


Abstract
Background Antibiotic resistance is a growing concern and antibiotic usage the main contributing factor, but there are few studies examining antibiotic use and resistance in children.
Aim To investigate the association between previous trimethoprim prescribing and resistance in urinary Escherichia coli (E. coli) isolates in children.
Design and setting Retrospective, population cohort study in Tayside, Scotland.
Method Multilevel modelling of linked microbiology and dispensed prescribing data for 1373 ≤16-year-olds with E. coli urinary isolates in 2004–2009, examining the association between prior trimethoprim prescription and subsequent trimethoprim resistance in people with urinary E. coli isolates.
Results Trimethoprim resistance was common (26.6%, 95% confidence interval [CI] = 24.6 to 28.6). Previous trimethoprim prescription was associated with subsequent culture of trimethoprim-resistant E. coli, with more recent prescription being more strongly associated with resistance. After adjusting for the number of previous E. coli isolates and sample year, trimethoprim prescribing in the previous 84 days remained significantly associated with culturing trimethoprim-resistant E. coli (adjusted OR 4.71, 95% CI = 1.83 to 12.16 for the previous 15–28 days versus never prescribed; adjusted OR 3.16, 95% CI = 1.63 to 6.13 for the previous 29–84 days); however, associations were not statistically significant for longer periods since prior exposure.
Conclusion Trimethoprim prescription has implications for future resistance in individual children, as well as at population level. Clinicians must ensure appropriateness of treatment choice and duration, and alternative antibiotics should be considered for childhood urinary tract infections if trimethoprim has been prescribed in the preceding 3 months.
- anti-bacterial agent
- child
- child, preschool
- general practice
- infant
- trimethoprim resistance
- urinary tract infections
INTRODUCTION
Increasing antibiotic resistance is a major threat to public health worldwide.1 Infection with a resistant organism is associated with adverse outcomes for individuals, such as increased length of hospital stay and mortality, placing a burden on many health systems. In primary care, infection with resistant organisms is associated with greater duration of symptoms, increased GP workload, and increased costs.2,3 Antibiotic usage has been identified as the main contributing factor to the development of antibiotic resistance, and improving the prudent use of antibiotics or antibiotic stewardship is a policy priority.1,4,5
At country level, higher use of antibiotics is associated with higher rates of resistance,4 and a similar relationship has been shown in adults at individual level in a recent systematic review and meta-analysis.6 Costelloe et al examined the association between antimicrobial resistance and previous antibiotic prescription, and found that prior antibiotic exposure was associated with higher rates of resistance. Although this association weakened as time since exposure increased, it remained statistically significant for antibiotic use up to 12 months before the infection being examined.6 For urinary tract infection (UTI), several studies in adults have shown that antibiotic resistance is significantly associated with previous individual exposure to antibiotics.6–10
Most studies of the association between prior antibiotic exposure and antibiotic resistance are carried out in adults rather than children. In children, Gruneberg and Shaw found a positive association between previous antibiotic prescribing and resistance patterns in coliform UTI.11 This finding is, however, based on only 35 children attending hospital, and prescribing and resistance patterns are likely to be different in primary care. A more recent study found that trimethoprim resistance in urinary isolates in children rose from 25% to 34% between 2002 and 2008, and recommended that UK laboratories monitor urinary-resistance patterns so clinicians prescribe antibiotics that are associated with less resistance.12 UTI is the second most common indication for empirical antibiotic treatment in children and, although many infections are not formally diagnosed, the National Institute for Health and Clinical Excellence (NICE) in the UK estimates that one in 10 girls and one in 30 boys will have a UTI during childhood; not all, however, will be recognised or proven by culture.13 Recurrent infection in children is relatively common,13,14 and many children are at risk of repeated antibiotic exposure for the same indication. This study, therefore, aimed to examine the relationship between primary care trimethoprim prescribing and Escherichia coli (E. coli) trimethoprim resistance in all urinary isolates in children resident in a defined geographical area.
How this fits in
This is the first population-based study in children examining the relationship between prior trimethoprim exposure and resistance in urinary tract infections (UTIs); the findings show a strong time-dependent association, with prescription in the preceding 3 months significantly associated with increased resistance. The findings emphasise that antibiotic prescribing has important implications for resistance in the individuals for whom prescriptions are written, and that an alternative antibiotic should be considered for the treatment of suspected childhood UTI if trimethoprim has been prescribed in the preceding 3 months.
METHOD
Study design
The overall design was a cohort study, using linked retrospective data, of all residents in Tayside, Scotland, aged ≤16 years with E. coli isolated from urine samples. Fully anonymised data were provided by the University of Dundee’s Health Informatics Centre (HIC). A linked dataset was created using the Community Health Index number: a unique patient identifier used in all healthcare settings, including microbiology, in Tayside. From 2004 to 2009 inclusive, data were extracted for all urine samples from people aged ≤16 years with a pure E. coli growth ≥104 colony-forming units/ml, and where trimethoprim sensitivity/resistance was reported (a standard test for all suspected UTIs). These was linked to data for trimethoprim prescriptions dispensed between 1993 and 2009, as well as being linked to demographic data. To avoid double counting unresolved infection that was reinvestigated, urine samples were excluded if E. coli had been isolated from a urine culture in the previous 28 days.
Statistical analysis
As individual patients could have multiple samples, univariate and adjusted odds ratios (ORs) for the presence of trimethoprim resistance were calculated using multilevel logistic regression to account for the repeated measures nature of the data. A two-level model of samples within patients was used. Sample-level variables included:
age at test;
time since most recent previous trimethoprim prescription; and
year of the test.
Patient-level variables included sex, socioeconomic status (based on the Scottish Index of Multiple Deprivation — a postcode-derived measure of socioeconomic deprivation15), rurality (based on the Scottish Executive Urban–Rural Classification, which is based on settlement size and distance from large urban areas), and the total number of E. coli urinary isolates in the study period. Initial data management and analysis was conducted using PASW Statistics (version 18.0) and multilevel modelling using Stata Intercooled (version 11).
Ethics
Study-specific ethics approval was not needed as data linkage, anonymisation, and analysis were carried out under HIC Standard Operational Procedures, which have been approved by the East of Scotland NHS Research Ethics Committee and the Tayside Caldicott Guardian; as such, individual study review was not required.
RESULTS
Sample characteristics and main findings are summarised in Table 1. In total, 1855 urine samples with a pure E. coli growth from 1373 patients were included, of whom 88.9% were female. For the majority (82.6%) of patients, this was their first E. coli urinary isolate during 2004–2009; 50.9% of samples included were from patients who had never been prescribed trimethoprim, with prior exposure for the remainder occurring over a wide spread of times. For most samples from patients who had previously been prescribed trimethoprim, exposure had occurred more than a year before; just over 10% had been exposed in the 28 days before culture.
Sample characteristics and associations between trimethoprim prescription and trimethoprim resistance
Over the whole period of analysis, 26.6% (95% confidence interval [CI] = 24.6 to 28.6) of included E. coli isolates were trimethoprim resistant, rising from 19.0% in 2004 to 33.3% in 2009 (univariate OR 2.46, 95% CI = 1.19 to 5.08). Resistance was less common in boys than girls, although this difference was not statistically significant (21.1% versus 27.2%, univariate OR 0.62, 95% CI = 0.34 to 1.14). This did not vary with rurality or age. Patients with four or more E. coli isolates in the study period were considerably more likely to have trimethoprim-resistant E. coli compared with those with only one (45.5% versus 20.8%; univariate OR 5.18, 95% CI = 2.79 to 9.59). Patients who had previously been prescribed trimethoprim were more likely to have resistant E. coli than those who had not, with the highest rates of resistance in those who had been prescribed trimethoprim most recently: 20.3% (95% CI = 17.7 to 22.9) of those never prescribed trimethoprim had a resistant E. coli isolated, compared with 43.1% (95% CI = 29.4 to 56.9) of those prescribed it in the 15–28 days before the index sample and 45.0% (95% CI = 36.5 to 53.6) of those prescribed it 29–84 days before. Rates of resistance then progressively fell; when previous exposure had been >365 days before the index sample, there was little difference in resistance rates.
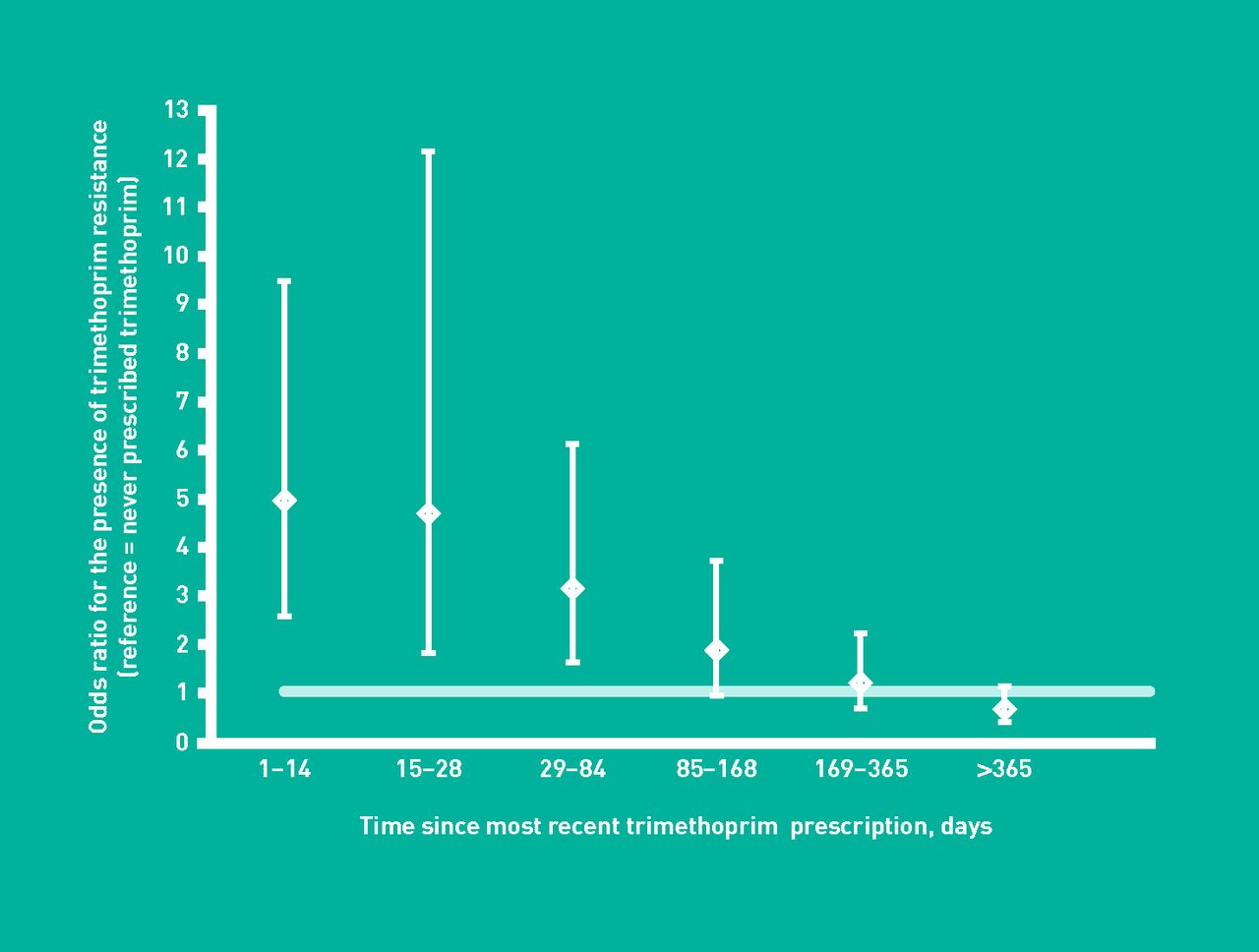
Table 1 also shows ORs from the multivariate multilevel model. In the adjusted model, only three variables were significantly associated with trimethoprim resistance: the number of E. coli urinary isolates over the whole period; the sample year; and prior trimethoprim prescription. Adjustment for other variables attenuated the strength of the univariate associations with number of urinary isolates and prior trimethoprim prescription, and somewhat increased the strength of the univariate association with year of sample. Trimethoprim prescription in the previous 84 days remained significantly associated with having a trimethoprim-resistant E. coli (adjusted OR for 1–14 days, 15–28 days, and 29–84 days groupings: 4.97 [95% CI = 2.60 to 9.49], 4.71 [95% CI = 1.83 to 12.16], and 3.16 [95% CI = 1.63 to 6.13] respectively), but associations were not significant for longer periods since prior exposure (Table 1).
DISCUSSION
Summary
This study found a time-dependent relationship between prior trimethoprim prescription and resistance in E. coli isolates from urine samples in children. Resistance was significantly higher in children who had been prescribed trimethoprim in the previous year in univariate analysis, with stronger associations for more recent prescriptions. There were no significant associations with age, sex, deprivation, or rurality in the adjusted model, but there was a time-dependent association: prior trimethoprim prescription was significant for prescriptions that had been given in the preceding 84 days.
Although the study found a highly significant association between previous trimethoprim prescription and trimethoprim resistance, it should be noted that 20.3% of samples from patients who had never previously been prescribed trimethoprim also cultured trimethoprim-resistant E. coli. This may be driven by mean population rather than individual antibiotic prescribing, intrafamilial spread of antibiotic resistance, travel, and consumption of food contaminated with resistant coliforms.8
Strengths and limitations
The strengths of the study are that it uses a complete population dataset, including all community-dispensed prescribing and all microbiology-laboratory urine cultures for a defined geographical population, making it the largest such study, to the authors’ knowledge, that has been conducted with children.6 However, as in all routine data analyses, there are a number of potential weaknesses.
There are no data on hospital prescribing of antibiotics, although the analysis does include prescribing by out-of-hours primary-care services. In addition, there are no data on whether children had an underlying anatomical abnormality predisposing them to complicated UTI, although the inclusion of the variable for total number of positive urine cultures in the 5-year period may partially account for this in the analysis. Many episodes of UTI in children will be treated empirically, and it is notable that many more children in this study had received prior trimethoprim than had prior documented UTI. As such, samples may be more likely to be sent for laboratory culture when an empirical course of antibiotics has failed because the organism being treated is already resistant. Interpretation of the association between resistance and trimethoprim prescribing in the preceding 14 days should, therefore, be undertaken with caution. Although the prescription of trimethoprim in the 85–365 days before UTI was not significantly associated with resistance in the adjusted model, there does seem to be a persistent dose–response relationship (Figure 1) and lack of significance for antibiotic exposure in this period may be due to lack of power. A further weakness is that, although the prescribing data are for dispensed prescriptions; that is, the parent or child has collected the antibiotic from a community pharmacist, some dispensed prescriptions may not actually be taken. Finally, the study did not examine exposure to other antibiotics. There is some evidence that prescription of other antibiotics can be associated with resistance to trimethoprim,8 although the most recent systematic review did not find a consistent relationship.6 However, as most of these weaknesses would likely bias the results to the null, these findings are reasonably robust.
{kind=link}
Adjusted odds ratio for trimethoprim resistance in relation to prior trimethoprim exposure.
Comparison with existing literature
The results of this study are consistent with similar studies in adults, although the odds of resistance associated with previous trimethoprim exposure are somewhat larger.8–10 Smaller studies have also shown that resistance in urinary isolates is more common in people who are treated with antibiotics in the previous 3 months.10 In the largest single study in adults using the same datasets as used in this analysis, Donnan et al showed that the risk declined over time, as found here, but that it was persistent for up to 6 months after prior antibiotic exposure.9 The most recent systematic review and meta-analysis for urinary isolates was largely based on adult studies, but found a consistent association between prior antibiotic exposure and subsequent resistance that persisted for up to 1 year.6
Implications for practice
This study is the largest such analysis to date in children. Its findings show that trimethoprim prescription in children has implications for future resistance in their urinary isolates, as well as likely effects on overall resistance rates at population level.1,6 These results suggest that an alternative antibiotic should be considered in cases of childhood UTI if trimethoprim has been prescribed in the previous 3 months; for this to be achievable, it is important that all antibiotic prescriptions, including out-of-hours and hospital prescriptions, are clearly recorded in the primary care medical record.
At a more general level, implementing the recommended monitoring of local resistance patterns and communication of these to prescribers is required to ensure that clinicians make rational choices of antibiotics.12 Although in vitro resistance is not necessarily associated with lack of in vivo response, UTI caused by resistant E. coli in primary care is associated with greater duration of symptoms, increased GP workload, and increased costs.2,3 Clinicians must, therefore, be ‘prudent prescribers’16 and ensure appropriateness of antibiotic choice and length of treatment when bacterial infection is proven or highly likely. Although empirical treatment of a suspected UTI may be indicated in a sick child,13 clinicians should minimise empirical antibiotic use by following guideline recommendations for the diagnosis of UTIs in children wherever possible. NICE guidelines recommend urine culture for all children aged <3 years with suspected UTI and for those aged ≥3 years when dipstick testing is equivocal (only one of leukocyte esterase or nitrite testing is positive). Although both leukocyte esterase and nitrite dipstick positivity is considered diagnostic of UTI in those aged ≥3 years, culture is indicated ‘if a child has a high or intermediate risk of serious illness and/or a history of previous UTI ...’, which will include most children with a previous trimethoprim prescription and in whom the risk of resistance is higher.13
Use of antibiotics varies considerably between countries, localities, and practices.4,9,17,18 There is evidence that educational interventions can reduce antibiotic use,19 and that reducing their use at country20,21 and practice level18 is associated with subsequent lower rates of resistance. There is a need for further research to examine how individual, household, and community exposure to antibiotics is associated with resistance, and the extent to which interventions to reduce antibiotic prescribing also reduce antibiotic resistance.
Acknowledgments
We acknowledge the support of the Health Informatics Centre, University of Dundee for managing and supplying the anonymised data, as well as the original data source, NHS Tayside. We also acknowledge the approval of Tayside Academic Health Sciences Centre for Research and Development to carry out this project, and would like to thank Dr Gabby Phillips (consultant microbiologist at NHS Tayside) for her advice on defining ‘culture-proven UTI’.
Notes
Funding
The study was carried out as a fourth-year medical student project by Mary Duffy and received no external funding.
Ethical approval
The East of Scotland Research Ethics Service has stated that projects such as this one, which only use fully anonymised data that are provided and managed under University of Dundee’s Health Informatics Centre Standard Operating Procedures, do not need individual review.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
The authors have declared no competing interests.
Discuss this article
Contribute and read comments about this article on the Discussion Forum: http://www.rcgp.org.uk/bjgp-discuss
- Received October 6, 2012.
- Revision received October 22, 2012.
- Accepted November 27, 2012.
- © British Journal of General Practice 2013
REFERENCES
In this issue









Jump to section
Keywords
More in this TOC Section
Related Articles
Cited By...

