


Abstract
Background Physical activity and dietary change interventions can prevent or delay a range of chronic disease. Little is known in primary care about their effectiveness in South Asian populations, who are often at higher risk of developing such diseases.
Aim To assess evidence for effectiveness of primary care based physical activity and dietary interventions in South Asian populations, and identify methods to inform future intervention development.
Design Systematic review.
Method Intervention studies conducted in developed countries that reported data for South Asian adults were sought by searching electronic databases, trial registries, and conference proceedings. Following wider screening of titles and abstracts, 119 full articles were reviewed.
Result Of the 119 articles, four studies met the inclusion criteria and evaluated community-based interventions with South Asian individuals. Methodological quality was poor overall. Interventions appeared generally effective in promoting a decrease in weight, with some positive changes in blood pressure and biochemical outcomes, such as cholesterol. There was limited evidence for effects on behaviour. Theoretical frameworks were not identified and evidence on attitudinal or knowledge-based outcomes was sparse. The inclusion of individual feedback and community workers in communities of deprivation appeared important to the acceptability of the interventions. Information distinguishable for South Asian individuals within intervention studies of general populations was lacking.
Conclusion Physical activity and dietary interventions with South Asian populations show modest promise but, given the paucity of controlled evaluations or use of objective measures, outcomes are difficult to interpret. Potential insights may be missed if experience concerning South Asian groups within studies is not reported. Further development of culturally appropriate interventions that are theoretically informed and assessed in experimental designs are required.
INTRODUCTION
In developed countries, people of South Asian origin who are historically immigrant (including those of Indian, Pakistani, Bangladeshi, and Sri Lankan ancestral origins) have markedly higher and earlier mortality and morbidity from coronary heart disease (CHD) and type 2 diabetes, as well as their complications, than the general population.1,–,3 These contribute to extensive disability and suffering, as well as significant societal costs. For primary care, the greatest opportunity to address the personal and societal burden of such chronic disease is to prevent development of the disease or delay its onset in those, often socially disadvantaged, communities that are at highest risk and need.4
Although genetic factors contribute, lifestyle features strongly in the development of a range of chronic diseases.5 Well-documented risk factors for cardiovascular disease, diabetes, and cancer include physical inactivity, a diet that is high in fat and sugar, and obesity.3,6,7 A significant association is found between cardiovascular-protective behaviours and lower risk of all-cause and cardiovascular mortality on a national scale.8 Large international trials of intensive physical activity and dietary interventions have demonstrated long-term reductions in the development of type 2 diabetes for adults at higher risk.9,10 Several reviews on the effects of diet and exercise on the incidence of CHD and type 2 diabetes have emphasised their importance in the primary and secondary prevention of disease.11–13
With South Asian populations identified as less physically active than the general population,14,15 alongside growing concern about child and adult obesity,16 culturally appropriate and effective interventions in this high-risk group are urgently needed.17 However, little is known about relevant experience of such interventions with South Asian populations. This study aimed to systematically review current evidence to address two research questions:
Can community or primary care based interventions targeting physical activity and/or dietary change improve health outcomes in people of South Asian origin in developed countries?
Can culturally appropriate methods and theoretical models be identified from eligible studies to inform the development and delivery of future interventions?
METHOD
Study eligibility criteria were any community or primary care based intervention study conducted in a developed country that quantitatively evaluated the effectiveness of a physical activity and/or dietary change intervention in adult South Asian communities of people who were historically immigrant, or described inclusion of the latter in their samples and reported data identifiable for South Asian individuals. The search aimed to identify both randomised and non-randomised controlled studies, the latter including before and after, between-group designs. The search was limited to the English language.
How this fits in
Evidence for the impact of interventions promoting dietary change and physical activity is strong, particularly for diabetes, but less is known about their effectiveness in South Asian populations at high risk of developing chronic diseases. This systematic review suggests there is modest evidence that interventions with people of South Asian origin may improve weight loss, blood pressure, and blood lipid profiles, although there is little evidence for facilitating change in behaviour or knowledge. Community-based interventions involving bilingual link workers and using individual feedback, appear promising, especially within South Asian communities that are socio-educationally disadvantaged. The development of culturally appropriate interventions that are theoretically based and evaluated in high-quality experimental research is still needed to achieve effective health promotion in this high-risk group.
The following databases were searched from inception to January 2011: MEDLINE®, embase, CINAHL®, PsycINFO, Cochrane Database of Systematic Reviews, and DARE. Search strategies were designed for each database. The MEDLINE search strategy was developed using existing Cochrane search strategies and peer-reviewed by an information scientist (Box 1). Supplementary searches of online trial registries and conference proceedings were also conducted. Two reviewers independently inspected titles and abstracts of identified papers. The data extraction form was developed by two individuals, who independently reviewed the full-text articles of eligible studies; data extraction was undertaken by a third reviewer and the details were cross-checked by the first two individuals. Any disagreement on inclusion or data entry was resolved by consensus discussion.
Box 1. MEDLINE search strategy
1. exp Ethnic Groups/
2. exp Minority groups/
3. ethnic$.tw.
4. Bangladeshi$.tw.
5. Pakistani$.tw.
6. Indian$.tw.
7. exp Indians, North American/
8. 6 not 7
9. exp India/
10. 8 not 9
11. Asian$.tw.
12. South Asian$.tw.
13. Sri Lankan$.tw.
14. 1 or 2 or 3 or 4 or 5 or 10 or 11 or 12 or 13
15. exp African Americans/
16. exp Mexican Americans/
17. exp Hispanic Americans/
18. Hispanic$.ti.
19. 15 or 16 or 17 or 18
20. 14 not 19
21. exp Diet/ or exp Diet Therapy/
22. exp Feeding Behavior/
23. (diet$ or food choice$ or eat$).tw.
24. 21 or 22 or 23
25. exp Exercise/
26. exp Exercise Therapy/
27. exp Physical Fitness/
28. exp “Physical Education and Training”/
29. physical activit$.mp.
30. physical inactivit$.mp.
31. exp Sports/
32. exp Walking/
33. walk$.tw.
34. ((promot$ or uptak$ or encourag$ or increas$ or start$ or support$ or advi$) adj5((physical adj (activit$ or exercis$)) or exercis$)).mp.
35. 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34
36. exp Life Style/
37. (life style$ or lifestyle$).tw.
38. 36 or 37
39. exp Weight loss/
40. weight loss.tw.
41. 39 or 40
42. ((health$ adj6 (behav$ or educ$ or promot$))and (diet$ or exercis$ or physical activit$ orwalk$ or life style$ or lifestyle$ or weightloss)).mp.
43. 24 or 35 or 38 or 41 or 42
44. exp Primary Health Care/
45. exp Community Health Services/
46. exp Physicians, Family/
47. exp Family Practice/
48. (primary adj2 care).tw.
49. community.ab,ti.
50. 44 or 45 or 46 or 47 or 48 or 49
51. 20 and 43 and 50
52. animal/ not (human/ and animal/)
53. 51 not 52
From eligible studies, all effects of physical activity and dietary interventions were categorised into primary clinical outcomes and secondary outcomes of behaviour and psychological/knowledge-based change, which are meaningful in explaining clinical endpoints.18 Data were extracted in terms of the percentage of change from baseline to follow-up, and presented with the actual baseline value and level of statistical significance where available. Qualitative data on intervention acceptability were also extracted where available. The methodological quality of the studies was assessed using a validated quality index,19 based on the reporting of findings, validity, the extent of bias in measurement and outcome, and selection bias.
RESULTS
Study characteristics and quality assessment
The flow of studies through the stages of the systematic review is shown in Figure 1. Data distinguishable for South Asian individuals who were historically immigrant and were, or may have been, included in the samples of many studies was lacking. In total, only four studies were included in the final review.
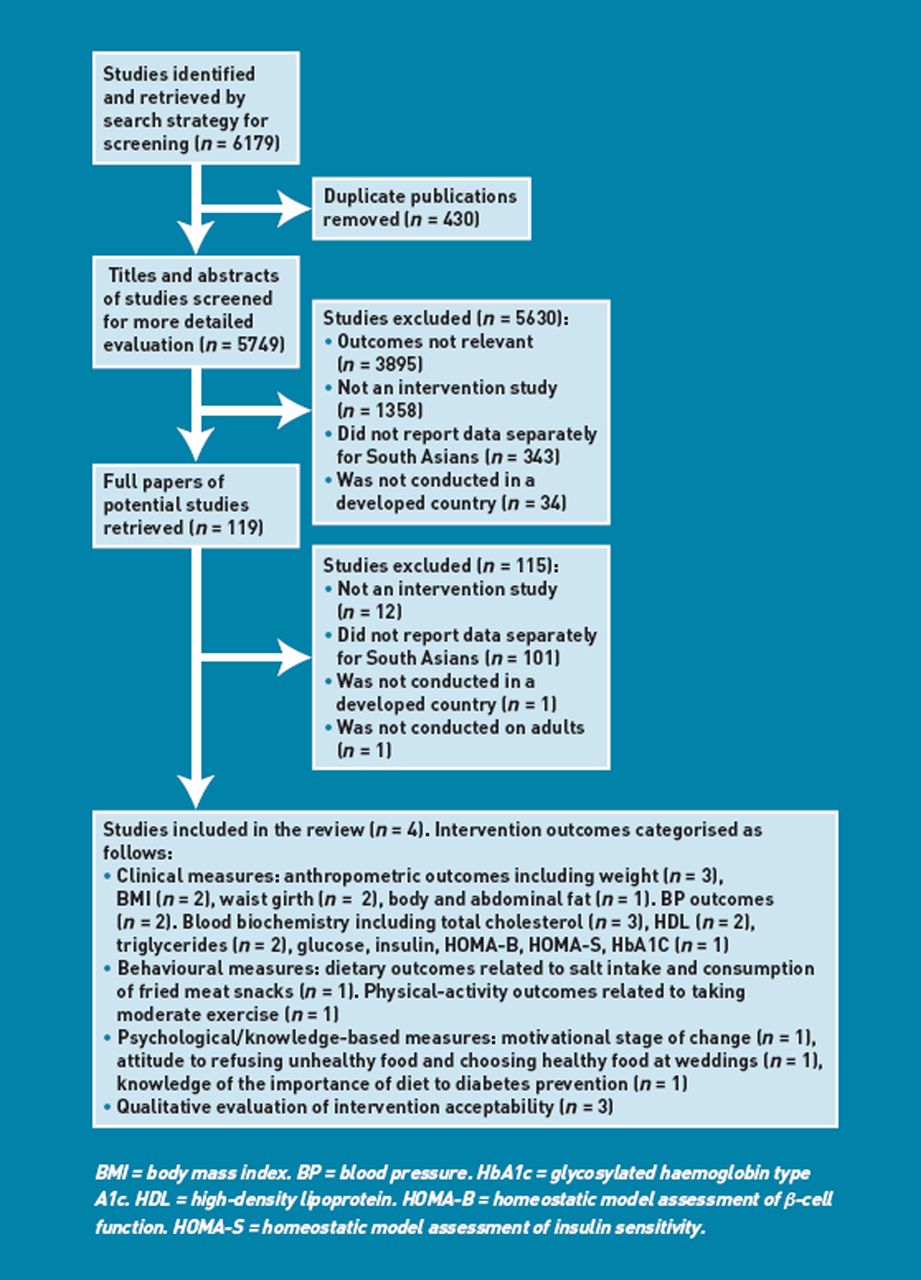
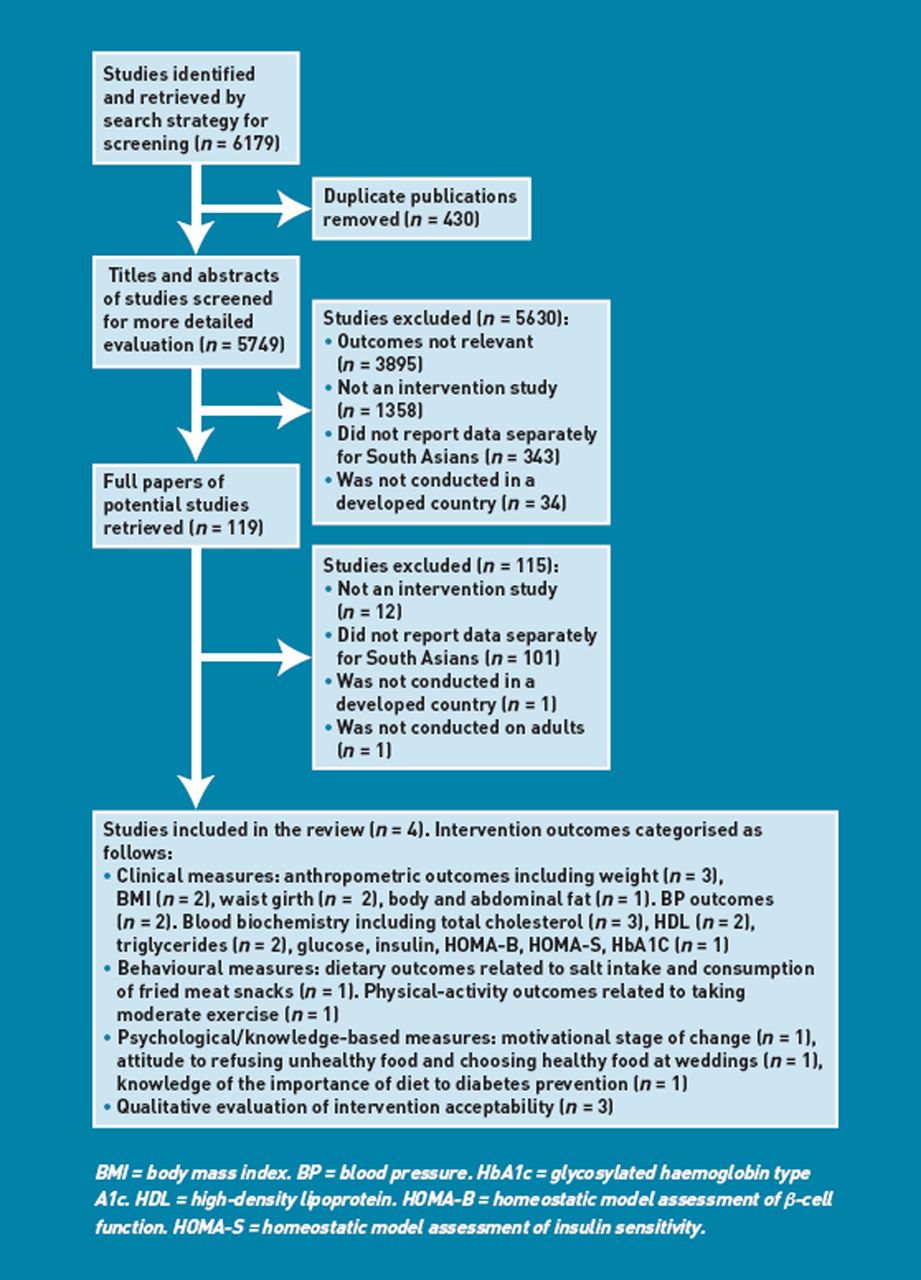{kind=link}
Flow chart for studies through stages of systematic review.
Details of the study characteristics and interventions are described in Table 1. Due to the small number of studies and considerable heterogeneity in intervention type, assessment, and outcome measures, meta-analyses were not feasible and a narrative synthesis was performed.20 The four studies included physical activity and/or dietary change as part of one-to-one and/or group educational interventions for CHD risk and/or diabetes, involving health visitors, bilingual link workers, or dietitians in community settings.21–24
Characteristics of included studies
All studies were uncontrolled before-and-after designs, except one randomised controlled trial.24 No studies reported using theoretical models to inform interventions, though one study21 measured participants’ stage of change.25 Reported methodological quality was generally poor, with total scores ranging from 41% to 56%19 (full data available from authors). The number of participants varied from 1323 to 201,24 involving people who were largely from South Asian communities; however, detailed descriptors beyond ethnicity or, in one study, education, were lacking. For reporting quality, higher scores were gained for adequately describing study aims, interventions, and participants, but only three of the four studies clearly described the main findings.21–23 Two studies reported exact significance levels for the main outcomes21,22 and one reported a sample-size calculation.24 External and internal validity and bias scores were low, with only one study reporting reliable compliance with the intervention.24 One study failed to score on the use of accurate, valid, and reliable main-outcome measures24 and reliability of secondary measures was poor. No studies adjusted for confounding in analyses, or reported on potential adverse effects, and only one provided a comparison group.24
Intervention effects
Clinical outcomes.
The clinical impacts of the interventions are summarised in Table 2. All four studies reported clinical outcomes, including changes to anthropometric measures, blood pressure, and/or blood biochemistry. All studies measuring changes in weight demonstrated a reduction in kilogrammes from baseline to follow-up, ranging from a 0.9% reduction over 6–12 months21 to 3.4% at 17 months.23 Waist girth in centimetres showed small percentage decreases of 0.621 and 2.1,22 and reductions in body and abdominal fat were also found.22 However, all reductions in weight, waist girth, and body and abdominal fat were significant for males only in one community-based, group-education intervention.22
Clinical outcomes of included studies
One study reported significant reductions in systolic blood pressure of 2.8%21 and two studies reported reductions in mean diastolic blood pressure of 3.9%21 and 3.9%22 (females only). Measures of blood biochemistry showed mixed results. Significant positive impacts on cholesterol (–3.7% over 6–12 months)21 were reported in one of three studies; increases in high-density lipoprotein were reported in another (9.5% females only, increases in males also approaching significance),22 and significant decreases in triglyceride levels (13.3%)21 were found in one of two studies. No significant changes were reported in glucose, insulin, homeostatic model assessment of β-cell function (HOMA-B), homeostatic model assessment of insulin sensitivity (HOMA-S), or glycosylated haemoglobin type A1c (HbA1c).
Behavioural outcomes.
Self-reported changes to dietary behaviour and physical activity were measured in one study21 (Table 3). Males and females reported significant improvements in salt intake and consumption of fried meat snacks following a CHD-prevention service.21 In relation to physical activity, an average of 49% of participants reported taking more moderate exercise (defined as ‘physical activity that makes one out of breath but not sweaty’) 6–12 months after intervention.21 Another study discussed specific dietary changes, such as increases in fish intake and cereal, following group activity and dietary-education sessions, but no data were reported from these measures.22
Behavioural outcomes of relevant included studies
Psychological and knowledge-based outcomes.
Table 4 shows the psychological and knowledge-based impacts of the interventions. In total, 50% of participants in one study showed an increase in the stage of change relating to motivation to address lifestyle behaviours after 6–12 months, in comparison with a decrease of 21% and 29% who stayed the same.21 With regard to attitude change, a single item about ‘finding it hard to refuse food at social events’ increased, and ‘choosing correct food at weddings’ showed a modest increase, but no significance data were reported.24
Psychological and knowledge-based outcomes and acceptability of included studies
Little evidence was demonstrated for knowledge-based changes following the interventions. Single items asking if the participant ‘agrees the importance of diet to diabetes prevention’ and the percentage of people ‘correctly identifying different food values’ showed small increases after 6 months, but no significance levels were reported.24
Intervention acceptability.
Three of the four studies presented data on the acceptability of programmes;21,23,24 these reported that interventions were positively valued and some participants felt empowered to control health issues following the programme.24 In one study, 69% of women attending community healthy-eating and exercise classes said they would recommend them to friends, and attended for social reasons as well as weight loss.23 Word of mouth by link workers or members of the community were the most popular methods of engagement.23 Prioritising the needs of families and a reluctance to walk to classes were barriers to attending group classes.
Exercise was popular, and women who had a large body mass index were more likely to want the intervention to continue.23 Participants wanted to keep materials such as audiotapes and flashcards following the interventions to use afterwards.24 Participants particularly valued the role of South Asian bilingual link workers and interpreters within programmes.23,24 One study anecdotally reported that changes were adopted by others in the community.22
DISCUSSION
Summary
Only four studies, all specifically involving South Asian communities alone, met eligibility criteria. Lack of controls in three, as well as inconsistency in measures and outcomes, meant it was not possible to pool data in a meta-analysis; as a result of this, firm conclusions about the effectiveness of the interventions that were assessed cannot be made. However, several insights and common themes can be offered from this review to inform future intervention development and research.
In relation to clinical outcomes, all programmes with combined physical activity and dietary change components reported decreases in weight where measured, but where the results were analysed by sex, changes in weight, waist circumference, and body and abdominal fat, these were only significant for men.22 The sex difference could relate to South Asian women from a variety of religious backgrounds being deterred from attending mixed-sex activities27 but, as programme engagement data were not provided, this cannot be ascertained. Mixed results were found for other clinical outcomes, with some reduction in blood pressure and blood lipid profiles, but no improvement, for example, in insulin sensitivity or resistance.
Participants in one study appeared to change dietary and activity patterns, but reliability of these behavioural outcomes was limited by use of single-item measures and self-reporting. Support for the efficacy of improving dietary knowledge was weak and no study measured knowledge of physical activity. One study suggested its community-based programme may encourage participants to progress through motivational stages of change,21 but this was reported in relation to general risk rather than specific behaviours.
Factors contributing to intervention engagement and acceptability
The involvement of trained bilingual community link workers appeared key to enhancing intervention acceptability and delivery in those studies that involved participants who were socially disadvantaged; for example, those from Pakistani and Bangladeshi communities, with significant proportions of participants across studies speaking little or no English.23,24 Qualitative feedback confirmed that, in addition to language skills, link workers were valued for their sensitivity and cultural understanding, which may have facilitated more meaningful and personal engagement in programmes. This finding is consistent with previous research suggesting that establishing relationships is important to the receptivity of lifestyle interventions in primary care.28
Programmes that were also promoted in the community and recruited by word of mouth appeared to generate more positive outcomes than those initiated from more formal healthcare settings, such as hospitals or clinics. Generating interest through local-community resources appeared to be beneficial due to the familiarity of the setting and the informal, social element of the meetings.23
Most programmes offered some form of personalised feedback, either in the form of one-to-one consultations or measurements of individual progress. This approach seemed to be potentially promising when accompanied by visual aids and handouts.21 Pictures and other visual aids were also valued and may help to overcome language and literacy barriers.22
Implications for research and practice
Many intervention studies that were identified had, or may have, included South Asian participants who were historically immigrant, but experiences that were distinguishable for South Asian individuals were not reported; as a result, only four studies met review criteria. Potentially important insights for enhancing appropriateness and implementation of interventions may be missed if relevant data are not reported when South Asian individuals are part of study populations. In addition to outcomes, information about participants’ engagement, language abilities, and social demographic, including deprivation and education status, may enable assessment of relevance and transferability. This is particularly pertinent for those South Asian communities that are more disadvantaged and at higher risk, where effective interventions are most needed and evidence is lacking.17
Three of the four studies reviewed appeared to have benefited from some prior qualitative work with target communities to inform intervention components; this may have been important to enhancing their acceptability.17,29 However, the quality of outcome data in the studies reviewed was generally poor, with a failure to consider potential confounders or adverse effects, and a lack of formal statistical-significance testing. All studies had flaws in internal validity, due to a lack of concurrent controls and data concerning programme compliance. Another common problem was a lack of standardised measures, particularly for behavioural, psychological, and knowledge-based outcomes. The majority of these measures lacked clear definition and appeared to be purpose designed, with no data available on piloting outcomes, validity, or reliability. Where possible, objective measures of behaviour, using standardised scales that have been validated in South Asian populations, are needed alongside clinical measures, as maintained behaviour change is necessary for sustained clinical benefit.
The importance of theoretical frameworks for evaluating complex interventions is increasingly recognised,29 but none of the studies designed their intervention with this in mind. Improving the effectiveness of lifestyle interventions requires an understanding of the causal techniques and procedures responsible for change.30 In the absence of a clear evidence base, progress is likely to be slow, with ‘wheels’ being reinvented rather than reapplied. All studies but one failed to measure the motivation of participants to change their lifestyles, which may account for the relative lack of intervention effects. Greater emphasis on combining targeted information with appropriate motivational techniques and specific behavioural guidance is needed. In addition, interventions may have been time and resource intensive in these studies, but no economic evaluation data were provided.
This review highlights a dearth of well-evaluated, community-based, physical activity, and dietary interventions for South Asian populations. Nevertheless, programmes were well received, suggesting that the potential to enhance physical activity and promote dietary change in these communities is considerable. Interventions that were reviewed may have resulted in some initial effects on health outcomes and offer useful first steps for enhancing health promotion in this group, which is at high risk of developing chronic disease. However, there remains much to be done to impact disease risk or morbidity, given the sustained and highly intensive interventions necessary to achieve this in other populations that are at risk. 9,10,13
Further research should focus on developing interventions that:
are informed by prior qualitative work with target communities;
incorporate a theoretical framework;
employ a robust methodology, with standardised and objective measures;
target education and behavioural motivation; and
provide a comparison group to assess effectiveness when naturally occurring change is controlled.
Approaches, particularly for South Asian populations that are socio-educationally deprived, may usefully build on current experience by using community-based programmes in a familiar environment with trained, bilingual community link workers. Interventions that include feedback and audiovisual media seem to be well received. Health–economic analyses should be performed alongside future experimental studies to ensure that promising preventative health programmes in these high-risk groups are cost effective and can be feasibly implemented.
Acknowledgments
We thank Wendy Stanton for her review of the search strategy; Caroline Mulvaney, Mandeep Bhoday, and Helena Tuomainen for contributions to review development and searches; Julie Moss for administrative support; and Tracey George for managerial support.
Notes
Funding
This review was funded by a National Institute for Health Research Collaboration in Applied Health Research and Care (Nottinghamshire, Derbyshire and Lincolnshire) grant. The funders had no role in the study design, data collection or analysis, decision to publish, or preparation of the manuscript.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received April 23, 2012.
- Revision received June 26, 2012.
- Accepted August 21, 2012.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
More in this TOC Section
Related Articles
Cited By...

