


Abstract
Background Visual impairment (VI) is rising in prevalence and contributing to increasing morbidity, particularly among older people. Understanding patients’ problems is fundamental to achieving optimal health outcomes but little is known about how VI impacts on self-management of medication.
Aim To compare issues relating to medication self-management between older people with and without VI.
Design and setting Case–control study with participants aged ≥65 years, prescribed at least two long-term oral medications daily, living within the community.
Method The study recruited 156 patients with VI (best corrected visual acuity [BCVA] 6/18 to 3/60) at low-vision clinics; community optometrists identified 158 controls (BCVA 6/9 or better). Researchers visited participants in their homes, administered two validated questionnaires to assess medication adherence (Morisky; Medication Adherence Report Scale [MARS]), and asked questions about medication self-management, beliefs, and support.
Results Approximately half of the participants in both groups reported perfect adherence on both questionnaires (52.5% Morisky; 43.3%, MARS). Despite using optical aids, few (3%) with VI could read medication information clearly; 24% had difficulty distinguishing different tablets. More people with VI (29%) than controls (13%) (odds ratio [OR] = 2.8; 95% confidence interval [CI] = 1.6 to 5.0) needed help managing their medication, from friends (19% versus 10%) or pharmacists (10% versus 2.5%; OR = 4.4, 95% CI = 1.4 to 13.5); more received social service support (OR = 7.1; 95% CI = 3.9 to 12.9).
Conclusion Compared to their peers without VI, older people with VI are more than twice as likely to need help in managing medication. In clinical practice in primary care, patients’ needs for practical support in taking prescribed treatment must be recognised. Strategies for effective medication self-management should be explored.
INTRODUCTION
Visual impairment (VI) constitutes a major public health burden.1 Its prevalence is rising and is greater among older people, predisposing to difficulty in practical daily living activities,2 reduced quality of life,3 and increased morbidity, including falls,4 depression,5 suicide,6 and cognitive decline.7 Optimal health outcomes are associated with people’s ability to self-manage illness.8 Many older people require long-term complex therapies for the management of multiple chronic diseases: medication adherence is of key importance in optimising the overall effectiveness of their health care.9,10 Those with reduced visual acuity may be at particular risk of medication non-adherence, with potential adverse consequences for their health, but little is known about the impact of visual impairment on medication self-management. Medication non-adherence in older people has not been well described.10
The use of prescription drugs is rising in both the US and the UK: over 90% of those aged >65 years take at least one prescription medication long term and almost 50% take three or more.11,12 However, recent estimates indicate that, in the developed world, only approximately 50% of patients with chronic disease adhere to treatment recommendations.13 Various predictors of adherence have been identified, including the complexity and costs of treatment, characteristics of the illness, and personal factors,13 such as physical dependency,14 concerns about medicines,9,15 and social support.15 GPs are the key coordinators in prescribing in primary care.16 Their role in understanding patients’ problems and ensuring that management plans are appropriate, is fundamental in promoting medication adherence and optimising outcomes. The extent to which individuals with VI, compared to their peers with normal sight, require or receive support in managing medication has not been reported but has potentially important implications for prescribing in primary care. Therefore, this study aimed to compare levels of medication adherence between older people with and without VI, and to examine issues related to their management of their medication.
METHOD
Participant recruitment
Individuals aged ≥65 years, who attended the regional multidisciplinary low-vision clinic at the Royal Victoria Hospital, Belfast, and peripheral outreach clinics in Northern Ireland, were identified. They were sent information about the study, in large print, with a routine clinic appointment, and offered the information in audio format. At the clinic, the optometrist invited participation from those taking two or more different long-term oral medications daily, living within the community, not receiving daily medical or nursing care, and not participating in other research. For those who agreed, the optometrist recorded post refraction best corrected distance and near visual acuities (BCVA) using Bailey Lovie distance, and near-text reading charts.17 Visual impairment was defined by the World Health Organization (WHO) classification — BCVA <6/18 and >3/6018 — and those with BCVA outside these limits were excluded. Thus, all had some usable vision and were given optical aids, including spectacles.
How this fits in
Visual impairment is an increasing health problem, particularly among older people, and contributes to comorbidities that require long-term medication in primary care. Little is known about the impact of visual impairment on medication adherence or self-management. This study shows that almost 30% of older people with defined visual impairment need help in managing their medication, despite using optical aids; they are more than twice as likely as their peers without impaired vision to receive help from friends or statutory services. To ensure optimal health outcomes, clinicians must ask about problems with vision and check that appropriate support is available for individuals to take their medication as prescribed.
Primary care community optometrists recruited the control (C) group. They invited people aged ≥65 years to participate if they were taking two or more long-term oral medications daily, living in the same localities as those recruited with VI (to ensure availability of similar services), not requiring daily medical or nursing care and, had a BCVA of 6/9 or better. VA was measured using standardised optometry instrumentation and the same protocol as in the low-vision clinics. Anonymous data about those who declined to participate were recorded.
Data collection
All participants were visited at home (April 2007 to February 2010), where cognitive function was assessed (12-item Clifton Assessment Schedule) (CAS)19 and a researcher administered a bespoke questionnaire to gather information about living arrangements, educational status, falls, social support, and use of health and social care services. A measure of socioeconomic status was derived from participants’ postcodes (Multiple Deprivation Measure [MDM]):20 possible scores range from 1 to 890 and lower scores indicate greater deprivation.
Self-reported medication adherence was assessed by two validated measures, the Medication Adherence Report Scale (MARS; five questions about non-adherence behaviours, responses to each on a five-point scale)21 and Morisky Scale22 (four questions, yes/no responses). Beliefs about medication were examined using questions based on constructs linked to the health belief model23 and theory of planned behaviour.24 Quality of life (QoL) was assessed using validated generic (Short Form 12 [SF-12],25 EuroQol 5D [EQ-5D]26) and vision-specific (Daily Living Tasks associated with Vision [DLTV])27 questionnaires. Questions were asked about the use of optical aids, handling medications, and reading medication-related information.
With participants’ consent, for a randomly selected 10% sample, prescribing data were collected from GPs and dispensing data from community pharmacists for 6 months prior to their home visit, to attempt to verify self-reported adherence. A continuous multiple-interval measure of medication availability (CMA) was calculated for three medications for each patient (cholesterol lowering, antihypertensive, and one other), by dividing the intended prescription duration (days) by the observation period (or number of days between fills) and multiplying by 100. Scores below 80% were considered to indicate non-adherence; scores above 120% were considered over-adherent.28
Sample size and statistical analysis
Based on previous reports,29 it was estimated that a sample size of 150 per group would allow detection of 15% difference between groups in reported adherence, with 90% power, 0.05 alpha and two-tailed testing. Data were analysed using SPSS for windows (version 17). Independent-sample χ2-tests were used to examine differences between groups in parametric variables, following testing for normality of distribution; 2 tests were used to compare categorical data; and differences in non-parametric data were analysed using Mann–Whitney U tests. Associations between adherence scores and other variables were sought using regression analysis. Differences between groups in numbers having falls, contacts with health and social care services, and medication management were compared by calculating odds ratios (ORs).
RESULTS
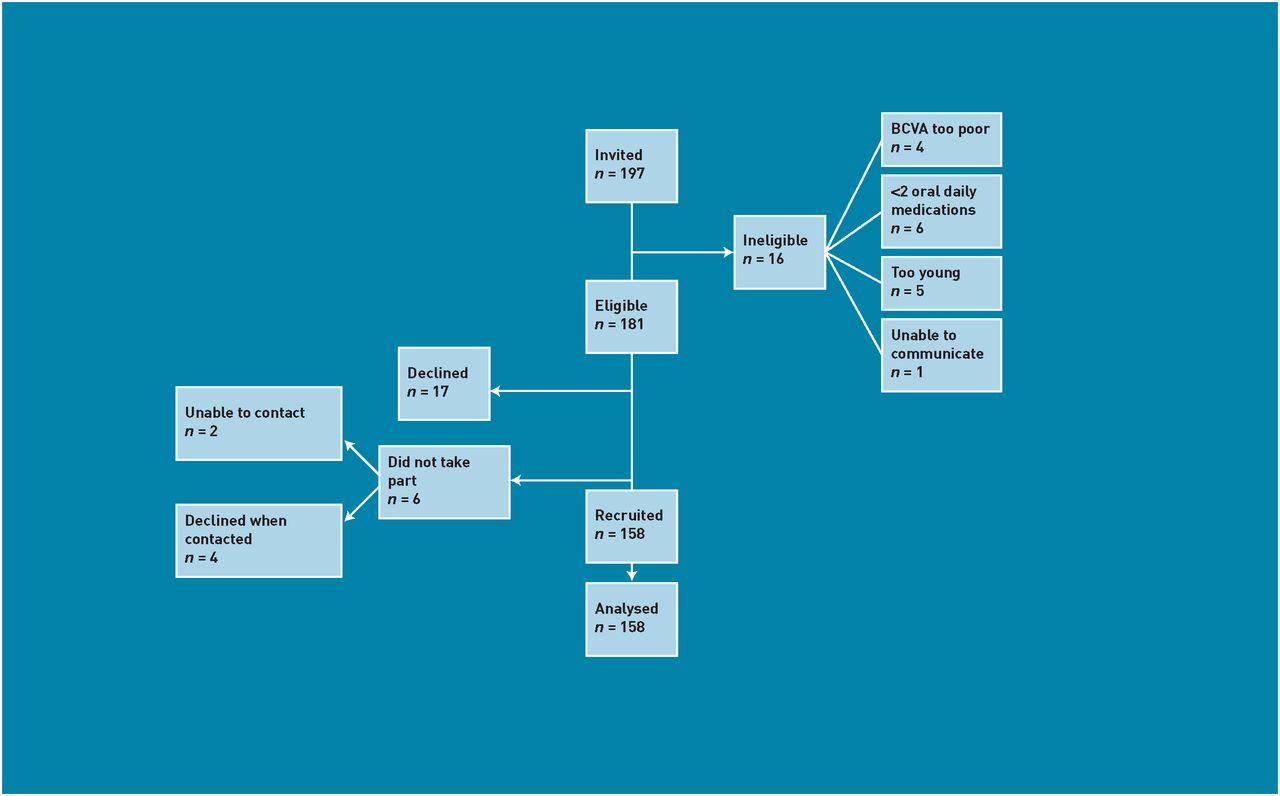
Of the 893 individuals who were sent study information, for 178 their appointment was cancelled, either by the hospital or by the patient; a further 132 did not attend. Of the remainder, 372 failed to fulfil the inclusion criteria (Figure 1); 211 were eligible, 73.9% (156/211) participated. Community optometrists identified 197 potential controls; 181 met the inclusion criteria, 87.3% (158) participated (Figure 2).

Flowchart for participants with visual impairment. aIncludes illness and changed caring or nursing arrangements. BCVA = best corrected visual acuity.

{kind=link}
{kind=link}
Flowchart for participants in the control group. BCVA = best corrected visual acuity.
Participant characteristics
Participants’ ages ranged from 65 to 101 years. The mean age of those with VI was higher than that of controls (81.0 versus 77.8 years, P<0.001) (Table 1); more with VI (33%; n = 51) were aged ≥85 years, compared to controls (15%; n = 23). No cognitive impairment was identified in any participant. There were no significant differences between groups in sex distribution (62.7% female), socioeconomic status (mean MDM score 300, standard deviation [SD] = 205), or living arrangements (88.9% lived in their own home; 46.8% lived alone). The groups had similar educational backgrounds: the majority (65.9%, n = 207) had received only primary school education.
Demographic characteristics, living arrangements, recent falls, and service use by study participants in visually impaired and control groups and the total sample
Falls, social services support and family physician contact
More of the group with VI (26.9%) than controls (8.9%) reported at least one fall during the previous 6 months (OR = 3.8; 95% confidence interval [CI] = 2.0 to 7.3; after adjusting for age, OR = 3.9; 95% CI = 2.0 to 7.6) (Table 1). The groups did not differ significantly in numbers of contacts with their GP; most had consulted at least once in the previous 6 months. Of those with VI, more (46%) reported contact with social care services in the previous 6 months, compared to controls (10.8%) (OR = 7.1; 95% CI = 3.9 to 12.9; age-adjusted OR = 6.6; 95% CI = 3.6 to 12.1). Most individuals who had such contact received ongoing service support in dressing, personal hygiene, preparing meals, or housekeeping, but not for taking medication. Multiple regression analysis showed no association between contact with services and age or living arrangements.
Medications, adherence and management
Individuals in both groups were prescribed similar numbers of medications (range = 2–14; mean = 5.1, SD = 2.5) and types of medications, suggesting similar comorbidity in each group. Overall, 93.3% (293/314) were prescribed cardiovascular medication, 16.6% (52/314) antidiabetic medication, 18.5% (58/314) psychotropic medication, 32.8% (103/314) analgesic medication, and 37.9% (119/314) gastroprotective medication.
No differences were found between the groups in mean adherence scores. Both scales indicated that approximately half of the participants were fully adherent (MARS: 43%; Morisky: 52%); a minority reported poor adherence. CMA scores also indicated high levels of adherence for both groups (overall mean scores: VI = 105.2 [SD = 26.0], C = 103.9 [SD = 14.2]; mean difference = 1.3, 95% CI = –3.3 to 5.9).
Significantly more with VI (29%), compared to controls (13%) (OR = 2.8 [95% CI = 1.6 to 5.0]; age-adjusted OR = 2.6 [95% CI = 1.4 to 4.7]) relied on help to take their medication each day or to sort it into a compliance aid (a container holding usually seven daily aliquots of medication, each within separate sections). Both groups used compliance aids (VI: 40%; control: 36%) but community pharmacists dispensed medications in these for more of the VI group (10% versus 2.5%) (OR = 4.4 [95% CI = 1.4 to 13.5]; age-adjusted OR = 3.8 [95% CI = 1.2 to 12.0]). Compared to controls, more individuals with VI relied on help from relatives or friends (19% versus 10%). Almost all (97%) with VI had difficulty reading medication labels, despite 80% using optical aids; 24% had difficulties distinguishing tablets, particularly in differentiating colours, compared to none of the controls. Almost half of each group had difficulties opening medications, especially blister packages. These results are summarised in Table 2.
Medication adherence questionnaire scores and medication management for visually impaired and control groups and the total sample
Beliefs and quality of life
Table 3 shows summary statements for questionnaire items representing health beliefs regarding medication. To mitigate the risk of over-reporting statistical significance when running multiple tests, a significance level of 0.01 was applied. While there were several statistically significant differences between the groups, only the ‘fear/anxiety’ item demonstrated a difference in mean scores of more than one unit, suggesting that the effect size for other differences is small. Thus participants with VI reported a significantly higher level of anxiety about becoming ill if they did not take their medication as prescribed.
Health Beliefs Questionnaire: scoresa for summary statements for visually impaired and control groups
Quality of life (Table 4), measured by the SF-12 (physical and mental health components) and EQ-5D, was worse for participants with VI than controls. The DLTV questionnaire, relating to performance of tasks requiring visual acuity, showed that those with VI reported significantly greater difficulties.
Quality of life, measured by SF-12, EQ-5D and DLTV questionnaires, for visually impaired (VI) and control (C) groups
DISCUSSION
Summary
These findings indicate that, while older people with and without VI achieve similar levels of medication adherence, those with VI require and receive significantly more support in medication self-management: they were more than twice as likely to require help and four times as likely to receive support from a community pharmacist. Almost 30% of participants with VI required help daily in taking their prescribed medication: despite using optical aids, almost all had difficulty reading information. Compared to their peers, significantly more with VI had difficulty distinguishing between medications but almost half of both groups had difficulties opening packaging. This report provides novel information about people with defined levels of VI, and indicates that the impact of VI on medication self-management should be considered when planning health and social care.
Strengths and limitations
The study achieved a high level of participation from all those identified as eligible, and the study groups were well matched in sex, prescribed medications (suggesting comparable comorbidity) and socioeconomic status, thus suggesting that the findings are not biased by these factors. Fewer individuals aged >85 years were recruited from community optometrists than from low-vision clinics but the characteristics of the participants with VI were similar to those described previously,30 suggesting that a representative sample was recruited: they reported more falls4,31 and poorer quality of life2,32 than their normally sighted counterparts. The sample reported levels of adherence that were similar to those reported previously for people with chronic disease in the developed world,13,29 so the findings of this study are likely to be generalisable.
In assessing adherence, there is no ‘gold’ standard:13 best practice is to use a multi-method approach. The study used two validated self-report questionnaires and an objective, although indirect, measure, based on community pharmacy and GP records. Self-report may overestimate adherence, but this study’s triangulation of measures provides robust data. Nonetheless, by selecting those who attended appointments, the sample may be biased towards adherence: those who miss appointments and decline to participate in research may be less adherent to prescribed treatment. However, this does not alter the finding that while similar adherence behaviour was reported by both groups, those with VI needed significantly more assistance.
Comparison with existing literature
There are few reports of levels of adherence to long-term therapies in general practice. This work adds to a previous report of older people with a range of self-reported vision impairments:33 its finding of a smaller proportion (10.8%) reporting difficulty managing medication may be because it included people with minor visual deficits, potentially corrected by spectacles. The study has defined participants’ visual acuity and described the problems experienced and help received, thus informing future strategies for medication self-management that should improve healthcare access for people with VI.34
Use of social care services was greater among those with VI. However, individuals mostly relied on informal social and family networks for help in managing medication. Older Australians have reported increased reliance on community and family support services as their VI increased.30 VI adversely influences people’s ability to care for themselves and their dependents.35 As society ages and VI increases in prevalence, sources of informal support for those needing help will become less and a need for other resources will increase. Multimodal interventions are likely to be required: recognising patients’ problems is the initial step in relevant intervention design.36
Major problems relating to pharmaceutical packaging have been reported.37 Lack of standardisation in packaging can cause confusion, particularly for older people, and is a barrier to their self-management. Several participants’ ‘coping strategies’, including memorising medications by touch, shape, or colour, were upset when, with generic prescribing, the size, shape, and colour of tablets and/or packaging varied for prescriptions dispensed on different occasions. There is a need for pharmaceutical companies and policy-makers to engage more with patients, to determine cost-effective ways of minimising problems due to different generic preparations of the same medicine, and to design more accessible packaging (while recognising child safety issues).
Health beliefs are significant predictors of medication adherence.13 The study participants with VI reported fear of the consequences of not taking medication as prescribed, a feeling that may contribute to their poorer quality of life. Recognising their need for support in medication management is important.
Implications for research and practice
This study was set in the context of the UK NHS, within which the potential influences of costs of treatment and services on medication adherence are removed, as these are free at the point of care. However, the findings indicate an insidious rising tide of need for help in medication self-management, as the numbers of older people with VI increase. Healthcare professionals should ask patients about their vision,34 and check that they have sufficient support in opening packaging, distinguishing tablets, measuring liquids, or using eye drops or injections. Practical help may include providing more accessible information through large-print labels, different textures and shapes of containers,38 electronic devices with pre-recorded voice messages (‘talking labels’), devices for scanning labels and converting to audio format (‘pen-friends’), syringe-filling aids, and ‘pillboxes’ with medication packed in daily quantities. Clinicians’ and pharmacists’ awareness of solutions to patients’ problems should prompt them to inform policy-makers and pharmaceutical companies regarding ways to improve their health care, recognising the associated cost implications for commissioning of future services. Further research, exploring how best to address their needs, is warranted, to avoid potential adverse health consequences from non-adherence to prescribed medication, and to inform strategies for cost-effective support programmes.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
Acknowledgments
The authors wish to thank the Royal National Institute for the Blind (RNIB) for their support and oversight of the study and The Blind Centre for Northern Ireland for their initial involvement in it; optometrists in low-vision clinics and in the community for recruiting participants; the NI Clinical Research Network (Primary Care and Vision) for facilitating data collection; and participants’ family physicians and pharmacists, for providing access to prescribing data. We also thank Ms Pat Hart (Consultant Ophthalmologist, Royal Group of Hospitals, Belfast), Dr Drew Gilliland (Senior Lecturer, General Practice, Queen’s University, Belfast), Mr David Bickerstaff (Belfast Health and Social Care Trust), Mr David Mann (RBNI), and Mrs Karen Toogood (RBNI) for their valued contributions to the Study Steering Committee.
Notes
Funding
The study was funded by The Big Lottery Fund.
Ethical approval
The Office of Research Ethics Committees (Northern Ireland) approved the study (Reference Number: 06/NIR01/140).
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
- Received January 11, 2012.
- Revision received March 14, 2012.
- Accepted March 22, 2012.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

