


Abstract
Background Chronic obstructive pulmonary disease (COPD) is common. Telehealthcare, involving personalised health care over a distance, is seen as having the potential to improve care for people with COPD.
Aim To systematically review the effectiveness of telehealthcare interventions in COPD to improve clinical and process outcomes.
Design and setting Cochrane Systematic Review of randomised controlled trials.
Methods The study involved searching the Cochrane Airways Group Register of Trials, which is derived from the Cochrane Central Register of Controlled Trials, MEDLINE®, embase™, and CINAHL®, as well as searching registers of ongoing and unpublished trials. Randomised controlled trials comparing a telehealthcare intervention with a control intervention in people with a clinical diagnosis of COPD were identified. The main outcomes of interest were quality of life and risk of emergency department visit, hospitalisation, and death. Two authors independently selected trials for inclusion and extracted data. Study quality was assessed using the Cochrane Collaboration’s risk of bias method. Meta-analysis was undertaken using fixed effect and/or random effects modelling.
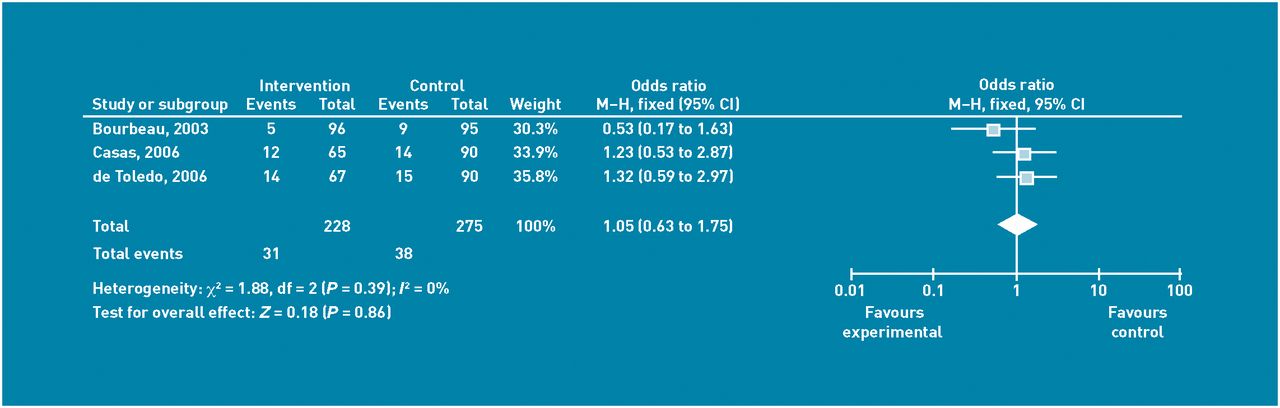
Results Ten randomised controlled trials were included. Telehealthcare did not improve COPD quality of life: mean difference –6.57 (95% confidence interval [CI] = –13.62 to 0.48). However, there was a significant reduction in the odds ratios (ORs) of emergency department attendance (OR = 0.27; 95% CI = 0.11 to 0.66) and hospitalisation (OR = 0.46; 95% CI = 0.33 to 0.65). There was a non-significant change in the OR of death (OR = 1.05; 95% CI = 0.63 to 1.75).
Conclusion In COPD, telehealthcare interventions can significantly reduce the risk of emergency department attendance and hospitalisation, but has little effect on the risk of death.
INTRODUCTION
At present, there are only a limited number of effective pharmacological interventions for chronic obstructive pulmonary disease (COPD).1,2 It is against this background that interest in telehealthcare models of care, which involve care for patients from a distance, have captured policy interest. It has been suggested that telehealthcare will help manage the burden of COPD by making health care more efficient,3 often by incorporating a degree of service redesign.4
Telehealthcare is attracting a considerable amount of investment globally; therefore, it is important and timely to scrutinise the evidence for telehealthcare in COPD and to look to resolve uncertainty regarding the effectiveness of such interventions.5,6 The objective of this study was to systematically review the effectiveness of telehealthcare interventions for people with COPD in improving quality of life and reducing emergency department visits, hospitalisations, and mortality. This report is a synopsis of the recently published Cochrane Review.7
METHOD
Participants
Researchers were interested in studies involving participants with clinician-diagnosed COPD. Studies could be based in primary care, secondary care, or intermediate care settings. No exclusions were made on the basis of participants’ sex, ethnicity, or language spoken.
Interventions
Miller’s conceptualisation of telehealthcare was adapted to define it as ‘the provision of personalised health care from a distance’.8 This definition encapsulates the following key considerations:
Information is obtained from individual patients; for example, in the form of a symptom score, oxygen saturation level, pulse rate.
These data are transmitted over a distance by information and communication technology.
A healthcare professional then exercises their clinical skills and judgement in interpreting this information and actively provides the patient with personalised feedback.
Self-care technologies, self-education, and websites without professional feedback were excluded. This study aimed to concentrate on interventions with an emphasis on ‘personalised’ or ‘tailored’ health care. This required a focus on patient–professional interactions enabled by distance communications technologies. Telehealthcare includes active professional feedback to patients, and excludes passive, automated feedback.9
Telehealthcare encompasses both synchronous (for example, telephone, mobile phone) and asynchronous communication modalities (for example, e-mail and text message). The synchronous approaches allow real-time communication between patient and professional, whereas asynchronous approaches enable patient data to be stored in packages and forwarded at specified intervals (for example, once a week) for review by the healthcare professional.
How this fits in
Chronic obstructive pulmonary disease (COPD) is increasingly common and now poses a substantial health problem in many parts of the world. Governments and industry are optimistic that telehealthcare will help manage the care burden of these people. This study found consistent evidence that telehealthcare helps people with COPD stay out of emergency departments and hospitals. Telehealthcare did not appear to affect the death rate or patients’ quality of life.
Comparisons
Control groups varied across the different studies in terms of the frequency and intensity of clinical contact provided. Most often, control groups featured ‘usual care’ although in some instances this included regular face-to-face home visits.
Design
Researchers stipulated that eligible study designs must randomise individuals/groups to the telehealthcare intervention of interest or control.
Outcomes
Data were gathered on a variety of process and clinical outcomes. Primary outcomes of interest were: quality of life scores, the number of patients with one or more emergency department visits over 12 months, the number of patients with one or more hospitalisations over 12 months and numbers of deaths. Other outcomes of interest were patient satisfaction, costs, and forced expiratory volume in 1 second (FEV1).
Protocol
Researchers specified the search strategy, study quality assessment methods, and approaches to synthesising data in a protocol, which was published in the Cochrane Database of Systematic Reviews.10
Searching for studies
The study involved searching the Cochrane Airways Group Register of Trials, which is derived from systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials, MEDLINE®, embase™, Cumulative Index to Nursing and Allied Health Literature (CINAHL®), and other electronic sources. Manual searches of respiratory journals and meetings’ abstracts also contribute to the register. All records in the register that had been coded as ‘chronic obstructive pulmonary disease’ were searched using the telehealthcare terms specified in the search strategy, published by Cochrane.7
Researchers contacted the authors of the identified articles and asked them to identify other published and unpublished randomised controlled trials. Authors searched the UK’s National Research Register(http://www.nihr.ac.uk/Pages/NRRArchive.aspx). References of the included trials were searched to find further randomised controlled trials; as well as additional registers of ongoing and unpublished trials: ClinicalTrials.gov (www.clinicaltrials.gov), Current Controlled Trials (www.controlled-trials.com), and the Australian New Zealand Clinical Trials Registry (www.anzctr.org.au).
Selection of studies
Using an agreed definition of telehealthcare, two authors screened the titles and abstracts to obtain a list of potentially eligible studies. Researchers obtained full-text copies of these studies and reached agreement through discussion regarding the final list of studies for inclusion. If agreement could not be reached, a third reviewer arbitrated.
Data extraction
The following data were extracted from the included studies and then independently verified by a second reviewer: country and setting; study design; the number of participants; a description of the telehealthcare intervention; a description of the control group; outcomes assessed and outcome data; proportion of patients with follow-up data; any harms or adverse effects.
Assessment of risk of bias
The study used the approach from The Cochrane Handbook for Systematic Reviews of Interventions, section 611 to assess the risk of bias in each trial using the following criteria:
Was the allocation sequence adequately generated? For example, by computer randomisation.
Was allocation adequately concealed? For example, by sealed envelopes.
Were the patients and researchers blinded to the allocated interventions?
Were incomplete outcome data adequately addressed? For example, were all patient withdrawals accounted for?
Were study reports free of any suggestion of selective reporting?
Was the study apparently free of other problems that might cause bias?
Analysis and data synthesis
Summary statistics for primary outcomes were calculated where there were sufficient data to pool outcomes. Mean difference for available quality of life scores were calculated, as well as odds ratios (ORs) for other variables using fixed effect meta-analysis in the absence of significant heterogeneity (I2<40%) and random effects meta-analysis where significant heterogeneity was present. Pooled data were presented graphically as Forest plots. The information that could not be pooled in meta-analysis was narratively summarised.
RESULTS
Searches revealed 220 potentially relevant studies. Following review of titles and abstracts, full text of 48 reports were obtained for appraisal of relevance and quality. Finally, 10 trials were selected,12–21 published in 12 reports12–23 (Figure 1) studying a total of 1004 patients.

PRISMA flow diagram showing selection of studies.
Description of studies
A summary of the key characteristics of all 10 trials is given in Table 1.12–21 Some of the studies14,16,17,20 relied on videoconferencing or telephone communication to set up ‘virtual consultations’, sometimes in addition to face-to-face consultations. Key outcomes of emergency department visits and hospitalisations were studied across most studies, but only those four studies which investigated a period of 12 months contributed to meta-analysis.12–14,19
Description of characteristics of included studies
Risk of bias
A summary of the risk of bias in the included studies can be found in Table 2.
Cochrane risk of bias rating
Effectiveness of telehealthcare
Results regarding the effectiveness of the interventions on outcomes from all studies are summarised in Table 3.
Results from the 10 included trials
Impact on quality of life
Two studies12,13 reported health-related quality of life using the validated St George’s Respiratory Questionnaire (SGRQ). Negative change on this questionnaire’s scale indicates improvement; the minimal clinically significant difference in health status is a change of four points.24 Meta-analysis (Figure 2) of these studies revealed a potentially important clinical improvement of –6.57 (95% CI = –13.62 to 0.48), but this pooled estimate was imprecise: the wide 95% CI indicated there was insufficient evidence to demonstrate clear benefit. A third study18 used the validated Chronic Respiratory Questionnaire (CRQ). Given concerns about the appropriateness of pooling these data with those derived from the SGRQ, it was decided not to include these data in the meta-analysis.25 After 6 months of this study18 the difference across the control and intervention group in CRQ scores was not significant.
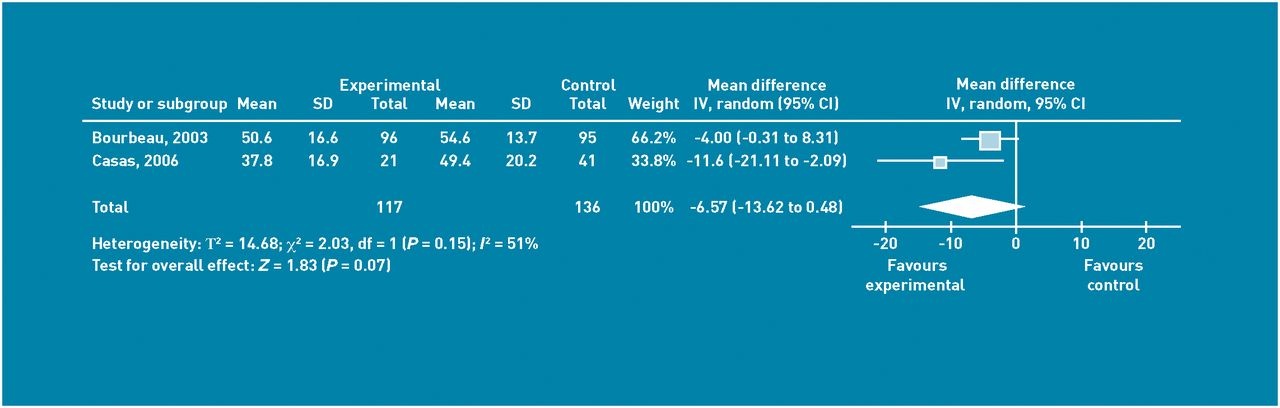
Mean difference between groups at end of 12 months according to St George’s Respiratory Questionnaire for COPD-related quality of life. Random effects analysis.
Emergency department visits
Three studies12,14,19 reported data on emergency department visits over 12 months. Intervention group patients were significantly less likely to attend the emergency department than patients in the control group: OR 0.27 (95% CI = 0.11 to 0.66; Figure 3).

Numbers of patients with one or more visits each to the emergency dept over 12 month period of study. Random effects analysis. M-H = Mantel Haenszel odds ratio.
Hospitalisation
Four studies12–14,19 reported on hospitalisations. The number of patients with one or more hospital admissions during the 12-month period of follow-up in these trials was significantly lower in the intervention group: OR 0.46 (95% CI = 0.33 to 0.65; Figure 4).
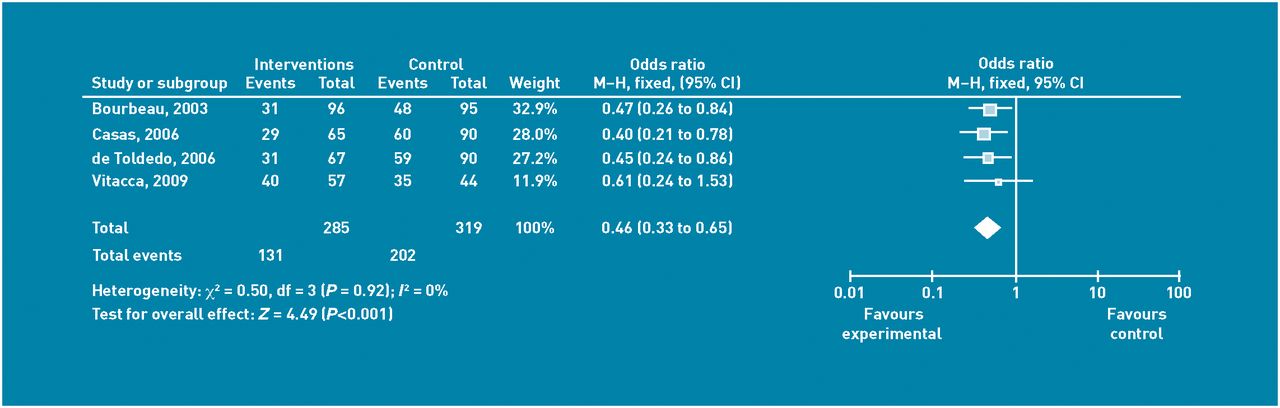
Number of patients with one or more hospitalisations over 12 months. Fixed effects analysis. M-H = Mantel Haenszel odds ratio.
Another study21 reported that there was insufficient evidence of a difference between telehealthcare follow-up and the control group in hospitalisation rates at 3 months (P = 0.182). In addition, one study16 examined the outcome measure of ‘discharge to a higher level of care’ (hospital or nursing home), and found that telehealthcare intervention patients were less likely to be discharged to a higher level of care than usual care patients OR 0.29 (95% CI = 0.08 to 1.05), but this result was again imprecisely estimated.
Death
In terms of deaths, the Vitacca et al study19 included data from patients who did not have COPD; however, when stratified for diagnosis, mortality rate did not differ between the two arms of the study. The best estimate comes from a pooled fixed effect meta-analysis which was undertaken with data from three studies12–14 to give OR 1.05 (95% CI = 0.63 to 1.75), an imprecise estimate close to no effect (Figure 5). The only other study16 which included deaths reported no statistically significant difference in mortality between the groups; however, raw data were not available for this study and so these were not included in the meta-analysis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Deaths over 12 months in the control group and telehealthcare group of the studies. Fixed effects analysis. M-H = Mantel Haenszel odds ratio.
Other outcomes
Exacerbations
Only the Bourbeau et al12 study recorded the total number of exacerbations of COPD. Over the 12 months of follow-up, there were 362 exacerbations in the control group (n = 95) and 299 exacerbations in the intervention group (n = 95). The between group difference was significant, favouring intervention: relative risk 0.83 (95% CI = 0.74 to 0.92).
Secondary outcomes
Patient satisfaction data showed that patients were largely satisfied with telehealthcare as long as they could have a face-to-face consultation on request. FEV1 was recorded in two studies and did not show a significantly different increase from start of trial to trial end across the two arms of the trials.
Discussion
Summary
There was consistent evidence that the numbers of visits to the emergency department and also the number of hospitalisations were significantly reduced with telehealthcare over 12 months. In terms of quality of life, the evidence was inconclusive as the confidence intervals were wide.12–14,18 There was evidence of almost no effect on the OR of mortality.
Strengths and limitations
The main strength of this review is its broad search strategy designed with the Cochrane Airways Group to identify 10 completed and seven ongoing relevant trials. The definition of telehealthcare used was conceptual and consistently applied: all included studies thus featured an interaction with a healthcare professional providing personalised feedback over a distance.
It can be challenging to decide whether or not to synthesise data quantitatively and, on balance, researchers thought it appropriate because the intervention approach that was being investigated; that is, facilitating personalised care from a distance was conceptually coherent thus making comparisons logical and consistent. An alternative approach would be to organise a series of reviews focusing on distinct technologies, but this was not the aim of the current study as, given that technologies are rapidly evolving and continually emerging, this would necessitate undertaking many separate reviews. Another potential limitation includes the possibility that the study did not uncover all relevant research.
Comparisons with literature
It is relevant to consider the meta-analysis in the Polisena et al26 review, where there is a transposition of the deaths in the Bourbeau et al12 study between the intervention and control groups which has a major impact on the mortality meta-analysis. Researchers of the current study have informed the authors of this. In addition, Polisena et al26 did not limit inclusion criteria to only randomised controlled trials and so there is a risk of bias from less methodologically rigorous studies.
A recent review by Bolton et al9 concentrated on telemonitoring in COPD and included interventions without the same degree of healthcare professional interaction that formed part of the inclusion criteria in the current study. They included both randomised and non-randomised studies which introduces a high risk of bias. They found only two randomised controlled trials, one of which was included in this study19 and the other trialled a self-management intervention27 which was excluded.
Implications for research and practice
Telehealthcare research for COPD needs to involve large scale trials with rigorous cost-effectiveness assessments built in. In this context, the full report of the results of the Whole System Demonstrator Project is eagerly awaited.28 Telehealthcare aims to keep those with COPD out of emergency departments and hospital. However, such a change may result in unintended consequences. For example, reducing the intensity of the care of such patients may be expected to impact unfavourably on the death rate. However, almost no evidence of this was found in the current meta-analysis (n = 503).
More qualitative research is also needed to help understand why particular interventions are (or are not) successful. Telecommunications technology should only be one element of the delivery of a substantially enhanced package of integrated chronic illness care.4 Successful interventions involve the provision of tailored and timely information to the individual. Personalised feedback from a healthcare professional is important. The telehealthcare models adopted in these studies often involved a mix of face-to-face and ‘virtual’ consultations with a specialist nurse or physiotherapist who had additional training in the management of COPD and who used a variety of techniques including early intervention, breathing exercises, and other elements of pulmonary rehabilitation to maintain patients’ health.
There has been much recent optimism regarding the potential for telehealthcare to reduce the cost of health care in patients with COPD. Although largely consistent, the studies in the review are small, with follow-up to only 12 months. Nonetheless, these data do indicate that telehealthcare-based models of COPD care can significantly reduce emergency department attendance and hospitalisation. The best evidence for telehealthcare involves redesigning the care pathway into a personalised interaction across a distance to deliver feedback from a healthcare professional in response to specific patient data. These benefits are still to be demonstrated when telehealthcare is implemented routinely on a larger scale.
Notes
Funding
Susannah McLean was supported by a National Health Service Education for Scotland Clinical Academic Fellowship in General Practice. Other support came from the NHS Connecting for Health Evaluation Programme (NHS CFHEP 001) and the Edinburgh Medical Research Council Trials Methodology Hub (G0800803). The funding agencies had no role in designing or conducting this study, the collection, management, analysis, and interpretation of the data, or the preparation, review, or approval of the manuscript.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
Susannah McLean has received an honorarium from Cumbria Trust for speaking and from the BMJ for writing about telehealthcare. Joseph LY Liu has worked on a Medicaid funded project on telehealthcare. All other authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received February 3, 2012.
- Revision received March 8, 2012.
- Accepted May 1, 2012.
- © British Journal of General Practice 2012
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

