


Abstract
Background Emerging evidence suggests that early intervention and prevention programmes for mental health problems in the offspring of parents with depression are important. Such programmes are difficult to implement if children with psychiatric disorder are not identified and are not accessing services, even if their parents are known to primary care.
Aim To investigate service use in children of parents who have recurrent depression, and factors that influence such contact.
Design and setting A total of 333 families were recruited, mainly through primary health care, in which at least one parent had received treatment for recurrent depression and had a child aged 9–17 years.
Method Psychiatric assessments of parents and children were completed using research diagnostic interviews. The service-use interview recorded current (in the 3 months prior to interview) and lifetime contact with health, educational, and social services due to concerns about the child’s emotions or behaviour.
Results Only 37% of children who met criteria for psychiatric disorder were in contact with any service at the time of interview. A third, who were suicidal or self-harming and had a psychiatric disorder at that time, were not in contact with any service. Lack of parental worry predicted lower service use, with higher rates in children with comorbidity and suicidality.
Conclusion Most children with a psychiatric disorder in this high-risk sample were not in contact with services. Improving ease of access to services, increasing parental and professional awareness that mental health problems can cluster in families, and improving links between adult and child services may help early detection and intervention strategies for the offspring of parents with depression.
INTRODUCTION
Some 10% of children and adolescents in the UK have a psychiatric disorder,1,2 of whom approximately one-quarter will access mental health services over a 3-year period.3 Psychiatric disorders have both an immediate and long-term negative impact on young people, and show strong continuities with adult mental health problems and psychosocial disadvantage.4,5
Emerging evidence suggests that early detection, intervention, and prevention are most useful when targeted at children with known risk factors or with some symptoms already present.6 Despite this, most psychiatric disorders in young people go unrecognised and untreated, even in groups that are known to be at risk.
The children of parents with recurrent depression are an identifiable high-risk group.7,8 Meta-analysis has shown that the offspring of parents with major depressive disorder have higher rates of psychiatric disorder than children of parents who are unaffected, including a three- to fourfold increased risk of developing depression.9,10 Furthermore, when depression does arise in the children of parents with depression, evidence suggests that the course is more severe and impairing.11
As adult depression is the third most common reason for consultation in general practice in the UK, children of parents with depression are a potentially accessible high-risk group for early detection of problems and targeted intervention. However, clinical knowledge about the parent is not necessarily linked to the child, and different services are likely to be involved in the assessment and management of adult and child mental health problems. Understanding the patterns of service use in the offspring of parents with depression may help identify the different types of services that are involved and potential barriers to children receiving help.
This study focuses on a sample of children of parents who were known by their GP to have recurrent depression. The aims were to:
examine rates of service use for children with psychiatric disorder regarding mental health concerns;
identify which services were accessed;
identify factors associated with access to these services by children or parents on behalf of their children.
How this fits in
Children of parents with depression are at increased risk of psychiatric disorder. Despite parents attending GP practices, their children’s mental health needs often go unnoticed. In primary care, it is important not to miss the opportunity for early intervention and treatment in this high-risk group of children, in order to prevent poor long-term outcomes.
METHOD
Participants
The sample consisted of families seen at the baseline assessment of the longitudinal Early Prediction of Adolescent Depression study.12 Participants included 337 parents with a history of recurrent unipolar depression (at least two episodes of depression confirmed at interview), together with their offspring. Participating children were required to:
be aged 9–17 years;
be biologically related to the affected parent and living at home; and
have an IQ of ≥50.
To be included in the study, consent was required from both parent and child at study entry. If >1 eligible child was present in the household and willing to participate, the youngest child was selected to eliminate bias. Parents with a bipolar or psychotic diagnosis at recruitment or during baseline assessment were excluded from the study.
Families were recruited from across the UK. The majority were recruited from GP surgeries in South Wales (n = 263); others were recruited using a database of adults previously identified as having recurrent unipolar depression (n = 64), as well as posters in local health centres, hospitals, and the depression alliance newsletter (n = 10). Figure 1 illustrates the recruitment process. Of the 337 participating families who met the inclusion criteria, four failed to provide sufficient data or complete the service-use questionnaire, leaving a final sample of 333 families available for analyses. The adult sample included 311 mothers and 22 fathers (aged 26–55 years, mean age 41.7 years); the child sample included 195 females and 138 males (aged 9–17 years, mean age 12.4 years).
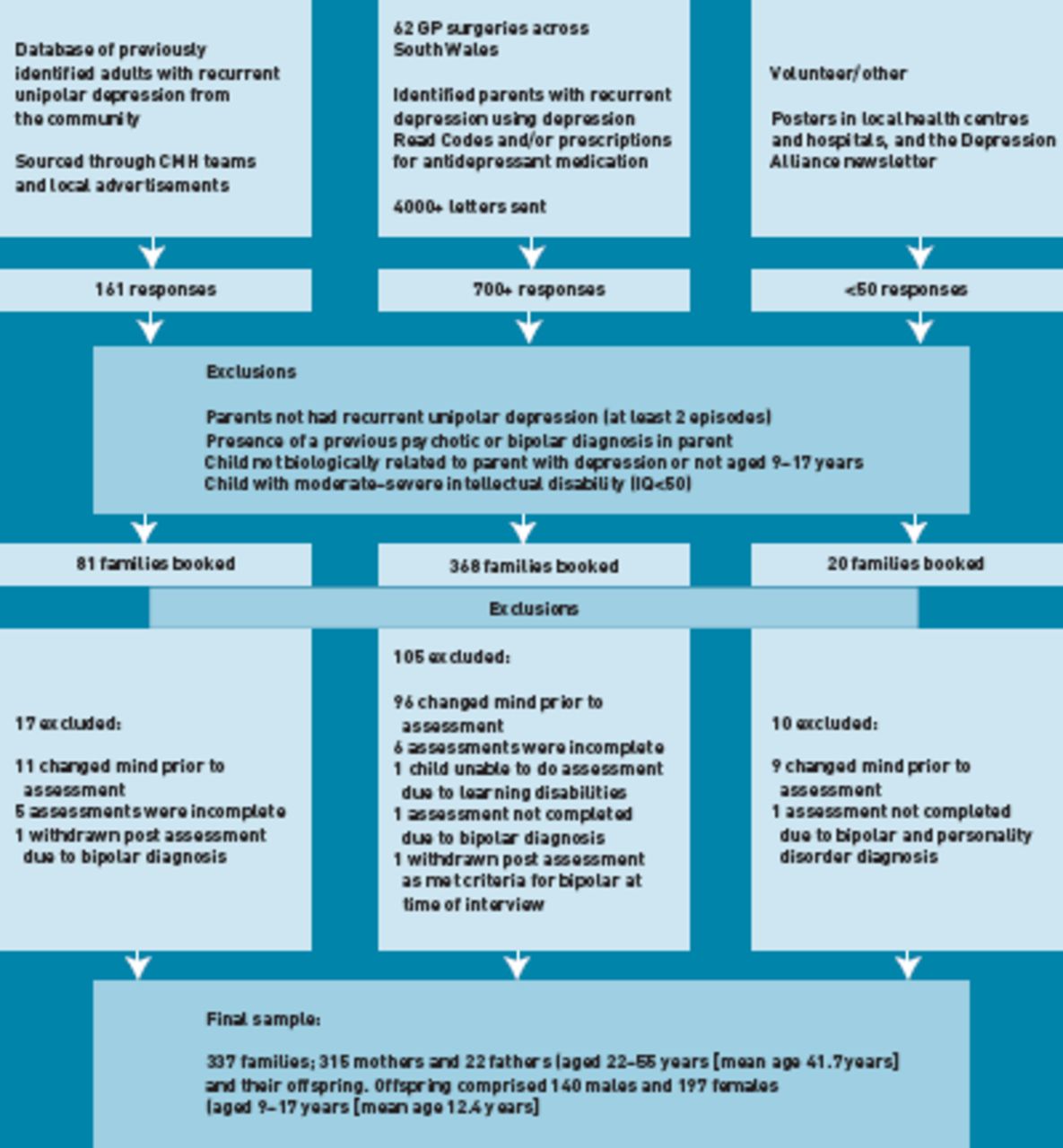
Flow chart of the Early Prevention of Adolescent Depression study’s recruitment process.
Procedure
Participating families were visited at home. Parents and children were interviewed independently by two trained research psychologists, and consent was obtained. Questionnaire data were also collected.
Measures
Service-use interview.13
This semi-structured interview, completed by the parent with an interviewer, asks about any contact with services (lifetime and in the 3 months prior to interview) by the parent or child because of concerns about the child’s emotions or behaviour. Services were classified as either medical or non-medical. Medical services included primary care, paediatrics, and mental health services; non-medical services included education (schools and special educational needs [SEN] services), social services, and youth justice services. Parents were also asked if they had been worried about their child, whether they had ever been reluctant to ask for help and, if so, why. Qualitative data regarding the reasons for reluctance were then simple-coded into categories.
The Schedules for Clinical Assessment in Neuropsychiatry.14
This semi-structured interview was administered to the affected parent by a trained interviewer, and was used to assess whether an episode of depression, as classified by the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), had occurred over the previous month.
Child and Adolescent Psychiatric Assessment (CAPA) — parent and child versions.15
This diagnostic interview was used to assess child mental health over the preceding 3 months. The parent and child versions were completed independently and were used to assess child mood disorders, attention deficit hyperactivity disorder (ADHD), disruptive behaviour disorders (conduct disorder, oppositional disorder, and disruptive disorder not otherwise specified), anxiety, and eating disorders. Child diagnoses were generated according to criteria from DSM-IV, based on CAPA symptoms and impairment of functioning. A diagnosis was considered present if reported by either the parent or the child at interview. All children who met diagnostic criteria, together with all those who were sub-threshold, were reviewed by two senior child and adolescent psychiatrists.
The parent and child CAPAs were also used to identify children who had experienced suicidal ideation or who had self-harmed (that is, endorsed the items relating to thoughts about death, suicidal thoughts, plans, behaviours, or self-harm).
Questionnaires
Hazardous alcohol use in the parent was assessed using the Alcohol Use Disorders Identification Test. This is a self-report questionnaire completed by the affected parent at interview. Scores of ≥8 are considered indicative of hazardous and harmful alcohol use.16
Additional information
Information regarding the number of previous episodes of parental depression (dichotomised into ≥4 episodes versus <4) and episode severity (a severe depressive episode was defined as involving either severe impairment or hospitalisation) was obtained from the parent retrospectively, using a life history calendar approach.17 Information was also obtained at interview from the parent regarding family demographic variables including child age and sex, parent age, and family composition.
Analysis
The data were analysed using SPSS (version 16). Data on rates of child DSM-IV diagnosis, child suicidal thoughts and self harm, service use, and patterns of service use were obtained. A series of univariate logistic regression analyses were used to investigate factors affecting service use in those children with psychiatric disorder.
RESULTS
Rates of child DSM-IV psychiatric diagnoses
Of the 333 children included in the present analysis, 79 (23.7%) met criteria for a current DSM-IV diagnosis at the time of the assessment. Some 16 (4.8%) children met criteria for a mood disorder, 38 (11.4%) for an anxiety disorder (specific phobia not included), 21 (6.3%) for ADHD, and 24 (7.2%) met criteria for a disruptive behaviour disorder. Over a quarter of children with psychiatric disorder experienced comorbidity (26.6%), which ranged from two to five diagnoses.
Rates of service use
Of those children with a DSM-IV diagnosis at the time of interview (n = 79), only 29 (36.7%) accessed services in the 3 months prior to interview due to concerns about their emotions or behaviour. A fifth (n = 17, 21.5%) had been in contact with medical services and 21 (26.6%) with non-medical services (Table 1). Of the 79 individuals with a psychiatric disorder at the time of interview, 48 (60.8%) had been in contact with services at some point in their lifetime — 33 (41.8%) had been in contact with medical services, and 38 (48.1%) in contact with non-medical services.
Percentage of children with and without psychiatric disorder accessing the different types of services
Type of service accessed
For the children who met DSM-IV criteria for current psychiatric disorder, the types of services that were accessed varied. Teachers and special educational needs (SEN) services were the most frequently accessed services. Table 1 summarises the frequency of utilisation of each of the services (ever and in the 3 months prior to interview) in those children who had and did not have a psychiatric disorder at the time of interview.
Access to services according to sex and diagnostic group
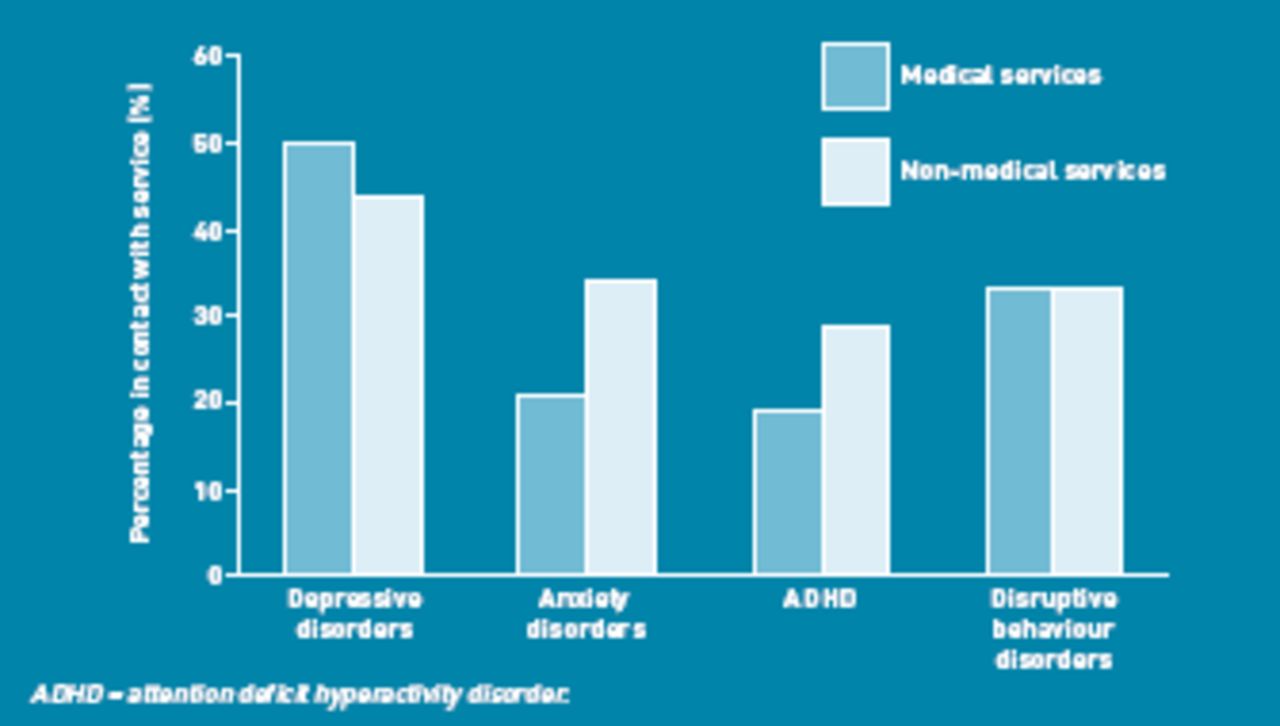
The pattern of service use varied according to child diagnosis (Figure 2). Services were more likely to be accessed when children had a mood disorder than when they had anxiety, ADHD, or disruptive behaviour disorders (Table 2). For children with anxiety disorder, service use was more frequent among the females than males. No female children with ADHD were in contact with services. Access to services was similar for males and females with mood disorder or disruptive behaviour disorder.
{kind=link}
{kind=link}
Type of service accessed according to disorder type in the 3 months prior to interview.
Access to services according to child disorder type and sex, in the 3 months prior to interview
Impact of suicidal ideation and self-harm on service use
Of the 333 children included in these analyses, 23 (7.0%) were recorded as having experienced suicidal ideation or self-harm in the 3 months prior to interview. Of these, nine (39.1%) had not accessed services. For those children who had a psychiatric disorder, 15 (19.0%) endorsed suicidal ideation or self-harm symptoms at interview. In total, five (33.3%) of the children who had disorder and suicidal ideation at the time of interview had not accessed any services in the 3 months prior to interview.
Reluctance to ask for help
In total, 15 (19.0%) of parents with children who met criteria for a psychiatric disorder had felt reluctant to ask for help, even though they felt they needed it. Reasons for this included: previous bad experiences (n = 6); worries about stigma (n = 4); fear that it would reflect badly on them as a parent (n = 4); concern about social services getting involved (n = 2); reluctance to admit there was a problem (n = 1); and feeling that they should deal with their own problems first (n = 1). However, reluctance to ask for help was not significantly associated with lack of service use among children with disorder (odds ratio [OR] 1.19, 95% confidence interval [CI] = 0.38 to 3.76, P = 0.769).
Potential barriers to service use
A series of univariate logistic regression analyses investigated factors affecting service use among children with psychiatric disorder (Table 3). A number of factors were significantly associated with service use. Children with comorbidity (≥2 disorders) were more likely to access services (OR 5.73, 95% CI = 1.95 to 16.90, P = 0.002) than children with a single disorder. Children in whom suicidality/self-harm had been recorded were also more likely to access services than children without suicidality/self-harm.
Univariate analysis showing potential barriers to services for children with a psychiatric disorder defined by DSM-IV
When looking at potential barriers to service use in children with disorder, lack of parental concern was significantly associated with lack of service use (OR 7.20, 95% CI = 2.36 to 22.01, P = 0.001). Neither features of parental depression (current parental depressive episode, frequent depressive episodes, or presence of a severe depressive episode) nor sociodemographic factors (child age, child sex, age of the affected parent, lone parent family), nor hazardous drinking in the parent significantly affected service use (data available on request).
DISCUSSION
Summary
Almost two-thirds of young people with psychiatric disorder in this study were neither being seen by health or other services at the time of interview, nor were their parents seeking help on their behalf. Although all parents were known to primary care because of recurrent depression, only 36.7% of young people with current psychiatric disorder had accessed any service within the 3 months prior to interview, and only 15.2% of those accessed mental health services. The most commonly accessed services by those with disorder were teachers and SEN services (accessed by 26.6%). Only 11.4 % with a psychiatric diagnosis had accessed primary health care in the 3 months prior to interview. Children with ≥1 psychiatric diagnosis were more likely to access services than those with one psychiatric diagnosis only. Service use was also more likely among children with suicidality/self-harm then children without suicidality/self-harm. A lack of parental concern about child mental health was a barrier to children accessing services.
Strengths and limitations
Data were drawn from a large study of children at high risk for psychopathology, recruited predominantly from general practice. Assessments were rigorous, involving multiple informants and diagnostic interviews, and access to a wide range of different services was considered. The findings must however be interpreted in light of several study limitations. Most of the parents were mothers and they were mainly from one region of the UK (south Wales). However, families were recruited from 62 different practices and it is known that depression more commonly affects females, with females more likely to seek treatment.18
The service-use interview, which was used as a measure of access to services due to concerns about the child’s emotions or behaviour, is a parent-completed measure and depends on the parent’s recall.
It is possible that the child may have accessed services without the parent knowing, causing some service use to go unreported. However, parent and child reports of service use have previously shown reasonable agreement.19
The interview does not distinguish between child and parent access to services. The pattern of use and potential barriers may be different for these groups.
Finally, as the interview records access to services due to concerns about emotions or behaviour, it was not possible to establish whether children had been in contact with services for other reasons.
Comparison with existing literature
Most psychiatric disorder in children and adolescents is poorly recognised and poorly treated.20 In the follow-up of the 1999 British Child and Adolescent Mental Health Survey, 56.7% of children with disorder had accessed one or more services in the preceding 3 years, and 25.1% had accessed mental health services.3 These rates are similar to those in this high-risk sample where 60.8% of children with a disorder reported ever having accessed any services (36.7% in the 3 months prior to the interview) and 27.8% reported ever having accessed mental health services (15.2% in the 3 months prior to the interview).
Reported barriers to parents seeking help for their children with emotional or behavioural difficulties have been previously described.21 These include embarrassment, stigma of mental health problems, concerns about the child being labelled or given a diagnosis, concerns about being judged as a poor parent, and concerns their child would be removed from the family should they seek help. Similar factors were given as reasons for reluctance to access services in this study, but they did not significantly impact on rates of service use.
Other research suggests that demographic, social, and psychiatric factors impact on service use in children of parents with mental illness.22 Of the factors looked at (parent and child age, child sex, lone parent family, hazardous drinking, parent current depression diagnosis, frequency and severity of depressive episodes), none were found to be significantly associated with service use in this study. Instead, lack of parental concern about children’s problems was identified as a more important barrier to service use. This is unsurprising but raises the question of how such children are best helped. School-based mental health and depression prevention programmes, including increased awareness of risk of depression, are likely to be especially useful for children whose parents show a lack of concern.23
Implications for practice
Most children with disorder in this study were being seen by services other than primary care. However, parent depression will be mostly managed in general practice. This highlights the need for GPs, who are seeing parents with depression, and for parents themselves to be aware of the risk of mental health problems in their children. This may be achieved by GPs explicitly asking a parent about mental health concerns in offspring during the primary care consultation with the parent. This would also be helpful for linking clinical information on different family members and across different services, which, at present, may not be recorded.
For those children who do see their GP, such contact is an opportunity for intervention. Although most children do not themselves explicitly seek help for their mental health difficulties, they may consult their primary care doctor for other reasons.24 It has been suggested that 20% of adolescents presenting at general practice clinics have a depressive disorder.25 This figure is likely to be considerably higher when parents suffer from depression. However, even when children have been identified in primary care current treatment options are limited. Other services also have their role to play and more research is needed to develop and evaluate brief evidence-based interventions for young people presenting with mental health problems.
In summary, young people in need of services are not accessing them. This is a particular concern for those with psychiatric disorder and suicidal ideation/self harm. All the children in this sample were offspring of parents with recognised recurrent depression and, as such, a group that is well known as being at high risk of mental disorder. There needs to be better recognition of the links between parent and child mental health problems.
Acknowledgments
We are very grateful to all the families and GPs who helped with this study. We thank the assistant psychologists who helped with data collection and investigators who are involved in the primary study: Professor Michael Owen, Cardiff University; Professor Gordon Harold, Leicester University; and Dr Daniel Smith, Cardiff University.
Notes
Funding
This research was funded by the Sir Jules Thorn Medical Trust, London. Stephan Collishaw is funded by The Waterloo Foundation, Cardiff.
Ethical approval
Ethical approval was granted by the Multicentre Research Ethics Committee for Wales, Cardiff (MREC reference number 06MRE09/48).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received November 9, 2011.
- Revision received December 14, 2011.
- Accepted January 24, 2012.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

