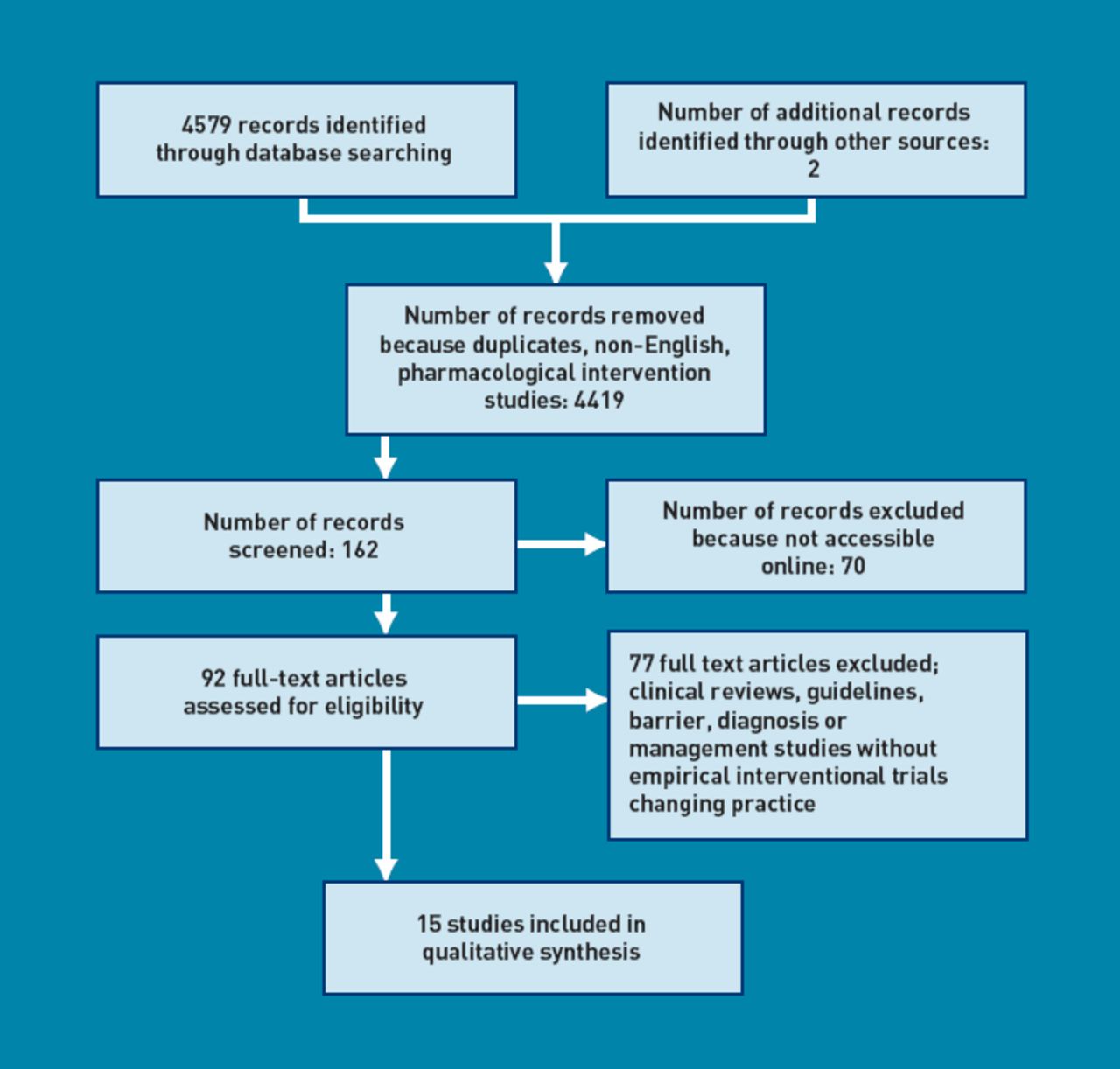
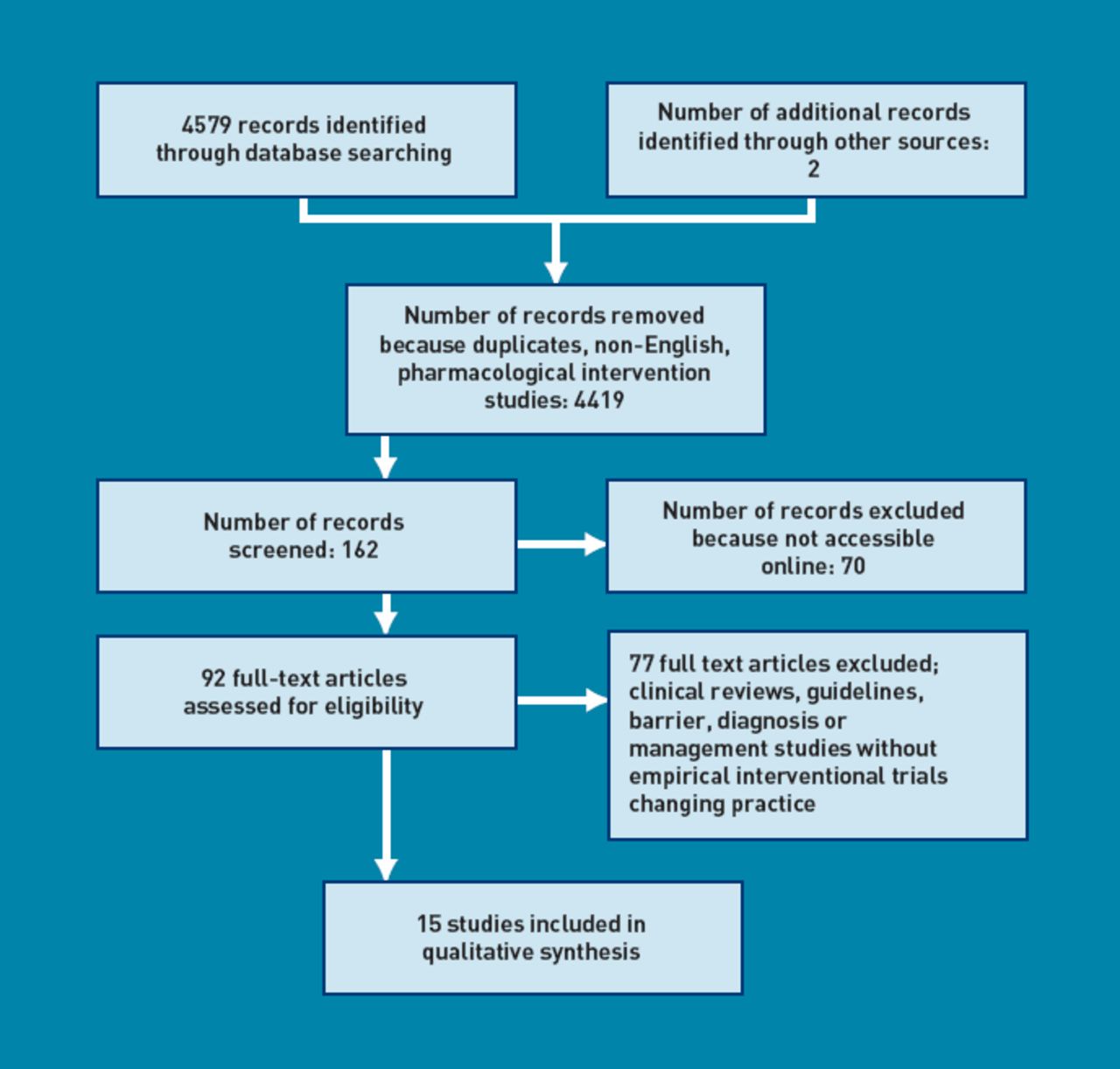
This search resulted in a total of 4579 articles. To prevent narrowing of the search scope and therefore potentially reducing the search sensitivity, the terms were not refined, but instead each title was reviewed — with its abstract if available — to ascertain its relevance. A number of exclusion criteria were then applied. All studies of pharmacological interventions were excluded, as were studies of the performance of cognitive function tests. Publications were excluded if they reported on the diagnosis or treatment of dementia in anywhere but a primary care setting (for example, the benefits of respite in long-term care facilities); if they related to a population outside the scope of this review (for example, interventions for caregiver health); or if they were clinical discussions about dementia diagnoses or care. Letters were also excluded, as were publications in languages other than English. Two other relevant articles were found, one directly from bibliographic searching, and a second was sourced following a recommendation from an expert in the field. Figure 1 shows the search process, presented according to PRISMA guidelines.10
{kind=link}
PRISMA flowchart
After applying these criteria, 162 articles remained, but 70 of these were not readily obtainable and these were also excluded for pragmatic reasons; 77 of the remaining 92 papers were excluded after analysis because they were clinical reviews, guidelines, studies of barriers, or studies without interventions designed to change practice. References in the 92 papers were reviewed to identify other intervention studies.
Data extraction
Data were extracted from each study report to allow comparison of interventions, and to assess the quality of study designs. The characteristics chosen for comparison include location and type of study, size, recruitment process, methodology, outcome measures, results, and conclusions (Table 1). A detailed description of each intervention can be found in Table 2. Randomised trials were assessed for quality using the PEDro (Physiotherapy Evidence Database) scale,11 as shown in Table 3. The PEDro scale was chosen because its assessment of blinding is very relevant to empirical studies in dementia. In quality-rating scales that consider double-blinding as the central methodological issue, studies would lose points for failing to be blinded. The PEDro rating scale divides blinding into participants, therapists, and assessors, recognising that while not all components of trials can be blinded, it is preferable that some groups are blinded rather than none at all.12
A descriptive comparison of controlled trials
Descriptions of the content of the interventions
APEDro (Physiotherapy Evidence Database) scale evaluation of studies in the review
RESULTS
Fourteen of the fifteen studies reviewed were controlled trials, and one was a qualitative study. Three of the fourteen trials are still under way and have results pending. Studies with published findings are shown in Tables 1 and 2.
Educational interventions
There were eight studies that evaluated educational interventions. Of these, one still has results pending,13 and one tested the implementation of guidelines for the diagnosis of dementia in Denmark.14 The remaining six involved either delivering seminars or workshops to primary care physicians, or other educational interventions, such as facilitated small-group learning or the use of decision-support software. Five of these six studies measured whether the educational intervention would improve detection and management,15-18 while one focused on diagnosis alone.19
Two of the studies examined whether educational seminars or workshops would change primary care physicians' diagnostic or management capabilities. Rondeau etal included training on the use of neuropsychological testing but failed to demonstrate an improvement in detection rates in the intervention group as compared with the controls.19 Chodosh et al delivered five educational seminars and subsequently measured knowledge about capacity, evaluation, and management of patients with dementia, as well as attitudes or perceptions about the quality of care (as part of the ACCESS study).18 They showed that the primary care physicians who had received the intervention knew more about determining capacity, and more of them felt that management was difficult, but there were no other statistically significant differences in knowledge, attitudes, or perceptions of quality of care.
A third study looked at whether ‘blended learning’ methods — a combination of traditional teaching methods, e-learning, and the use of other learning media — would improve GPs' knowledge acquisition in the diagnosis and management of dementia. This found that both ‘blended learning’ and classical learning methods improved knowledge in these areas, but no significant difference between the groups was found, although a subgroup analysis showed that when GPs self-reported as having used the e-learning modules, their knowledge gain was significantly better than the other group's (an increase in knowledge score of 1.17, 95% confidence interval [CI] = 0.20 to 2.14, P= 0.019).20
Four of the educational intervention studies investigated facilitated or small-group teaching. Facilitated learning can be described as an educational process wherein the learners are actively involved by collaborating and negotiating in all components of their own learning. One of these studies13 evaluated a multifaceted dementia training programme which involved pairing GPs with primary care nurses, and comprised individual coaching sessions, two small-group interactive workshops, and a computerised clinical decision-support system. Results for this are still pending.
A further two studies demonstrated positive results from their interventions. The first was qualitative, used a facilitator to lead a small-group session, and showed, in focus group discussions after the intervention, that there was increased knowledge about dementia and increased motivation for self-directed learning. This study suggests that active learning and identifying needs with a facilitator can be an effective way for GPs to learn more about dementia.15Thesecond used three separate methods of self-directed learning with an electronic tutorial on a CD-ROM, computer decision-support software, and practice-based workshops, and showed that the latter two significantly increased the detection of dementia by 30% (P= 0.01) and 31% (P=0.02) respectively, although there was no improvement in concordance with guidelines on processes of diagnosis or management.16
The last study using facilitated or small-group learning investigated the detection of cognitive impairment rather than dementia (as well as improving care for incontinence and falls), by giving a 3-hour small-group educational session on Assessing Care of Vulnerable Elders (ACOVE) quality indicators. It found that while the overall care of cognitively impaired patients did not differ, the intervention group's primary care physicians were more likely to give attention to caregiver education, patients' decision-making capacity, and discussion about driving.17
Finally, one intervention study sought to improve adherence to guidelines on diagnosing dementia using educational seminars, outreach visits from facilitators, or reminder letters containing the main recommendations from the guideline. It concluded that there was no significant difference between intervention and control groups in the number of diagnostic evaluations undertaken, the number of investigations ordered, or the number of cognitive tests performed. However, a limitation of this study is that the interventions were delivered to individual GPs, but the outcomes were measured at practice level.14
Service innovations
Studies of service innovations trialled interventions that either modified an existing care pathway, or introduced case managers. Seven intervention studies of this kind were identified, two with results still pending.21,22 Of the remaining five, one evaluated a modified care programme,23 and four evaluated case managers.2-7 Of the studies that investigated changing the service pathway, one involved using the EASYcare Dutch Geriatric Intervention Programme, an in-home assessment using the validated EASYcare instrument which assesses function, cognition, mood, and goal setting.28 This was performed by a geriatric specialist nurse, but was triggered by GPs when they encountered a patient with a problem requiring action. A full description of the intervention is found elsewhere.29 Results showed that dementia diagnosis was significantly improved in the intervention group (29% compared with 9%, P=0.02).23
In evaluations of case management, the case manager undertook a range of tasks, including case finding, assessment, care planning, service coordination, and monitoring. One study also evaluated the intervention of a care manager using web-based support software for care planning and coordination.24 Care managers provided follow-up, support, and planning advice for the caregiver. Patients in the intervention group received care more adherent to 21 out of 23 guideline recommendations (P = 0.013), and better care was noted across all four domains (assessment, treatment, education and support, and safety; P = 0.001). Adjusted risk ratios for the improved guideline processes in the intervention group ranged from 1.2 (95% CI = 1.1 to 1.3) to 8.3 (95% CI = 5.2 to 21.7). These patients also received more community services (risk ratio 1.3; 95% CI = 1.0 to 1.9), and were prescribed more anticholinesterase inhibitors (P=0.32).24
A second study used care consultations via telephone between Alzheimer's Association staff and the patient or caregiverto assist with assessment, identify problems, and develop strategies to solve problems using a range of resources. The results showed that patients with more severe memory symptoms in a subsample of the intervention group were less likely to have hospital (regression coefficient beta = -2.97, P= 0.07) or accident and emergency admissions (beta = -2.30, P= 0.03), and had fewer contacts with physicians. They also had higher satisfaction levels with the service and lower depression rates. In addition, their feelings of embarrassment and isolation decreased, as did relationship strain.25
A third study of service innovation did not have such positive results, but still demonstrated some benefit. Callahan et al used a collaborative care-management model over 12 months, giving patients and caregivers education and support.26 Results showed that the intervention group had fewer behavioural symptoms, but there were no differences in cognition, depression, or functional scores in patients. The caregivers had improved stress scores. Overall, the intervention group had more contacts with physicians and nurses but there was no change in hospital or nursing home admissions.
The final study in the case-management category used dementia care consultants who contacted the caregiver monthly for 12 months and helped with behavioural symptoms, legal or financial planning, educational meetings, support, and respite services. Members of the intervention group were 40% less likely to end up in nursing homes than those in the control group, but this difference did not achieve statistical significance. No other differences were found, although 82% of caregivers were satisfied with the intervention.27
Within this category, there are two studies with results still pending. One used district nurses working as case managers for geriatric patients, who offered a variety of services comprising assessments, planning, coordination, collaboration, and monitoring of care.21 The other used a mixture of educational sessions (comprising a variety of materials and methods of delivery) for primary care physicians as well as using a dementia care manager as a case manager offering similar services such as assessment, monitoring, problem solving, and referrals to other services.22
Quality of studies
The 10 completed controlled trials were evaluated using the PEDro scale (Table 3), and of these only four studies attained a score of 8 out of 11 (>70%). Only one of these four studies involved testing an educational intervention;18 the remainder were studies evaluating service innovations. The remaining four educational interventions demonstrated weakness mainly in their methodology rather than their analysis (for example, failing to specify eligibility criteria), or had flaws in their random allocation and blinding processes. The studies of service innovation fared much better, with only one of the four scoring lower than 7;23 the study by Callahan et al study reached 9 points out of 11, losing points on blinding of the therapists, and not employing an intention-to-treat analysis.26 As with the educational interventions, these studies' limitations mainly involved the blinding process. It could be argued for all of these interventional studies that blinding of the participants and therapists would be difficult at least, if not impossible, and so lower scores may be inescapable.
DISCUSSION
Summary
Interventions designed to improve the detection and management of dementia can be categorised into two types: those that attempt to change primary care physicians' behaviour through education, and those that seek to alter or improve service provision to facilitate diagnosis and/or management. It appears difficult to bring about change in either diagnosis or management through educational interventions alone. None of the seminar-based interventions was able to demonstrate any improvement in outcomes measured. In studies of the facilitated or small-group educational strategies, qualitative analysis of facilitated learning suggested that it can improve knowledge and self-directed learning,15 while practice-based workshops and decision-support software appeared to improve the detection rate but not the management, in a trial of relatively limited quality according to the PEDro rating.16 Blended learning techniques only demonstrated a significant improvement in knowledge gain when GPs self-reported using the online modules.20 Among interventions that altered the care pathway, the trial of an in-home assessment of patients' mental wellbeing and functional capacity showed a significant improvement in detection rates.23 Two studies of case management demonstrated improved management either by providing care more adherent to guidelines, increasing referrals to community services, and increasing anti-cholinesterase prescribing,24 or by reducing hospital use and consultation rates with physicians, and by decreasing feelings of depression or isolation.25
Strengths and limitations
While the search terms used were broad enough to capture most relevant publications, it is possible that there is research that was not identified, because of the omission of one or other of the strata of terminologies; for example, primary care or general practi* or family practi*. This means that all relevant studies may not have been found, although in reality the lack of any substantive new studies identified on searching the bibliographies from known articles suggests that this is unlikely. In addition, many of the relevant articles identified by the search terms (70 of 162 articles) were either not in English, or were not readily located or available, so potentially some important or pertinent research that could have enriched this review has been foregone.
Sample sizes for some of the studies were small, which could reduce their generalisability. Furthermore, the recruitment process of some of the studies lacked robustness, as at times there was potential for selection bias in the way the researchers identified their sample.
Many of the studies omitted to mention that power had been calculated or met, and some of the studies appeared to neglect to analyse on an intention-to-treat basis.
As with all comparative reviews, while each study can be appraised individually, objective comparisons between them are more difficult because the outcome measures were different, and there was extensive variation in the outcomes being measured in the studies examined here.
The PEDro rating scale of trial quality does appear applicable as a method to examine the interventions studied here, because in these studies blinding of some or all groups of participants, therapists, and assessors, would have been impossible. Moreover, by rewarding concealment of allocation, intention-to-treat, and adequacy of follow-up, the PEDro ratings are also recognising other internal validity measures even if blinding was not possible.
Comparison with existing literature
This review has attempted to examine which interventions are being trialled to improve the detection and management of dementia in primary care. An earlier review investigated the common barriers to this being achieved,8 and concluded that the obstacles presented themselves in one of three ways: as a result of patient/caregiver or even societal behaviour or views (for example, delayed presentation or stigma of diagnosis); as a result of GPs' knowledge, attitudes, or behaviour (for example, diagnostic uncertainty or lack of experience); or due to system weaknesses (for example, resource deficits in time or money, or perceived lack of support from specialists for primary care).
One way to understand the outcomes of the interventional studies is to consider whether the interventions that produced positive results were successful because they designed their educational session to tackle specifically-determined barriers, or because they carefully chose the method of delivery based on established educational theory. One of the weaknesses of some of the studies reviewed here is that the content of the intervention was not adequately described, making it difficult to deduce how it affected the outcomes. However, seminar-structured educational sessions did not appear to enhance performance, a finding that has been corroborated by earlier non-experimental studies.30,31 This finding supports the argument that this educational method is of little value in changing complex professional behaviour or healthcare outcomes,32 and in the authors' opinion no further studies of this kind of intervention are needed.
In contrast, facilitated small-group learning and decision-support software proved to be effective educational approaches, increasing diagnostic rates if not enhancing management or care, although it is important to be cautious about this given the methodological limitations of these studies. These findings reveal more about successful educational strategies for the development of GPs' diagnostic capabilities, but do not illuminate methods to overcome other GP barriers such as stigma, or their ability to adhere to guidelines. Educational interventions introduced as part of a strategy to enhance the performance of primary care in the diagnosis of dementia are unlikely to have an impact if they are not based on facilitated small-group learning. Studies of educational strategies designed to improve GPs' diagnostic or management skills in other specific clinical tasks, including mental health,33 laboratory testing,34 and prescribing habits,35 support these conclusions, as do systematic reviews of educational interventions designed to improve professional practice.36-38
The systematic reviews conclude that conferences and workshops during which no attempts were made to elicit practice needs or to facilitate change fail to bring about a change in performance or health outcome, and that reminder systems (comparable to decision-support software) are also effective at changing performance but are very much dependent on when and how they are used. Moreover, outreach visits (comparable to facilitated sessions) are effective ways of changing health professionals' behaviours and practices.
The current authors hypothesise that the more precisely the educational needs of an individual or group are ascertained, the more the intervention can be customised to address those needs, resulting in a greater impact on behaviour or practice. There is evidence to support this, demonstrated by one study that found that the more personalised an educational strategy is, the more likely is the chance of success.39 However, a Cochrane review of tailored interventions to overcome identified barriers to change, which examined 15 separate tailored educational interventions, showed limited evidence for the benefit of tailored versus non-tailored or no intervention. Apart from the small sample size of these studies, some of the difficulties that were identified included the complexities around knowing whether all barriers had been uncovered, how valid they were, how to prioritise the importance of each barrier, and whether the barrier had been addressed by the intervention chosen.40
The interventions built around service modification showed positive results overall. One additional study that significantly increased the rate of detection in dementia in Sweden by introducing a locality programme could not be considered for the purposes of this review, because details of the actual programme appear only to be published in Swedish.41 The service innovation that produced the most benefits adapted the traditional doctor-patient-caregiver paradigm by introducing a multidisciplinary approach.23 Another non-controlled pilot study that tested shared (group) medical appointments for patients with dementia, and that demonstrated benefits by enabling collaboration between patients, caregivers, and clinicians,42 supports this conclusion. These findings are consistent with the arguments of de Lepeleire et al,43 who proposed that detection could be improved by employing a stepwise strategy, that improving the referral pathway could be more effective than introducing disease-specific guidelines, and that a strong, multidisciplinary approach enables diagnosis. A number of interventions that added resources to existing services by employing additional staff — usually in the form of specialist nurses but also voluntary sector advisers — also showed increased detection and adherence to guidelines, fewer admissions to hospital, and higher patient satisfaction.
All of the completed studies took place in the US, which means that, given the diversity of healthcare systems, it cannot be assumed that such positive findings could be extrapolated and applied elsewhere. There have been a few locally administered attempts to change systems in the UK, which anecdotally have accomplished reduced waiting times and increased all stakeholder satisfaction, for example, by offering memory clinics within the primary care setting,44 but these are yet to be tested empirically.
Implications for practice and research
There are implications from these intervention studies that can help inform the implementation of the National Dementia Strategy.1 Carefully planned educational interventions, which are determined by the learners and tailored to their needs, can change professional practice and can lead to enhanced knowledge about and detection of dementia. Such educational interventions can be integrated into GPs' training and can help achieve the improvements to care that the National Dementia Strategy is seeking; seminar-based training appears to be ineffectual.
The National Dementia Strategy has also highlighted the need for innovative approaches to improve dementia care and to achieve best outcomes for patients and their families, so case management ought to be seriously considered, despite its limited impact in studies in the US. However, employing additional staff to case-manage patients — often to assess, diagnose, problem solve, and monitor the patient — assumes that GPs are unable to fulfil this role themselves. In the last few decades, GPs have undertaken more and more management of chronic conditions, many of which are also complex; for example, asthma, diabetes, and ischaemic heart disease.34,45
Instead of addressing barriers to high-quality dementia care, the introduction of specialist nurses could be seen as an attempt to bypass barriers. This has implications for resources and may also be seen as an implicit criticism of the ability of GPs to improve their practice. Whether case management designed to bypass existing services will be economically justified, and sustainable when compared with enhancing the ability of GPs to provide a similar role, remains to be investigated.
Notes
Funding body and competing interests
Steve Iliffe is chief investigator of the EVIDEM programme (Evidence-based Interventions in Dementia, www.evidem.org.uk) and has received financial support from the Department of Health's National Institute for Health Research Programme Grants for Applied Research funding scheme (RP-PG-0606-1005). The views and opinions expressed in this article are those of the authors and not necessarily those of the NHS, the National Institute for Health Research (NIHR), or the Department of Health. Steve Iliffe is also associate director of the coordinating centre for the Dementias and Neurodegenerative Diseases research network (DeNDRoN), funded by the NIHR. He has received speaker's fees from pharmaceutical companies with an interest in dementia but has no other conflicting financial academic or personal interests relevant to this paper. Tamar Koch has no competing interests.
Provenance
Freely submitted; externally peer reviewed.
Additional information
A technical appendix, searches, and dataset are available from the corresponding author at t.koch{at}ucl.ac.uk.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received March 25, 2010.
- Revision received May 4, 2010.
- Accepted May 20, 2010.
- © British Journal of General Practice 2011
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

