


Abstract
Background Empathy as a characteristic of patient–physician communication in both general practice and clinical care is considered to be the backbone of the patient–physician relationship. Although the value of empathy is seldom debated, its effectiveness is little discussed in general practice. This literature review explores the effectiveness of empathy in general practice. Effects that are discussed are: patient satisfaction and adherence, feelings of anxiety and stress, patient enablement, diagnostics related to information exchange, and clinical outcomes.
Aim To review the existing literature concerning all studies published in the last 15 years on the effectiveness of physician empathy in general practice.
Design and setting Systematic literature search.
Method Searches of PubMed, EMBASE, and PsychINFO databases were undertaken, with citation searches of key studies and papers. Original studies published in English between July 1995 and July 2011, containing empirical data about patient experience of GPs’ empathy, were included. Qualitative assessment was applied using Giacomini and Cook’s criteria.
Results After screening the literature using specified selection criteria, 964 original studies were selected; of these, seven were included in this review after applying quality assessment. There is a good correlation between physician empathy and patient satisfaction and a direct positive relationship with strengthening patient enablement. Empathy lowers patients’ anxiety and distress and delivers significantly better clinical outcomes.
Conclusion Although only a small number of studies could be used in this search, the general outcome seems to be that empathy in the patient–physician communication in general practice is of unquestionable importance.
INTRODUCTION
Patients consider empathy as a basic component of all therapeutic relationships and a key factor in their definitions of quality of care.1,2 One hundred years ago, Tichener introduced the word ‘empathy’ into the English literature, based on the philosophical aesthetics concept of ‘Einfühlung’ of Theodor Lipps.3 Another important historical moment is the way Rogers speaks about empathy in 1961 in his book: On Becoming a Person: a Therapist’s View of Psychotherapy.4 Since then, various authors have written about empathy in the setting of psychotherapy and about its functionality in patient–physician communication. Neuroscientific research of recent decades has achieved significant progress in establishing the neurobiological basis for empathy, after discovering the mirror neuron system (MNS)5,6 as probably being related to people’s capacity to be empathic.7 Scientists have now added new insights, based on functional magnetic resonance imaging (fMRI) experiments. They have discovered that the MNS consists of mirror neurons in the ventral premotor cortex and the parietal area of the brain and neurons in the somatosensory areas and in limbic and paralimbic structures.8 The insula plays a fundamental role in connecting these regions.9 fMRI experiments have shown that individuals who score higher in a questionnaire measuring their tendency to place themselves in the other person’s shoes activate their MNS more strongly while listening to other people’s problems.10,11 These results draw the ‘soft’ concept of empathy into ‘hard’ science, which opens a challenging new field of research with potentially important clinical implications.12 However, these neurobiological studies do not give information about the impact of empathy in clinical care. Within the current opinion of ‘evidence-based health care’, it is important also to get evidence about the effectiveness of empathy in the daily practice of GPs.
To assess the effectiveness of empathy, it is necessary to define what authors mean when using the term ‘empathy’. Although many authors experience difficulties in giving a clear definition,1,2,13,–,20 a number of core elements can be identified. In general, authors consider empathy as the competence of a physician to understand the patient’s situation, perspective, and feelings; to communicate that understanding and check its accuracy; and to act on that understanding in a helpful therapeutic way. It has an affective, a cognitive, and a behavioural dimension.1,21,–,24
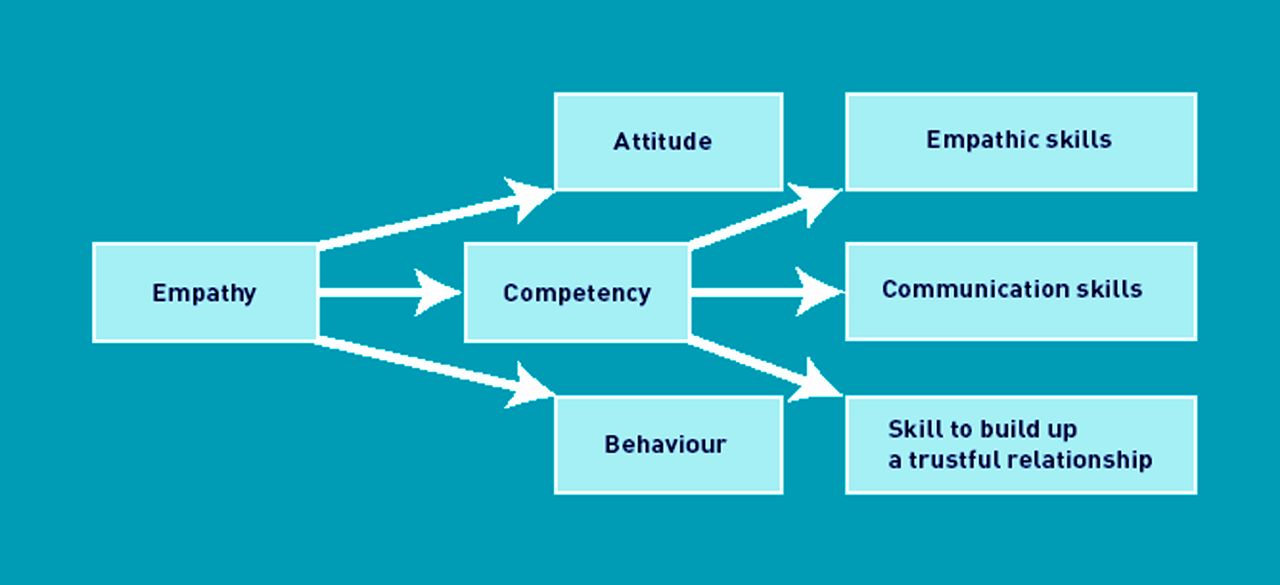
Empathy can therefore be defined at three levels: as an attitude (affective),25,26 as a competency (cognitive),2,15 and as a behaviour.2,16
Attitude is based on moral standards in the mind of the physician; such as respectfulness for the authenticity of the other person, interest in the other person, impartiality, and receptivity. These standards are formed by a physician’s own human development, their socialisation process, their medical training, their personal experience with patients; by reading professional literature; and by watching movies and reading books.13,15,22,27,–,29
How this fits in
Empathy is seen, as well as by patients as by physicians, as the base of good patient-physician communication. Despite these opinions one can see a decrease of interest in good patient-physician communication. There is an increase of technological aspects of care and of a prevalence on productivity in general practice. This systematic review shows that also a “soft” skill like empathy has its effectiveness on patient satisfaction, adherence, decrease of anxiety and stress, better diagnostics and outcomes and patient enablement. Physicians should be more aware of this. In the near future it is a challenge to draw the attention of policy makers and health insures on these aspects of empathy.
Competency can be subdivided into empathic skill, a communication skill, and the skill to build up a relationship with a patient based on mutual trust. Empathic skill is the approach by which the physician can elicit the inner world of the patient and get as much information as possible from the patient, while at the same time recognising the patient’s problem.2,30,31 Communication skill is used to check, clarify, support, understand, reconstruct, and reflect on the perception of a patient’s thoughts and feelings.15,23 The skill to build up a trusting and long-standing patient–physician relationship encourages physicians to resonate with the patient emotionally. These long-term relationships are important for telling and listening to the stories of illness.32,33
Behaviour has a cognitive and an affective part. The cognitive part includes verbal and/or non-verbal skills.14,15,22,25,26 The affective part includes recognition of the emotional state or situation of the patient, being moved, and recognising a feeling of identification with someone who suffers with anger, grief, and disappointment. After this recognition, the physician, in their behaviour, reflects on and communicates their understanding to the patient (Figure 1).20,23

Subdivisions of empathy.
Both patients and physicians mention empathy as the basis for a humane patient-centred method in general practice, and as an important component of professionalism.1,17,34 A large number of patients, nearly 80%, would recommend an empathic physician to other individuals.35
Despite these opinions, one can see a decrease of interest in good patient–physician communication. Reynolds et al report a low level of empathy in professional relationships.34 In their view, this is widespread in modern medicine and many recipients of professional help may not feel that their situation is understood by professionals.34 A study by Kenny et al suggests that physicians and patients have a different perspective on physicians’ communication skills: the perceptions of the medical encounter have been characterised as being so different that they appear to be from ‘different worlds’.36
Moreover, different authors report a rising prevalence in the last decade of technological and biomedical aspects of care and of more emphasis on effectiveness and productivity in family care.17,20,37Peabody proved to be prophetic when, in 1927, in his lecture The Care of the Patient, he expressed concern that rapidly growing scientific technology was crowding out human values in the management of patients.38 Just as Spiro asks attention for the ‘unseen and unheard’ patient in these developments,20 it is important to pay attention to the effectiveness of empathy in patient–physician communication.
The purpose of this literature review is to get a clear view on the proven effectiveness of empathy in patient–physician communication, in particular in general practice.
METHOD
A search was undertaken of PubMed, EMBASE, and PsychINFO databases, between July 1995 and July 2011, with the support of a professional librarian, to identify studies of general practice, empathy, and effectiveness or outcome of empathy. The search terms used are shown in Box 1. The search was performed using major medical subject heading (MeSH) terms in titles and/or abstracts (Box 1). After removal of duplicate studies, titles and abstracts were assessed as to whether the articles were pertinent to this literature review and whether they dealt with general practice. Potentially relevant articles were read in full text. Further papers were sought by checking references and citation searches of included and other leading articles (snowball method). After this selection, articles were assessed as to whether or not they fitted within the inclusion criteria.
Box 1. Database search terms used
((empathy[MeSH] OR empath*[tiab])) AND (Physicians, Family[MeSH] OR Primary Health Care[MeSH] OR Family Practice[MeSH] OR “General Practice”[MeSH] OR “General Practitioners”[MeSH] OR Family Physician*[tiab] OR Primary Health Care[tiab] OR Primary Healthcare[tiab] OR Primary Care[tiab] OR Family Practice*[tiab] OR General Practice*[tiab] OR General Practitioner*[tiab] OR Family Medicine[tiab]) AND outcome*[tw]
To fulfil the inclusion criteria, articles had to detail original and empirical studies, published in English. Studies had to contain patient experience, and outcome measures of empathy and measures of GPs’ empathy. Exclusion criteria were: reviews, guidelines, and theoretical or opinion articles. In the last selection, the studies were evaluated by the criteria of quality developed by Giacomini and Cook (Box 2).39 From the initial 964 papers, seven meeting the inclusion and qualitative criteria were identified (Figure 2).

{kind=link}
{kind=link}
Selection process for papers on the effectiveness of empathy in general practice.
Box 2. Giacomini and Cook’s criteria39
The participant selection is well reasoned and the inclusion is relevant to the research question; the population is representative.
The data-collection methods are appropriate for the research objectives and setting; the data collection is valid and reliable.
The data-collection process, which includes field observation, interviews, and document analysis, must be comprehensive enough to support rich and robust description of the observed events.
The data must be appropriately analysed and the findings adequately corroborated by using multiple sources of information.
RESULTS
Seven studies were found (Table 1).40,–,46 The effectiveness of empathy in patient–physician communication in the studies included is described as improvement of patient satisfaction and adherence, decrease of anxiety and distress, better diagnostic and clinical outcomes, and more patient enablement. Patient outcomes were measured by questionnaires and laboratory tests, and by analysing audio- and videotapes.
Summary of included articles
Improvement of patient satisfaction and adherence
Hojat et al found a good correlation between patients’ satisfaction and their perceptions of physicians’ empathic engagement.40 Corrected item–total score correlations of the patient satisfaction scale ranged from 0.85 to 0.96; correlation between patient satisfaction scores and patient perception of physician empathy was 0.93.40
Decrease of anxiety and distress
In the study by van Dulmen et al it was found that the more anxious patients were, the more adequately their GPs tended to respond. Patients who perceived their GP as empathic reported lower levels of anxiety.41
Better diagnostics and clinical outcomes
Levinson and Roter confirm that communication between physicians and patients is associated with underlying physician attitudes.42 Specifically, physicians with positive attitudes towards psychosocial issues make more statements expressing concern and empathy. The patients of these physicians offer relatively more information about psychological and social issues. These patterns of communication are associated with improved patient satisfaction and patient outcomes.42 An underlying attitude of genuine interest and empathy, within a continuing relationship, was highly valued. Patients described how the GP’s attitude helped or hindered them in discussing their problems. Patients also described how the GP helped them make sense of, or resolve, their problems and supported their efforts to change.43
Hojat et al found a positive relationship between physician empathy and patients’ clinical outcomes. Patients with diabetes had their glycosylated haemoglobin (HbA1c) and low-density lipoprotein (LDL) cholesterol levels checked. Both tests showed significantly better results in patients with a more empathic physician. It is suggested that more empathy in the physician–patient relationship enhances mutual understanding and trust between the physician and patient, which in turn promotes sharing without concealment, leading to a better alignment between patients’ needs and treatment plans, and thus more accurate diagnosis and greater adherence.44
Even the most common infectious disease on earth, a common cold, is shown to last for significantly less time and to be less severe in cases where there is good physician–patient empathy. A ‘physician empathy perfect group’ was associated with the shortest cold duration (5.89 days versus 7.00 days). The amount of change of interleukin-8 and neutrophil level was greater for the ‘physician empathy perfect’ group. Interleukin-8 and neutrophil counts were obtained from nasal wash at baseline and 48 hours later.45
More patient enablement
There is a direct positive relationship between GP empathy and patient enablement, as well as between enablement and changes in main complaint and wellbeing.46 Patient enablement was measured by the Patient Enablement Instrument (PEI), with questions on topics such as: ability to cope with life and illness, and patients’ confidence about their health and their ability to help themselves.46
DISCUSSION
Summary
This review investigates the relationship between GP empathy and patient outcomes. A GP’s daily practice involves many elements that are not evidence based. The existence and use of empathy in communication is one of these ‘soft’ elements. However, this review shows that there is empirical evidence for effects of human aspects in patient–physician interaction. There is a relationship between empathy in patient–physician communication and patient satisfaction and adherence, patients’ anxiety and distress, better diagnostic and clinical outcomes, and strengthening of patients’ enablement.
As mentioned in the introduction, there are different levels of empathy. Authors used different types of tests to measure these different levels, such as the Jefferson Scale of Patient Perceptions of Physician Empathy (JSPPPE), a self-report measuring scale for cognitive and attitude factors; the Consultation and Relational Empathy Measure (CARE), a patient rating system that measures physicians’ communication skills and attitudes; the Roter Interaction Analysis System (RIAS), an observer rating system that measures empathy skills; and the Tape Assisted Recall method (TAR), which measures the development of a long working relationship.47
Strengths and limitations
A previous review by Beck et al mentioned that actual empirical data were relatively scarce.48 With the inclusion criteria used in this review, seven articles were found with a bearing on general practice.
This study has a potential cultural bias in interpreting and judging phenomena by standards inherent to European culture. General practice in Europe is most commonly delivered by GPs. In the US, primary care includes both general internists and paediatricians, as well as GPs.
A possible limitation of this review is the underexposure of ‘the danger of empathy’, such as a physician losing their professional distance, which, in certain situations, might make empathy a less desirable aspect of patient–physician communication.16,49
In focusing on empathy, the effects of contextual factors on specific health outcomes are possibly underexposed, such as intrinsic and/or extrinsic factors, healthcare setting, access to care, GP’s workload or pressure, and sociocultural factors.50
General limitations of this review are that only articles written in English are included. Furthermore, the existing measures of empathy have been taken as presented in the literature; no critical reflection of the validity of these measures has taken place.
Comparison with existing literature
The results of the studies seem to be supported by other authors. For patient satisfaction and adherence, Neumann et al,21 Kim et al,51 and Lelorain et al52 confirm the data; they found links between physician empathy and patient satisfaction, in various clinical settings. Mercer et al have shown that patients view quality of consultation in general practice as related to both the GP’s competence and the GP’s empathic care.53 Further, Neumann et al argue that affective-oriented effects of empathy are related to more satisfaction, adherence, and trust.16 Indirectly, patients who are more satisfied with the care received exercise greater adherence to agreed and recommended treatment regimens and courses of action.3
In relation to decrease of anxiety and distress, in experimental research in which a GP was trained in special communication styles, Verheul et al found that combining a warm and empathic communication style with raising positive expectations leads to positive effects on the patient’s anxiety.12
In relation to better diagnostics and clinical outcomes, authors have shown that empathic communication achieves the effect that patients talk more about their symptoms and concerns, enabling the physician to collect more detailed medical and psychosocial information. This leads to more accurate medical and psychosocial perception and ultimately to more accurate diagnosis and treatment regimens.13,22 Neumann et al based their ‘effect model of empathic communication in the clinical encounter’ on this evidence.16 It has also been mentioned that patients’ overall satisfaction with healthcare services, adherence to medical regimens, comprehension, and perception of a good personal relationship are positively related with interpersonal communication between the patient and care provider and are particularly related to the physician’s empathic behaviour.24,48,51,54,–,57 However, physician-perceived stress has also been shown to correlate negatively with enablement.57
Implications for practice and research
Empathy is a familiar term in the helping and caring literature. In 2008, the World Health Organization (WHO) reaffirmed the importance of primary health care with its report Primary Health Care Now More Than Ever.58 The key challenge was ‘to put people first, since good care is about people’.58 Rakel said that good medical care will continue to depend on care by concerned and compassionate family physicians who can communicate with patients, understand them, know their families, and see them as more than a case.59
Qualitative studies show that physicians link empathy to fidelity, prosocial behaviour, moral thinking, good communication, patient and professional satisfaction, good therapeutic relationships, fewer damage claims, good clinical outcomes, and building up a trusting relationship with the patient.15,24,25,60,61 In her study, Shapiro explored how primary care clinician-teachers actually attempt to convey empathy to medical students; they argued that the moral development of the GP, their basic willingness to help, their genuine interest in the other, and an emphasis on the other’s feelings are basic principles for acceptance of the empathic approach to the patient.25
In GPs’ views, limiting factors during consultation are: time pressure, heavy workload, a cynical view on the effectiveness of empathy, and a lack of skill.13,51,62 Neumann et al have shown that patients also see time pressure and busyness on the physician’s part as a limiting factor.21
Thus empathy can be seen as a part of patient–GP communication, characterised by feelings such as interest and recognition and the physician remaining objective. However, barriers exist for implementation in general practice.13,14,24,30,31,47,63,64
Another finding of this review is that some studies suggest that the degree of empathy shown by medical students declines over the course of their training.20,65,66 Empathy appears to increase during the first year of medical school, but decreases after the third year and remains low through the final year of medical school, measured using the Jefferson Scale of Physician Empathy–Student Version (JSPE-S).17,66,67 In the study by Hojat et al,66 there are no sex differences. On the other hand, Quince et al discovered that among males during medical education, in both the bachelor and clinical phases, affective empathy slightly but significantly declined and cognitive empathy was unchanged. Among females, neither affective nor cognitive empathy changed.68 It is ironic that there are indications that when students can finally begin doing the work they came to medical school to do (that is, taking care of patients) they seem to begin losing empathy.69 Possible explanations of the decline are: a lack of good role models and changes in general cultural and ethical views on illness, health, and portrayals of mankind. Interviews with physicians show that they think that, in current western society, it has become less a part of human nature to be interested in another person and to be affected by someone else’s misery.17 In their study of American college students, comparing the temporal changes between 1979 and 2009, Konrath et al showed that this development has social roots.65 Considering these possible tendencies in education and the above-mentioned technological changes within the healthcare system, which probably influence the patient–physician alliance negatively and could undermine empathy in these relationships, it makes sense to emphasise the results of the present review. The evidence of a correlation between empathy and clinical outcomes should be made widely known, especially among medical students and physicians. Some authors already believe empathy can be improved by targeted educational activities and they indicate opportunities to enhance empathy during education.16,17,26,38,69,–,71
It should be mentioned that, until now, the widely acclaimed benefits of empathy only have a small empirical base. Although a few studies of sufficiently high quality show promising results, much more research is needed to claim the effectiveness of empathy in clinical practice on evidence-based grounds. Neumann et al have already highlighted the need for an examination of the cost-effectiveness of empathy in the light of the recent focus of policy makers and health insurers on the efficiency of health care.16 It is a challenge to draw the attention of policy makers to empathy as an effective and efficient way of delivering health care. A vast majority of patients want empathic physicians, particularly, but not exclusively, in general practice.72 Indirectly, authors suppose empathic behaviour improves the physician–patient relationship and causes satisfaction for the patient but also for the physician,1,13,22 resulting in fewer cases of compassion fatigue or burn out.
Further research is needed on the practical use of empathy in general practice, with a focus on the effects and side effects of empathy and the expectations of patients and GPs. In this context, it is important to take account of how researchers have measured empathy. Measuring empathy is often based solely on self-reports and is therefore often remote from patients’ and physicians’ concrete feelings, experiences, and interpretations in practice. Only patient-perceived empathy is significantly related to patient outcomes. Therefore, it appears best to use a patient-perceived empathy scale to measure physician empathy in practice.47,48,63,65,73
It is remarkable that empirical studies on physician empathy are still relatively scarce. According to the results of the studies included in this systematic review, empathy is an important factor in patient satisfaction and adherence, in decreasing patients’ anxiety and distress, in better diagnostic and clinical outcomes, and in strengthening patient enablement. Thus, physician empathy seems to improve physical and psychosocial health outcomes.
Acknowledgments
I am most grateful to E Peters, specialist librarian of the medical library, for her help with the database searches.
Notes
Funding
The study was not funded.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received February 26, 2012.
- Revision received April 12, 2012.
- Accepted June 28, 2012.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

